


Abstract
Background: Gc protein-derived macrophage-activating factor (GcMAF) occurs naturally in the human body. It has various functions, such as macrophage activation and antitumor activities. Recently, immunotherapy has become an attractive new strategy in the treatment of cancer. GcMAF-based immunotherapy can be combined with many other therapies. Sonodynamic therapy (SDT) using low-intensity ultrasound is a novel therapeutic modality. Ultrasound has been demonstrated to activate a number of sonosensitive agents allowing for the possibility of non-invasive targeted treatment for both superficial and deep-seated tumors. The current case study demonstrates that GcMAF and SDT can be used in combination with conventional therapies in patients with metastatic cancer, especially where treatment options are limited due to factors such as toxicity. This case study also suggests a new concept of cancer treatment using local destruction of cancer tissue, in this case conducted with SDT, to be used in combination with GcMAF immunotherapy as a systemic treatment.
Immunotherapy has become an attractive new strategy in the treatment of cancer, due in part to minimal toxicity and an excellent safety profile when compared to conventional therapies such as chemotherapy and radiation.
Gc protein-derived macrophage-activating factor (GcMAF). Macrophages are important phagocytic cells that internalize and destroy pathogens and release cytokines. In addition, macrophages are known to play critical roles in antitumor immunity. They can infiltrate into tumors and are found in most tumor sites. GcMAF was first developed by Dr. Nobuto Yamamoto in 1991 (1), suggesting that it can be used as an important immunotherapy for cancer treatment (2-7). In previous studies, Gc protein (1f1f subtype) was isolated from human serum using an affinity column modified with 25-hydroxyvitamin D3. GcMAF was then prepared from this isolated Gc protein by an artificial enzymatic method (8). The process of separating Gc protein from serum leads to a much lower concentration, stability and activity of the final GcMAF that is produced. Additionally, re-use of the affinity column must be avoided because of cross-contamination between different serum samples. To overcome the problems associated with isolating Gc protein from serum in the production of GcMAF, we prepared de-galactosylated/desialylated human serum, which we coined serum GcMAF or second-generation GcMAF. Second generation GcMAF has a higher concentration (1,500 ng/0.5 ml) and longer stability because of this new manufacturing process, demonstrating that the 25-OH vitamin D affinity column is not necessary (Table I). Saisei Mirai developed a second-generation GcMAF in 2011, in collaboration with Dr. Hitoshi Hori and Dr. Yoshihiro Uto at Tokushima University (9). In addition to the higher concentration and stability, it has several other important properties, which include increasing phagocytic activity of macrophages (10), superoxide radical generation (11), anti-angiogenic effects (12), and antitumor effects (13). Increases in the number of monocytes and monocyte percentage in the blood have been observed in many patients during GcMAF therapy. In addition, serum GcMAF has been shown to increase the maturation of dendritic cells in vitro (unpublished data). By March 2014, Saisei Mirai will have treated more than 1,000 patients with GcMAF, both with and without conventional therapies, proving its safety as a therapy.
Comparison between first- and second-generation Gc protein-derived macrophage-activating factor.
Sonodynamic therapy (SDT). There is an ever-increasing amount of data showing that SDT, which refers to the use of low-intensity ultrasound with a sonosensitizer, can be used to produce free radical oxygen (14) to selectively destroy cancer cells (15, 16, 17). The concept of SDT consists of introducing a substance into the body that preferentially accumulates in cancer cells (15). This substance is then activated by ultrasound vibration instead of light stimulation, in contrast to traditional photodynamic therapy using a light-activated sensitizer. Since ultrasound is capable of passing completely through the body, the concept of destroying cancer cells without using damaging invasive procedures becomes possible. It also has the ability to destroy metastases in most places in the body, making it a very versatile and important therapy. SDT is considered to be a promising new modality for cancer treatment, without causing serious side-effects. Numerous sensitizers with various properties are being developed in a number of countries around the world. Recently, new sonosensitizers which only respond to ultrasound have been developed in Japan (14). This allows for the treatment of patients without light toxicity, which can be sustained during exposure to natural sunlight while the sensitizer remains in the body.
Ozone autohemotherapy and hyperbaric oxygen therapy. Tumor hypoxia, in which the tumor is deprived of an adequate oxygen supply, is a well-recognized factor in cancer treatment resistance to chemotherapy and radiotherapy as well as SDT, which requires production of oxygen-free radicals in order to be effective (15). Therefore any method of increasing oxygen supply within the tumor environment should increase the efficacy of SDT (15). Ozone therapy is a medical treatment that is used to increase the amount of oxygen in the blood. It is achieved by ozonating the patient's own blood outside the body and injecting it back into the body within a relatively short amount of time. Hyperbaric oxygen therapy is the medical use of oxygen at levels higher than atmospheric pressure. The equipment used for hyperbaric oxygen therapy consists of a pressure chamber and a means of delivering pure oxygen. In clinical situations, SDT is usually combined with ozone autohemotherapy to improve local hypoxia within the tumor environment.
