


Abstract
Background: Due to local ventilation and perfusion differences in the pulmonary lobes, the microenvironmental influence on metastasis formation in the lung can be studied. We, therefore, investigated whether the anatomical distribution of first lung metastases follow a particular pattern. Materials and Methods: Thirty-three out of 273 patients with melanoma who underwent 18F-fluorodeoxyglucose positron emission tomography and computed tomography (18FDG-PET/CT) were identified as patients with detected primary pulmonary metastases. All solitary metastases were allocated to the appropriate lung segment. Results: Segment L3 had the significantly highest number of metastases (n=11; p<0.001). Overall, both upper lung lobes manifested numerously more metastases in comparison to the lower lobes (26 metastases (70%) vs. 11 metastases (30%); p<0.001). Conclusion: Our results provide novel information supporting the hypothesis that pulmonary metastases occur prevalently in the upper lung segments.
The formation of distant metastases accounts for more than 90% of all cancer-associated deaths, yet it remains the most poorly-understood component of cancer pathogenesis (1-3). Metastasis formation is a complex process starting with the uncontrolled growth of the first malignant clone (4). If this primary cell mass reaches a few dozen cells, it sends out angiogenic signals so that blood vessels grow into the tumour. Some malignant cells loosen themselves from the primary tumour and invade the blood vessels. In order to reach the connective tissue stroma at the site of the future metastasis, tumour cells have to interact with the endothelium of this organ. Once they have attached to the endothelium, they need to transmigrate through it and lodge in the connective tissue stroma beneath the blood vessel endothelium. If the malignant cell starts to divide again, it becomes a clinically detectable metastasis when it has reached the size of about 1 cm (3). The formation of clinically detectable metastases is not a random process as some organs, such as bone marrow, liver and lungs, are more prone to harbour metastases than others (5). This peculiar distribution of metastasis formation was already noted in the 19th century and was coined by Stephen Paget as the “seed and soil” hypothesis (6, 7).
In the metastatic cascade, tumour cells adhere to the endothelium at the target organ. They do so by mimicking the leukocyte–endothelium interaction cascade which sequentially involves several cell adhesion molecules, which are, in part, redundant. In principle, two different adhesion processes take place. The first step is a dynamic one in which the leukocyte or malignant cell rolls over the endothelium and is stopped. This process is mediated by E- and P-selectin on the side of the endothelium and by selectin-binding carbohydrate ligands on the cell surface of the rolling cells. Once the cells have stopped on the endothelium, a static adhesion process commences which ultimately triggers transendothelial migration (8, 9).
The role of dynamic and static adhesion of malignant cells to the endothelium during metastasis formation is far less clear. While an 85% reduction in the number of spontaneous lung metastases was observed in a colon cancer xenograft model in E- and P-selectin deficient SCID mice as compared to wild-type SCID mice (10), a considerable smaller reduction in the number of spontaneous breast cancer metastases occurred in a similar breast cancer model (11). However, both models show that the knock-out of E- and P-selectins alone are not sufficient to completely abrogate metastasis. Hence, depending on the malignant entity, static adhesion processes must also play a role in distant metastasis formation.
The ideal organ to investigate the role of these two adhesion mechanisms is the lung. First of all, the lung is the second most common organ for the occurrence of metastasis, including malignant melanoma (12, 13). Secondly, it is also a fundamentally heterogeneous organ because of regional differences in perfusion and ventilation ratio (14, 15). In an erect individual, the lung apex is relatively over-ventilated (ratio of ventilation to perfusion, 3:1), and the base is relatively overperfused (ratio, 0.6:1) (16-18). This ventilation and perfusion mismatching results in regional hypoxia, which also invokes hypoxic pulmonary vasoconstriction (HPV) (16). HPV is unique to the pulmonary circulation, as other circulations (coronary, cerebral, and systemic) dilate in response to hypoxia (19, 20). Pulmonary vessels constrict in response to alveolar hypoxia, resulting in diversion of blood flow away from the hypoxic area (20, 21). The narrowed vessels cause a resistance to blood flow, which leads to a decrease in the blood flow rate (22). Hence we hypothesize that the lower speed of leukocytes and malignant cells in the upper lung could facilitate adhesion of the two cell types to the endothelium by static adhesion.
