


Abstract
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoma entity whose prognosis for high-risk patients is poor. Aggressive salvage treatments to improve patient outcome have been unsatisfactory. Therefore, we evaluated the efficacy of yttrium-90-ibritumomab tiuxetan (Zevalin®; 90Y-IT) consolidation after early salvage chemotherapy with autologous stem cell transplantation. Thirty-seven patients with intermediate-high risk DLBCL not in complete remission (CR) after three cycles of rituximab, cyclophosphomide, doxorubicin, vincristine and prednisone (R-CHOP) were assessed retrospectively. After early salvage treatment, 70% achieved CR and 30% partial remission. Twenty patients underwent additional consolidation with 90Y-IT. During the 3-year follow-up, 50% in the 90Y-IT-treated group experienced relapse compared to 82.3% in the other cohort (p=0.002). Progression- and disease-free survival were significantly longer in the 90Y-IT group. However, probably due to the relatively short follow-up period, no difference in overall survival was observed. 90Y-IT consolidation after early salvage chemotherapy improves treatment responses and reduces the percentage of relapses without significant additional toxicities.
Diffuse large B-cell lymphoma (DLBCL) is the most common aggressive lymphoma subtype, accounting for approximately 25-30% of new cases of non-Hodgkin's lymphoma (NHL) (1). Combination therapy with cyclophosphamide, doxorubicin, vincristine and prednisone (CHOP) has been considered the gold standard for more than 25 years (1). Nevertheless, estimated progression-free survival (PFS) and overall survival (OS) at three years were only 40% and 50%, respectively. In the past decade, the addition of rituximab (R-CHOP), a chimeric monoclonal antibody to the protein CD20, has led to an outstanding survival improvement for patients with DLBCL, which is why R-CHOP has become the new standard-of-care for this aggressive disease (2, 3). Despite this approach, due to the high percentage