Case Report
A 55-year-old female was diagnosed with breast cancer (left side, with skin invasion) in August 2009. She was treated by lumpectomy, with no chemotherapy or radiotherapy. She refused further standard treatment after the operation. The tumor was estrogen (ER)-, progesterone (PR)-, and Herceptin receptor (HER2)-positive. In October 2011, she noticed a right axillary tumor. At that time no treatments had been undertaken. The tumor kept growing and tumor markers increased. In July 2012, a needle aspiration biopsy was carried-out to confirm the recurrence of the tumor. The patient still refused standard treatment and underwent hyperthermia (total 24 times with Thermotron RF-8) and i.v. high dose vitamin C (total 10 times). She presented at our Clinic in January 2013. Her symptoms at presentation were a cough, back pain and severe swelling of the right arm (edema), and her pathological findings were invasive ductal carcinoma, N0 (no nodes were involved), negative surgical margin, grade 3, ER+, PR+, HER2+. Chest positron emission tomography and computed tomography (PET CT) on 6th June 2013 (Figure 1) showed a right axillary tumor, spinal metastases, intrapleural nodular tumor and right pleural effusion.
Second-generation high-dose GcMAF was administered at 0.5 ml, two times a week intramuscularly, for a total of 21 times. Sensitizers for SDT were modified in chlorin e6 at 25 mg i.v., and 5-aminolevulinic acid at 10 mg/kg orally. A total of 19 treatments of SDT were conducted from June to September 2013. Exemestane (Aromasin) aromatase inhibitor was also given to the patient at a dose of 25 mg/day orally.
By the beginning of October 2013 the patient showed dramatic improvement of symptoms such as cough, back pain and edema of the right hand from the combination therapy with SDT, GcMAF and hormone therapy. Her axillary tumor (Figure 1A) decreased in size and disappeared completely.

Chest tomography of a 55-year-old female patient on 6th June 2013 showing a right axillary tumor (A), spinal metastases (B), intrapleural nodular tumor and right pleural effusion (C).

A: Chest positron emission tomography and computed tomography (PET CT) horizontal plane of a 55-year-old female patient 6th June 2013 showing lung pleural effusion and intrapleural nodular tumor before treatment with sonodynamic therapy SDT. B: Chest CT horizontal plane on 9th September 2013 showing the complete disappearance of the lung pleural effusion and nodular shadow in the right lung after treatment with SDT and hormonal therapy.
Chest PET CT on 6th June 2013 (Figure 2A) showed lung pleural effusion and intrapleural nodular tumor before treatment with SDT. A later chest CT on 9th September 2013 (Figure 2B) showed complete disappearance of the pleural effusion and intra-pleural nodular tumor in the right lung after treatment with SDT, GcMAF and hormone therapy.
There was a significant increase in monocyte percentage and monocyte number (Figure 3) and a rapid decrease in tumor markers (Figure 4) during the treatment period from January 2013 to October 2013. There were no serious side-effects from the treatments except slight joint pain from the hormonal therapy with Exemestane aromatase inhibitor.
Discussion
Cancer is a broad group of diseases involving deregulated cell growth, forming malignant tumors which invade nearby parts of the body and can metastasize and spread to more distant parts. Therefore it is important to destroy local cancer tissue using therapies with minimal side-effects, whilst at the same time stimulating the immune system and allowing antigen-presenting cells display tumor-associated antigens to helper T-cells. This basic concept of recognizing tumor-associated antigens and teaching the immune system to attack cancer cells inside the body is a very similar idea to that of a cancer vaccine, even though a cancer vaccine itself is always created outside the body. Immunotherapy is both a local and a systemic therapy which can be used in combination with local tumor destruction in the case of large tumor burden.