For inflammation, this scenario seems to be true as the physiological disparities of the lung have been recognized as important factors determining the upper lobe predominance of certain pulmonary diseases (17). These account for an increased incidence of inflammation, which leads to a physiological overexpression of molecules of the leukocyte adhesion cascade, which are also essential for cancer cells to invade the organs.
However, for malignant cells, this disparity in the distribution of metastatic nodules has not been investigated, as far as we are aware. To do so, we chose malignant melanoma as the entity of choice. It is characterized by a high potential for invasion and metastasis, with resistance to current therapies and poor prognosis (23, 24). Paget himself in his landmark study noted the ophthalmologist Ernst Fuchs as the “chief advocate” of the seed and soil theory, who in cases of uveal melanoma described that some organs provide a more “fertile soil” for the growth of tumors than others (7).
Materials and Methods
Patient collective. An electronic database of patients with melanoma who underwent 18FDG-PET/CT examination from January 2009 to February 2013 was screened for those diagnosed with pulmonary metastases, and 273 patients were initially identified. Consecutively, all PET/CT reports were reviewed to identify patients with pulmonary metastases. The result was a total of 69 patients with the presence of lung metastases confirmed by a team of interdisciplinary physicians at the University Medical Center Hamburg-Eppendorf.
Among all patient reports, those describing the first pulmonary metastasis were identified. Patients were excluded in the case of non-identification of the first metastasis through PET/CT. The remaining 33 patients (29 with one metastasis; four with two metastases) were defined as patients with detected primary pulmonary metastases.
Patients' characteristics (n=33).
Imaging studies. PET/CT scanning was performed on a Philips Gemini GXL 10 System (Philips Medical Systems, (Cleveland) Inc., Cleveland, Ohio) after written informed consent had been obtained. Patients fasted for at least 4 h prior to the scanning, which started 60 min after the intravenous injection of 350±50 MBq of 18F-FDG. All patients were tested for a normal glucose level before scanning. Patients with glucose levels exceeding 200 mg/dl received intravenous insulin. One litre of an iodinated oral contrast agent (Gastrografin; BerliMed S.A., Madrid, Spain) was applied within one hour before CT imaging for better delineation of intestinal structures. PET data were acquired for 90 s per bed position at the head, thorax, and abdomen, and 60 s for the legs. A low-dose CT scan (120 kV, 80 mA, 5 mm slice thickness, no gap, 0.9 pitch, 0.74 s rotation time, 512×512 matrix) was performed for attenuation correction 60-90 min after FDG application. The diagnostic CT scan (Philips Gemini) followed after intravenous injection of iodine-containing contrast agent (Imerol 300; Bracco Imaging S.p.A., Colleretto Giacosa, Italy). The CT scan was acquired during breath holding in the normal expiratory position. The PET data were computed using an iterative 3D line-of-response reconstruction algorithm into a 144×144 matrix with a voxel size of 4×4×4 mm and the images were attenuation corrected. The imaging software (Extended Brilliance Workstation; Philips) provided multiplanar reformatted image view of PET and CT with linked cursors.
Evaluation. Images were reviewed and analysed qualitatively by two reporters without knowledge of the results of the imaging studies. Areas of focal increased uptake were considered pathological and were compared with follow-up investigations. If the FDG uptake was increased compared with the preliminary investigation, the lesions were interpreted as being metastases. If a metastasis was detected, fused PET/CT images were used to determine the exact anatomical localisation. Finally, all metastases of patients with solitary metastases were allocated to the appropriate lung segment by lung segmentation according to Huber (25).