of relapses, the prognosis for patients with high-risk DLBCL, namely those with an elevated International Prognostic Index (IPI), bulky disease, involvement of the central nervous system or testes, is still poor, with a 5-year OS of less than 50% (4). Current salvage treatments, including autologous stem cell transplantation (ASCT), are not able to cure most patients (5). Thus, since first-line treatment intensification (6-8) has not improved outcome, new salvage strategies are needed and the addition of radioimmunotherapy could be a valid option. Indeed, it has proven to be efficient in relapsed/refractory aggressive DLBCL (9-11). However, preliminary results of therapy with yttrium-90-ibritumomab tiuxetan (Zevalin®; 90Y-IT) after ASCT are conflicting and the analyzed cohorts were too small to draw any conclusions (12, 13).
Herein, we provide the first direct comparison of patients with intermediate/high-risk DLBCL after early salvage treatment including ASCT who either underwent 90Y-IT consolidation or did not.
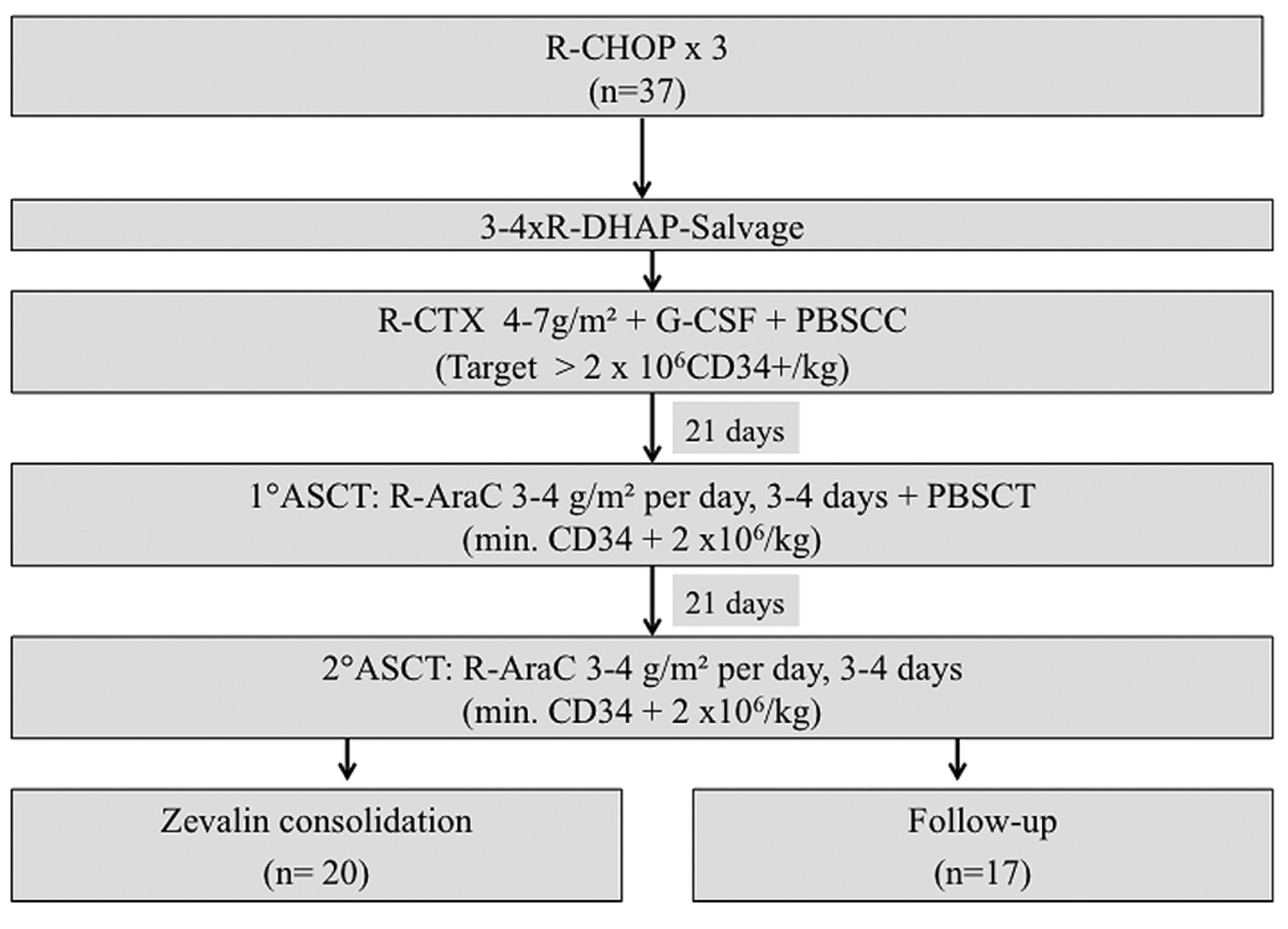
Treatment algorithm.
Patients and Methods
Patients. From July 2006 to September 2012, all 37 consecutive patients affected by intermediate/high-risk DLBCL indicated for early salvage treatment were retrospectively assessed at the G. Martino University Hospital in Messina. A histological review according to the current WHO classification (14) was performed on all cases at the Seràgnoli Istitute of Hematology, University of Bologna. As required by the inclusion criteria, all patients had stage III/IV disease, an IPI >1 (15) and a performance status <3. Consolidation with 90Y-IT was proposed to all patients who were considered fit enough, regardless of the type of response to treatment. Overall, 20 patients agreed to treatment intensification, while the others did not and were considered as a control group.
The local Ethical Committee approved this analysis (Prot. E 49/13) and all patients were required to sign an informed consent form.
