


Abstract
Background/Aim: Recurrent triple-negative breast cancer (TNBC) patients have poor prognoses and limited treatment options, especially after progression during prior chemotherapy. The present study aimed to determine the impact of itraconazole with chemotherapy in these patients. Patients and Methods: Medical records of recurrent TNBC patients receiving itraconazole with chemotherapy between 2008 and 2012 were retrospectively reviewed. Results: Thirteen patients who progressed during prior chemotherapy (12 with visceral organ metastases) were enrolled. All patients had received docetaxel, carboplatin, and gemcitabine with itraconazole. Additionally, 3 patients with pleural effusion and 2 with inflammatory breast cancer received bevacizumab. No febrile neutropenia, platelet transfusion, or chemotherapy-related death was observed during treatment with itraconazole. The response rate, median progression-free survival, and median overall survival were 62% (95% confidence interval (CI): 35-88%), 10.8 months (95%CI: 7.6-15.3 months), and 20.4 months (95%CI: 13.1-41.4 months), respectively. Conclusion: Chemotherapy with itraconazole is promising for heavily pre-treated TNBC patients.
Triple-negative breast cancer (TNBC) is a heterogeneous sub-group of breast cancer, characterized by low expression of both estrogen and progesterone receptors, and the lack of human epidermal growth factor receptor-2 overexpression (1, 2). TNBC accounts for approximately 10-15% of all breast cancer cases (3, 4) and is associated with a poor prognosis due to limited treatment options. Platinum-based regimens are often selected to treat TNBC owing to the disease's similar molecular features to hereditary BRCA1-related breast cancer (5, 6). A cytotoxic regimen of carboplatin and gemcitabine was administered in the control arm of a randomized phase II trial, and the addition of iniparib prolonged the overall survival (OS) of patients with metastatic TNBC; however, a subsequent phase III trial failed to demonstrate the efficacy of iniparib (7, 8). Combining bevacizumab with a taxane or other standard chemotherapeutic agents significantly improved progression-free survival (PFS) in a second-line setting (RIBBON-2) (9), but failed to improve OS. Therefore, a therapeutic breakthrough is urgently needed, especially for refractory disease.
P-glycoprotein (P-gp, also known as multidrug resistance-1 or ATP-binding cassette sub-family B member [ABCB]-1) has been extensively studied in breast cancer for its role in overcoming taxane resistance (10, 11). In the late 20th century, itraconazole, a common anti-fungal agent, was demonstrated to reverse the P-gp-mediated resistance associated with taxanes in a concentration-dependent manner in vitro (12, 13). Its potential for inhibiting angiogenesis and Hedgehog signaling pathway in cancer stem cells has recently been reported (14, 15). Since 2013, the clinical benefit of itraconazole has been documented in prospective trials of prostate cancer, non-small cell lung cancer (NSCLC), and basal cell carcinoma as well as in our retrospective studies of recurrent ovarian cancer (16-20). The present retrospective exploratory study aimed to assess the efficacy of itraconazole in heavily pre-treated patients with TNBC.
Patients and Methods
We retrospectively reviewed the medical records of patients with histologically confirmed TNBC who received chemotherapy in conjunction with itraconazole at Kohnan hospitals between 2008 and 2012. The visceral organs with metastases included the lungs, brain, and liver, but patients with bone or lymph node metastases were excluded. All patients provided written informed consent, and the study was approved by the Institutional Review Board (3-2-2007).
When the same regimen was administered, the number of regimens was recorded as 1. The treatment-free interval was calculated from the last date of previous chemotherapy to the first date of chemotherapy with itraconazole. The taxane-free interval was calculated from the last date of taxane administration to the first date of chemotherapy with itraconazole.
Patients' demographics (N=13).
Adverse events during the first concurrent administration of itraconazole and chemotherapy were graded according to the National Cancer Institute Common Toxicity Criteria, version 4.0. Efficacy was evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST), version 1.1 (21). Progression-free survival (PFS was defined as the time from the first itraconazole administration to the date of objectively determined disease progression or health status deterioration. OS was defined as the time from the first itraconazole administration to death.
Statistical analyses were performed on the observed distributions of PFS and OS using the Kaplan–Meier method. All analyses were conducted using XLSTAT 2014 (Addinsoft, Paris, France).
Results
Patients' characteristics. Between 2008 and 2012, 13 recurrent TNBC patients were concurrently treated with chemotherapy and itraconazole. Patients were referred from tertiary Hospitals after progression during 2 or more lines of chemotherapy. The referral Hospitals' pathological reports were reviewed to verify the diagnosis. All patients had previously received anthracyclines and taxanes, including weekly paclitaxel in 10 patients (77%), docetaxel in 7 (54%), and nab-paclitaxel in 1 (8%). None of the patients had received bevacizumab or eribulin. All patients had a treatment-free interval of less than 3 months, and 4 were referred from tertiary hospitals after progression during prior taxane administration (Table I).