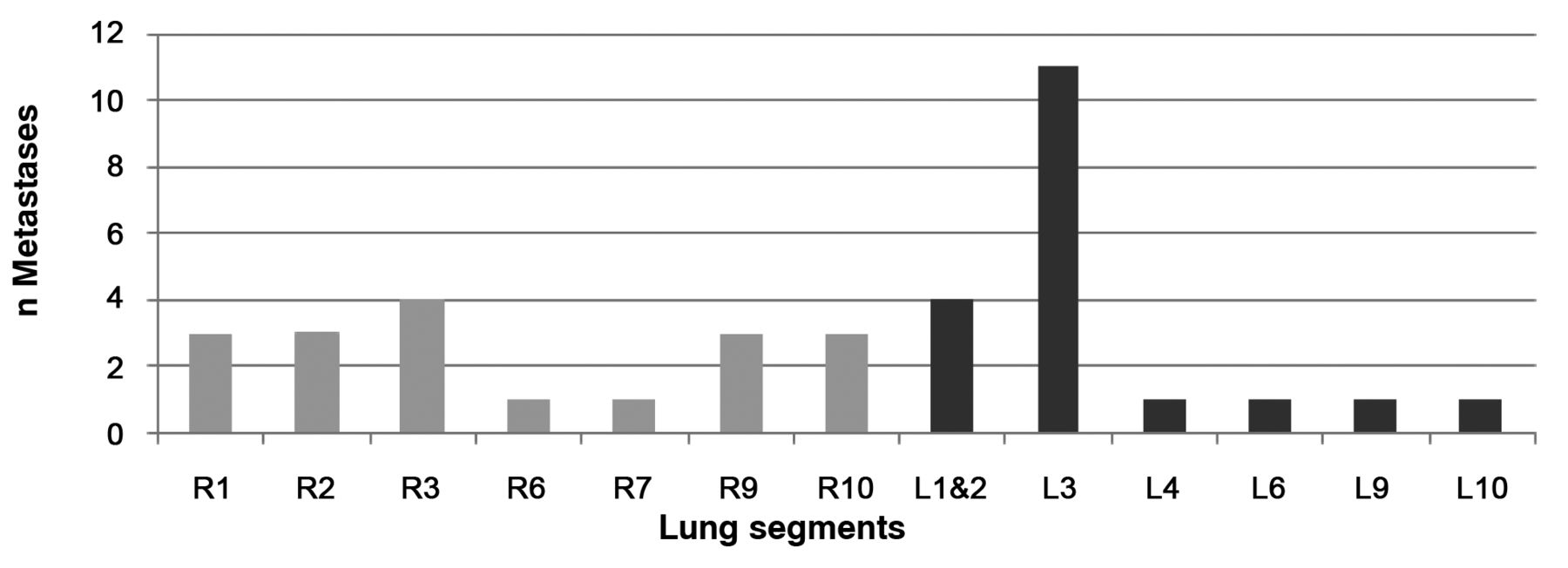
Diagramm showing the amount of metastases per lung lobe (‘L’ indicates lobes of the left and ‘R’ of the right lung)
Additionally, the site of the primary cutaneous melanoma was reconstructed from the study reports. The exact site of melanoma was only described for 20 patients. One patient with two separate primary nodules of malignant melanoma was excluded from this analysis because it was not possible to define which melanoma had metastasized to the lung.
Statistical analysis. The significance of differences between subgroups was calculated using the Chi-squared test. As null hypothesis, a uniform distribution of pulmonary metastases was chosen. Therefore the average number of metastases per lung segment was determined by correlating all lung segments with their mean volume (26). p-Values of less than 0.05 were considered statistically significant.
Results
Patients' characteristics are listed in Table I. There were 33 patients, of whom 22 were male and 11 females (67% vs. 33%; p=0.055). Primary tumours were located on the back in more than half of patients (56%, 18/33).