Treatment plan. None of the 37 patients achieved a complete response (CR) after three cycles R-CHOP-21 (16 patients with partial response (PR), 21 patients with stable disease (SD)) which is why they underwent early salvage immuno-chemotherapy with three or four cycles of R-DHAP (rituximab, cisplatin, cytarabine, dexamethasone) (5). Successive stem cell mobilization consisted of cyclophosphamide (4-7 g/m2) on day +1, rituximab (375 mg/m2) on day +2 and lenograstim 5 μg/kg die from day +3 until stem cell collection (Figure 1). In cases of insufficient harvest (<9×106 CD34+ cells/kg), additional leukapheresis was performed after mobilization with cytarabine (3-4 g/m2 days 1-4) and lenograstim 5 μg/kg from day +5 die until stem cell collection. Three weeks after stem cell collection, all patients underwent three tandem high-dose cytarabine administrations (12 to 24 g/m2, every 21 days), followed by rituximab and reinfusion on day +2 of at least 2×106/kg CD34+ cells (16, 17). Six to 10 weeks after ASCT, 20 patients received an additional consolidation treatment with 90Y-IT, while the remaining 17 did not. 90Y-IT was administered according to the international standard, namely rituximab at 250 mg/m2 on day 1 and on day 8 followed by 14.8 MBq (0.4 mCi)/kg of 90Y-IT after the last rituximab dose. In order to prevent infectious complications, patients routinely received granulocyte colony-stimulating factor once their total white blood cell count was ≤2,000/mm3 until full recovery and erythropoietin was administered when the hemoglobin decreased to less than 10 g/dl. Antibiotic and antifungal prophylaxis was also administered.
Patients' characteristics.
Treatment response was assessed after three cycles of R-CHOP, after ASCT and after 90Y-IT where applicable. It consisted of a complete physical examination, blood testing, bone marrow aspirate and biopsy in case of bone marrow involvement at diagnosis, as well as Positron emission tomography-computed tomography (18).
Statistical analyses. Chi-square test was performed to assess the significance of differences between categorical variables. OS, PFS and disease-free survival (DFS) were plotted as curves using the Kaplan–Meier method and were defined as the time from diagnosis until death from any cause, as time from diagnosis until disease progression or death from any cause, and as time from the achievement of a CR to relapse or death as a result of lymphoma or acute toxicity of treatment, respectively (18). Log-rank test was employed to assess the impact on survival of categorical variables. A p-value of <0.05 was considered as statistically significant. Statistical analyses were performed with the Statistical Package for the Social Sciences (SPSS) software v.17.0.1 (SPSS, Chicago, IL, USA), MedCalc (version 11.0; MedCalc Software Acacialaan, Ostend, Belgium) software and the GraphPad Prism (version 5.0; GraphPad Software, Inc., San Diego, CA, USA) package.
Results
Clinical characteristics at time of diagnosis. Overall, the median age at time of diagnosis was 54.3 years (range=34-64 years). A female predominance was observed (20/37, 54.1%). As required by the inclusion criteria, all patients had stage III/IV disease. Twenty-nine patients (78.3%) had B symptoms and lactate dehydrogenase was elevated in 34 patients (91.8%). Only a minority (13; 35.1%) had bulky disease (Table I). Except for extranodal disease that prevailed in the 90Y-IT-treated group (100% vs. 72%; p=0.011), clinical features at the time of diagnosis were similar in the two treatment groups and no statistically significant differences were observed (Table I).
Treatment response according to therapy.
Treatment and response. After three cycles of R-CHOP-21, 16 patients achieved a PR, and 21 had SD. Hence, early salvage immunochemotherapy with R-DHAP was initiated. As mentioned above, stem cell collection was performed with lenograstim after the last cycle and a median number of 3.15×106/kg CD34+ cells (range=2.01-4.10×106/kg) was harvested in the 90Y-IT group compared to 3.03×106/kg CD34+ cells (range=2.01-4.90×106/kg) in the other one. Only three patients had a sufficient CD34+ cell harvest after cyclophosphamide and therefore the remaining 34 patients underwent a second mobilization with high-dose cytarabine with peripheral blood stem cell collection. After three tandem ASCTs, 20 patients agreed to 90Y-IT consolidation: seven of them were in CR and 11 in PR, while the remaining were in CR and refused treatment intensification. After 90Y-IT, all 20 patients were in CR (Table II). After completion of the whole program, four out of five in the second group with initial high-risk achieved CR and one a PR.
Consolidation with 90Y-IT was well-tolerated. Reversible hematological toxicity, mainly consisting of grade 3 neutropenia and thrombocytopenia, occurred in eight patients (40%). Not a single case of febrile neutropenia was registered. Five patients (25%) developed grade 2 anemia. Transfusions of platelets or red blood cells were not required. About half of the patients experienced only mild-to-moderate fatigue following 90Y-IT consolidation therapy. Of note, no case of thyroid dysfunction or secondary malignancy occurred. There were no treatment-related deaths.