Response rate associated with chemotherapy with itraconazole.
Regimens with itraconazole. A cytotoxic regimen consisting of docetaxel, carboplatin, and gemcitabine was administered in combination with itraconazole. The starting doses of intravenous docetaxel, carboplatin, and gemcitabine were 35 mg/m2 (day 1), area under the curve of 4 mg x min/ml (day 1), and 1000 mg/m2 (day 1), respectively. An oral itraconazole solution was administered at a daily dose of 400 mg (days −2 to 2). This regimen was repeated every 2 weeks. A dose modification for carboplatin and docetaxel in the following cycle was considered if necessary to maintain patients' white blood cell (WBC) and platelet counts within the ranges of 1,000-1,500/mm3 and 30,000-50,000/mm3, respectively (19). Gemcitabine and itraconazole doses were fixed. After 6 cycles, docetaxel was switched to vinorelbine or irinotecan to prevent chemotherapy-induced peripheral neuropathy. Granulocyte colony-stimulating factor (G-CSF) was administered according to the manufacturer's recommendations on the drug label until the WBC count and absolute neutrophil count (ANC) recovered. In addition to cytotoxic agents and itraconazole, bevacizumab was administered at 15 mg/kg every 4 weeks to 3 patients with pleural effusion and 2 with inflammatory breast cancer.
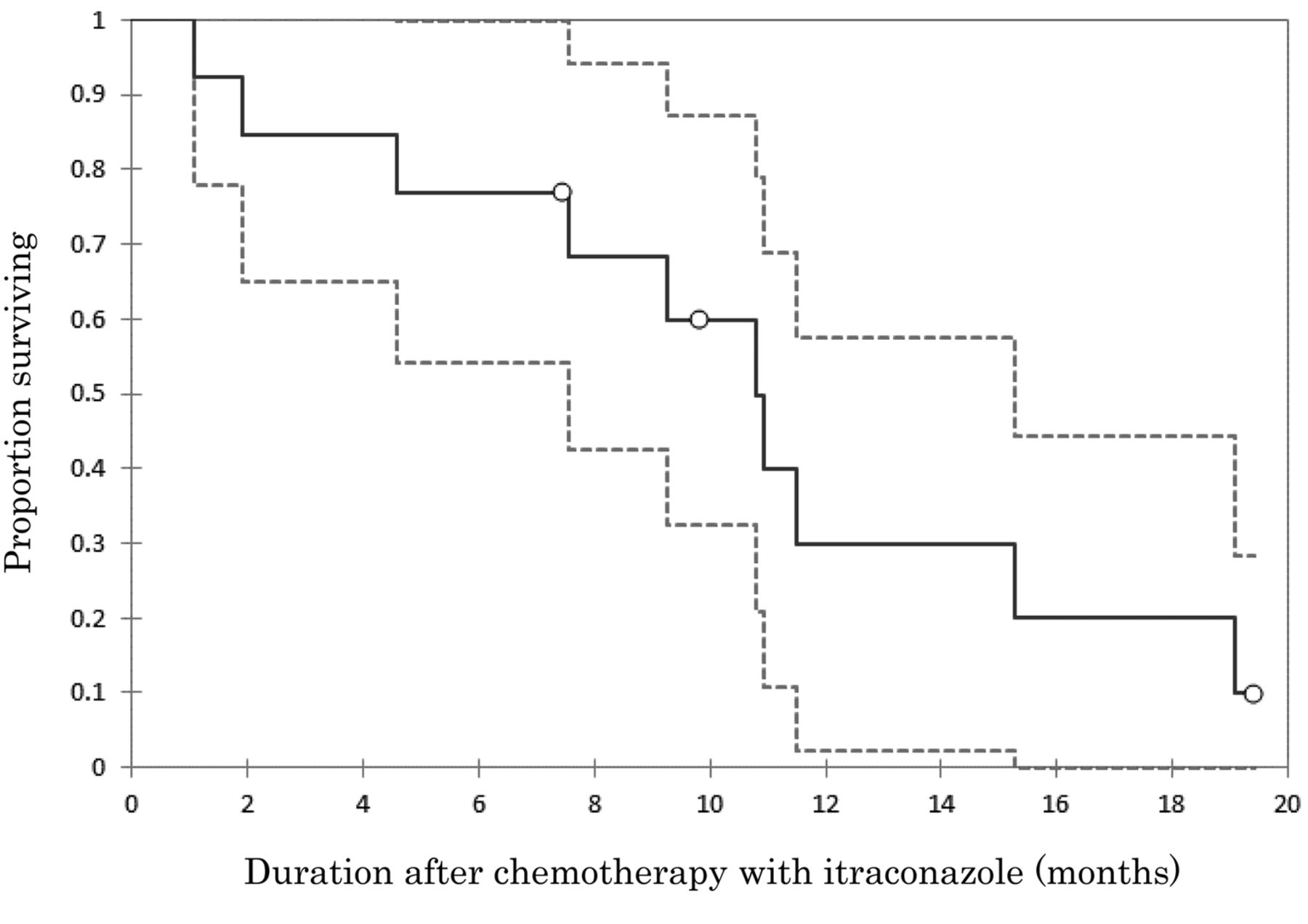
Efficacy. The response rates of patients receiving chemotherapy in conjunction with itraconazole were 62% (95% confidence interval [CI], 35-88%) according to the RECIST 1.1 criteria (Table II). The median PFS after the initiation of chemotherapy and itraconazole was 10.8 months (95%CI, 7.6-15.3 months), with data on 3 patients censored (Figure 1). The median OS after chemotherapy and itraconazole was 20.4 months (95%CI: 13.1-41.4 months), with data on 3 patients censored (Figure 2).