Figure 1 summarizes the numbers of pulmonary metastases for all lung segments. Segment L3 had the significantly highest number of metastases (n=11; p<0.001). Overall, both upper lung lobes manifested numerously more metastases in comparison to the lower lobes [26 metastases (70%) vs. 11 metastases (30%); p<0.001]. No metastases were detected in the middle lobe.
We were able to categorize 20 primary tumours to either the left or the right side of the patients. Interestingly, in 15 cases (75%; p=0.025), the primary tumour was located in the side opposite from that of the first pulmonary metastasis.
Discussion
The presence of pulmonary metastases in melanoma is clinically well-known, however, to the best of our knowledge, this is the first study concerning the localisation of individual metastases to particular lung segments. Compared to other cancer types, a skin lesion a few millimetres thick represents an advanced stage where the chance of developing distant visceral metastasis is very high (27). In comparison, other tumour types, such as colon or breast cancer, need a larger mass to be able to metastasize. To improve the understanding of metastasis formation, we attributed spontaneous melanoma metastases to individual lung segments. The most prominent finding in our investigation was the over-representation of primary lung metastases in left lung segment 3 (L3) compared to the other segments. Segment L3 accounted for 11 lesions, which is highly significant considering that this number represents 30% of all pulmonary metastases present here (p<0.001). Segment L3 was followed by R3 and L1 and 2 which only had four metastases each.
Additionally, the results show that the upper lung lobes apparently have predominance for metastatic localisation. Both upper lung lobes had significantly more metastases in comparison to the lower lobes [26 metastases (70%) vs. 11 metastases (30%); p<0.001]. This supports our hypothesis that pulmonary metastasis occur prevalently in the upper lung segments.
Almandos et al. (28) and others (29) discovered that hypoxia increases melanoma metastasis to the lung in an animal study. Supplementary to their results, we suspect that HPV also plays a role in the development of pulmonary metastases. The apex of the human lung is relatively under-perfused in comparison to the base of the lungs. This mismatch results in regional hypoxia, causing HPV (16). We assume that these constricted vessels cause a resistance in blood flow, leading to a possible decrease in the blood flow rate. The lower speed or probable stasis of the malignant cells in the upper lobes increases the static adhesion of the melanoma cells to the endothelium.
Another potential additional explanation could be the over-ventilation of the upper lobes. Due to over-ventilation of the apices, the upper lobes are exposed more often to particulates and other agents in comparison to the lower lobes. These account for an increased incidence of inflammation, leading to an overexpression of adhesion molecules on the endothelial surface used by leukocytes and metastatic cells to leave the blood vessels. As these features can also occur simultaneously, they may even amplify each other. Previous studies showed that the upper lobes are also predominant sites of lung cancer (30-31). The development of lung cancer could be attributed to mechanisms similar to those for melanoma metastases.
We were able to categorize 20 primary tumour locations to either the left or the right side of the body. Interestingly, in 15 cases (75%; p=0.025), the primary tumour was located on the opposite side from the first pulmonary metastasis. We are not able to explain this phenomenon, hence it remains unclear whether these occurred by chance or another molecular process underlies this observation.
Furthermore it should be mentioned that there were no primary pulmonary metastases of the middle lobe. Possible explanations for this could be the absence of a middle lobe in the left lung, the low volume of the middle lobe (9.2%±3.7%), and the small number of patients.
In conclusion, this retrospective study provides novel information supporting the hypothesis that pulmonary metastases occur prevalently in the upper lung segments. These findings highlight the importance of dynamic and static adhesion of malignant cells in metastasis formation and extend the original concept of the “seed and soil hypothesis.
Acknowledgements
We would like to thank Janos Mester for his extensive support and all individuals who have contributed to this study.
- Received March 30, 2014.
- Revision received May 27, 2014.
- Accepted May 28, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.