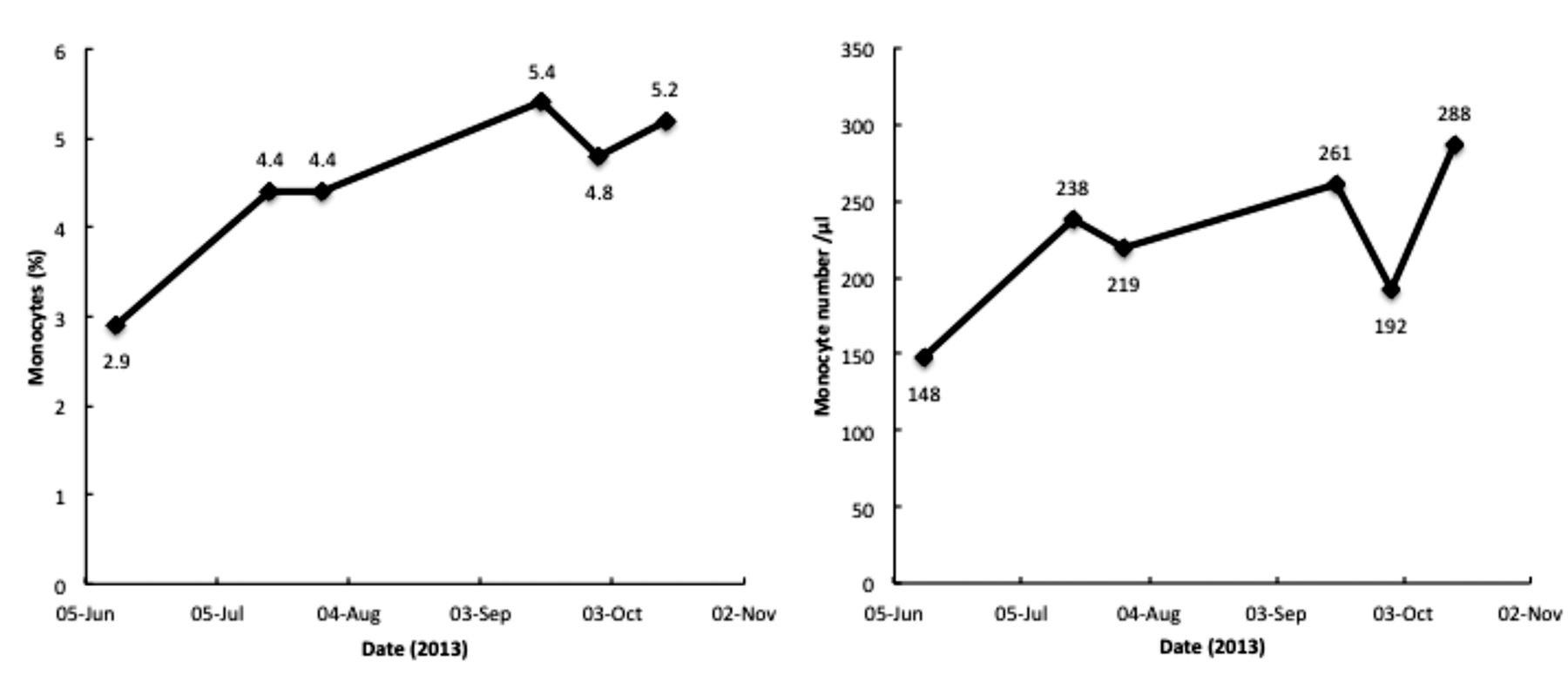
Change in blood monocyte percentage and monocyte number of 55-year-old female patient during Gc protein-derived macrophage-activating factor (GcMAF) therapy. The patient's monocyte number rose during high-dose GcMAF treatment, indicating a good response to the therapy.

Time course of tumor markers, nation cancer center-stomach-439 (NCC-ST-439), carbohydrate antigen 15-3 (CA15-3), and carboxy terminal telopeptide of type I collagen (ICTP). The patient's tumor markers rapidly decreased during the treatment period.
We highlight this case of a patient with terminal breast cancer having had good effects from SDT, GcMAF and hormonal therapy. It suggests that SDT and GcMAF can be used in combination with standard treatments, in particular targeted-therapies, with minimal toxicity and without negative effects on the immune system, to achieve better outcomes for patients with cancer. SDT, GcMAF and hormonal therapies are non-invasive, well-tolerated treatments that may be capable of controlling tumor progression by working synergistically. Furthermore, SDT and GcMAF may be capable of controlling tumor progression by inducing direct inflammatory necrosis inside tumors, producing antitumor immunity via antigen-presenting cells to prevent immune escape in a variety of deep and superficial tumors.
Utilizing these new approaches gives those of us who have been treating cancer good weapons that kill cancer cells selectively, efficiently, and by non-toxic and painless means. We are planning to further refine and improve our protocols with SDT and GcMAF.
Footnotes
-
This article is freely accessible online.
- Received April 4, 2014.
- Revision received June 12, 2014.
- Accepted June 13, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Concentration-dependent Activation of Inflammatory/Anti-inflammatory Functions of Macrophages by Hydrolyzed Whey Protein
- Case Report: A Non-small Cell Lung Cancer Patient Treated with GcMAF, Sonodynamic Therapy and Tumor Treating Fields
- Oral Colostrum Macrophage-activating Factor for Serious Infection and Chronic Fatigue Syndrome: Three Case Reports