Progression-free survival (PFS) after chemotherapy with itraconazole. The median PFS was 10.8 months (95% confidence interval, 7.6-15.3 months).

Overall survival (OS) after chemotherapy with itraconazole. The median OS was 20.4 months (95% confidence interval, 13.1-41.4 months).
Toxicities. During combinatorial treatment with chemotherapy and itraconazole, all patients received G-CSF, and their WBC count and ANC recovered within 5 days. None of the patients experienced febrile neutropenia or required platelet transfusion. All patients received packed red blood cell transfusion when their hemoglobin levels fell below 8.0 g/dl. No treatment-related death occurred during combinatorial treatment with chemotherapy and itraconazole.
Discussion
The primary aim of chemotherapy for refractory disease in heavily pre-treated patients with metastatic breast cancer is symptom palliation and quality of life maintenance. In a phase III randomized control study (EMBRACE) (22), eribulin monotherapy improved the OS of the studied patients, all of whom had received 2 or more prior chemotherapy regimens for advanced or recurrent diseases and had progressed within 6 months of the latest chemotherapy. The median OS was 13.1 months. In that study, 18% of enrolled patients had TNBC. The background of our investigation is similar to that of the above-mentioned study, except for the proportion of patients with TNBC. TNBC, a heterogeneous sub-group of breast cancer with a poor prognosis due to limited treatment options, shares many molecular features with hereditary BRCA1-related breast cancer. BRCA dysfunction is associated with a high sensitivity to platinum (23, 24). In a recent study (CALGB 40603), carboplatin as neoadjuvant chemotherapy improved the pathologic complete response rate among patients with TNBC (25); however, no survival benefit was observed in advanced or metastatic TNBC cases (26, 27). In a subgroup analysis of the RIBBON-2 trial (9), the addition of bevacizumab to second-line chemotherapy improved PFS but not OS in TNBC patients. In that study, 74% of the enrolled patients who received bevacizumab-containing therapy had visceral metastases and 67% had a treatment-free interval of >6 months. Their median OS was 17.9 months. The median OS of 20.4 months in our study was therefore favorable, considering the poorer patient background.
Inflammatory breast cancer is highly aggressive and has the worst survival outcome amongst all breast cancer subtypes. Inflammatory breast cancer often presents with high expression levels of angiogenic factors such as vascular endothelial growth factor (VEGF), and thus, anti-angiogenic agents that target VEGF have been the focus of clinical trials (28-32). In our study, 2 patients received bevacizumab with chemotherapy and itraconazole, although recent trials have indicated a modest effect of bevacizumab therapy. Additionally, since VEGF-A plays a critical role in pleural effusion development (33-35), 3 patients with pleural effusion also received bevacizumab.