Relapse and status at the last follow-up according to treatment.
Follow-up. After a median DFS time of three years (range=8-36 months), 22/37 (59.4%) patients eventually experienced disease relapse: 10/20 (50%) in the 90Y-IT-treated group and 12/17 (70.5%) in the other group (p=0.002). Overall, 21 of them underwent further treatments. The median response duration differed significantly between both groups, 52 months in the 90Y-IT-treated group and 25 in the other (p=0.001). At the last follow-up, 15 patients were alive in CR, 13 with disease and nine died with disease. (Table III) Treatment intensification significantly prolonged median DFS (4.3 years versus 2.0 years, p=0.001) and PFS (5.1 years versus 2.7 years, p=0.007; Figure 2A and B). However, probably due to the relatively short follow-up period, no difference in OS was observed (Figure 2C).
Discussion
The role of 90Y-IT consolidation after salvage chemotherapy with ASCT in patients with high-risk DLBCL has not yet been established, although it influences positively the outcome in patients with relapsed/refractory DLBCL (10, 19). Herein, we provide evidence that 90Y-IT consolidation after salvage treatment clearly reduces the percentage of relapses and improves PFS and DFS in these patients.

Kaplan–Meier analysis of disease-free survival (DFS) (A; p=0.001), Progression-free survival (PFS) (B; p=0.007) and Overall survival (OS) (C; p=0.507) according to Zevalin ® consolidation.
The strengths of the present analysis were the central histological revision and the homogeneous treatment, although these patients were treated outside a clinical trial. The main limit of our study was its retrospective nature.
90Y-IT consolidation was able to induce a CR in all patients who were in PR (55%) after salvage chemotherapy and ASCT. A similar experience was published by Ria et al. who administered 90Y-IT as consolidation therapy to seven patients with high-risk NHL and residual disease after at least three months from ASCT and five patients achieved a CR with minimal additional toxicity (13). In a recent phase II trial, Han et al. evaluated the efficacy and safety of tandem consolidation with 90Y-IT and HDCT with ASCT in 11 patients with high-risk DLBCL and with at least a PR after induction (12). In contrast to our data, none of the five patients with PR converted to CR after 90Y-IT but they suffered disease progression. However, since no adequate salvage therapy was administered before 90Y-IT consolidation the informative value of these data is limited.
In the present study, 90Y-IT was very well tolerated and no patient experienced life-threatening toxicity. Adverse events were limited to neutropenia and thrombocytopenia, both grade 3, (n=8; 40%) and grade 2 anemia (n=5; 25%). Of note, no case of febrile neutropenia was observed. However, previous trials (12, 20) reported a much higher hematological toxicity rate, most likely due to the large number of previous treatment lines.
Y90-IT consolidation after ASCT led to a significant increase in the duration of response because the median DFS was significantly higher in this group (4.3 years) when compared to the control cohort (2.0 years; p=0.002). This could be explained by better disease eradication by radioimmunotherapy. These results are in line with what was reported by Ria et al. who recorded a median response duration of four years (range=2-5 years) (13). However, in the trial by Han et al. during the median follow-up period of 18.1 months, nine out of 11 patients (82%) suffered disease progression (12). In the present analysis, PFS also differed significantly between the groups, suggesting that 90Y-IT not only reduces the risk of relapse but also the number of deaths. Indeed, OS was clearly longer in patients who underwent 90Y-IT consolidation, without achieving statistical significance. The relatively low number of patients assessed for this analysis could explain this observation. Again, our data in contrast with those published by Han et al (12) who reported a detrimental PFS and OS.
In conclusion, 90Y-IT consolidation after salvage chemotherapy is able to improve treatment response, reduce the percentage of relapses and improve PFS and DFS. Therefore 90Y-IT might be able to eliminate minimal residual disease, at least in some cases. However, these data have to be confirmed in a prospective trial.
Acknowledgements
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
Footnotes
-
↵* Present address: Lymphoma Department, Memorial Sloan Kettering, NY, U.S.A. Tel: +1 9173535554, e-mail: mondellp{at}mskcc.org
- Received May 28, 2014.
- Revision received July 5, 2014.
- Accepted July 7, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.