Resistance could simultaneously occur to therapeutic agents even when they have not been used in prior chemotherapy and differ from previous agents in chemical structure or mode of action. To improve the efficacy of chemotherapy, mechanisms of resistance involving the P-gp-mediated efflux system have been extensively studied. Toppmeyer et al. reported that of 35 breast cancer patients with paclitaxel-refractory disease who received paclitaxel with biricodar (VX-710), 4 (11%) achieved a partial response (36). When valspodar (PSC 833), a second-generation P-gp modulator, was administered with paclitaxel in 34 metastatic breast cancer patients, only 7 (21%) responded (37). To date, neither biricodar nor valspodar has been reported in a phase III clinical trial of breast cancer. However, valspodar was investigated in a phase III study of front-line chemotherapy for ovarian cancer. Compared to the standard regimen of paclitaxel and carboplatin, paclitaxel dose in that study was reduced from 175 mg/m2 to 80 mg/m2, when administered in combination with valspodar. Such a dose reduction of cytotoxic agents was necessary owing to the drug-drug interactions involving cytochrome P450, family 3, subfamily A (CYP3A) inhibition. However, the addition of valspodar to standard chemotherapy regimens did not improve PFS or OS, yet increased the number of adverse events (38). The third-generation P-gp inhibitor, tariquidar (XR9576), offered increased specificity and potency (39). Docetaxel could be safely administered at 75 mg/m2 every 3 weeks in combination with tariquidar (40). Nevertheless, to date, the concept of reversing drug resistance has failed in phase III clinical trials.
The anti-tumor effect of itraconazole has been reported in clinical studies since 2013. In a prospective analysis of itraconazole as a single agent, castration-resistant prostate cancer patients who received 600 mg itraconazole per day had a prolonged PFS compared to those receiving 200 mg per day (11.9 vs. 35.9 weeks). In a prospective translational study of basal cell carcinoma, itraconazole decreased the tumor area, together with reduced cell proliferation and Hedgehog pathway activity (18). The efficacy of itraconazole administered in combination with chemotherapy was also reported in patients with NSCLC and ovarian cancer. In a randomized phase II trial, concomitant itraconazole and pemetrexed therapy yielded an improved OS compared to therapy without itraconazole (32 vs. 8 months, hazard ratio=0.194, p=0.012) (17). In different retrospective studies for ovarian cancer, we have reported prolonged OS among patients who received itraconazole with chemotherapy. In recurrent clear cell carcinoma (19), which is known for its resistance to chemotherapy, patients who received chemotherapy with itraconazole had prolonged OS compared to historical controls or those who did not receive itraconazole (p=0.006). For recurrent ovarian cancer patients who had platinum resistance and progressed during prior chemotherapy (20), the OS of those receiving chemotherapy with and without itraconazole were 642 and 139 days, respectively (hazard ratio=0.27, p=0.006). The present study showed a more favorable outcome than those previously reported for heavily pretreated patients with TNBC, which is consistent with published investigations of itraconazole in other solid tumors.
Our present study has certain limitations, including its small sample size and observational nature. Data were pooled retrospectively from a single Institute. The cytotoxic regimen administered in combination with itraconazole was a triplet of docetaxel, carboplatin, and gemcitabine, which was unusualfor heavily treated patients. The dose modification was complicated, and all patients received G-CSF and packed red blood cell transfusion, although none had febrile neutropenia or platelet transfusion. Further investigation on efficacy, toxicity, and compliance is necessary for the cytotoxic regimens administered with itraconazole as well as the itraconazole dose. Nevertheless, our results are encouraging for heavily treated patients with TNBC owing to the efficacy and limited toxicity of itraconazole. Furthermore, itraconazole is not an expensive drug, and thus, its use could be affordable for patients in developing countries and might reduce treatment costs for those in developed countries.
Footnotes
-
Conflicts of Interest
The Authors have no financial conflicts of interest to disclose.
- Received March 25, 2014.
- Revision received May 23, 2014.
- Accepted May 26, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Itraconazole Repolarizes Tumor-associated Macrophages and Suppresses Cervical Cancer Cell Growth
- First-Line Gemcitabine, Nab-Paclitaxel, and Oxaliplatin Chemotherapy With Itraconazole in Patients With Metastatic Pancreatic Cancer: A Single Institution Experience
- Itraconazole Exerts Its Antitumor Effect in Esophageal Cancer By Suppressing the HER2/AKT Signaling Pathway
- S-1, Oxaliplatin, Nab-paclitaxel and Itraconazole for Conversion Surgery for Advanced or Recurrent Gastric Cancer
- Itraconazole Inhibits AKT/mTOR Signaling and Proliferation in Endometrial Cancer Cells
- Divergence of Antiangiogenic Activity and Hepatotoxicity of Different Stereoisomers of Itraconazole
- Expression of Hedgehog Signals and Growth Inhibition by Itraconazole in Endometrial Cancer
- Antifungal drug itraconazole targets VDAC1 to modulate the AMPK/mTOR signaling axis in endothelial cells
- Impact of Itraconazole After First-line Chemotherapy on Survival of Patients with Metastatic Biliary Tract Cancer
- Combination Chemotherapy with Itraconazole for Treating Metastatic Pancreatic Cancer in the Second-line or Additional Setting