


Abstract
Background: Although patients with the echinoderm microtubule-associated protein-like 4–anaplastic lymphoma kinase gene (EML4-ALK) re-arrangement and epidermal growth factor gene EGFR mutations have proven sensitive to specific inhibitors, there is currently no consensus regarding the sensitivity of non-small cell lung cancer (NSCLC) patients with such mutations to cytotoxic chemotherapy. Patients and Methods: The responses to first-line cytotoxic chemotherapy were retrospectively compared between advanced or postoperative recurrent patients with non-squamous NSCLC who harbor the EML4-ALK fusion gene (ALK+), EGFR mutation (EGFR+), or neither abnormality (wild-type). Results: Data for 22 ALK+, 30 EGFR+, and 60 wild-type patients were analyzed. The ALK+ group had a significantly lower response rate than the other two groups. Progression-free survival was significantly shorter in the ALK+ cohort compared to the EGFR+ (p<0.001) and wild-type cohorts (p=0.0121). Conclusion: NSCLC patients with the EML4-ALK fusion gene might be relatively insensitivite to cytotoxic chemotherapy.
- Non-small cell lung cancer
- anaplastic lymphoma kinase
- epidermal growth factor mutation
- cytotoxic chemosensitivity
Lung cancer is one of the most common causes of death worldwide (1). Non-small cell lung cancer (NSCLC) is the most prevalent histological type, accounting for almost 80% of all lung neoplasms. Its refractoriness to chemotherapy means that little major progress has been made in the treatment of advanced or recurrent NSCLC until recently, though the discovery of driver mutations is now changing the conventional treatment.
Somatic mutations in the epidermal growth factor receptor gene (EGFR) have been shown to correlate with clinical response to the tyrosine kinase inhibitor (TKI), gefitinib (2). The results of randomized phase III studies indicated that progression-free survival (PFS) was significantly longer in patients who received gefitinib compared to those who received cytotoxic chemotherapy (3, 4). The echinoderm microtubule-associated protein-like 4–anaplastic lymphoma kinase (EML4-ALK) fusion gene was identified in NSCLC in 2007 (5), since then small-molecule inhibitors targeting EML4-ALK have been developed and have shown impressive efficacy in patients with lung adenocarcinomas harboring the EML4-ALK fusion gene (6).
In this context, it is becoming increasingly important to consider the genetic status, such as EGFR mutations and EML4-ALK rearrangements, when selecting chemotherapies for NSCLC. Cisplatin-containing regimens are still important to the treatment of postoperative-recurrent or advanced NSCLC, though the sensitivity of NSCLCs with gene mutations to such cytotoxic chemotherapies remains unclear. Some studies (7-9) have investigated the response of NSCLC patients with EGFR mutations or the EML4-ALK fusion gene to cytotoxic chemotherapy, but the results remain controversial. The present study aimed to evaluate the efficacy of cytotoxic chemotherapy in NSCLC with driver-gene mutations.
Patients and Methods
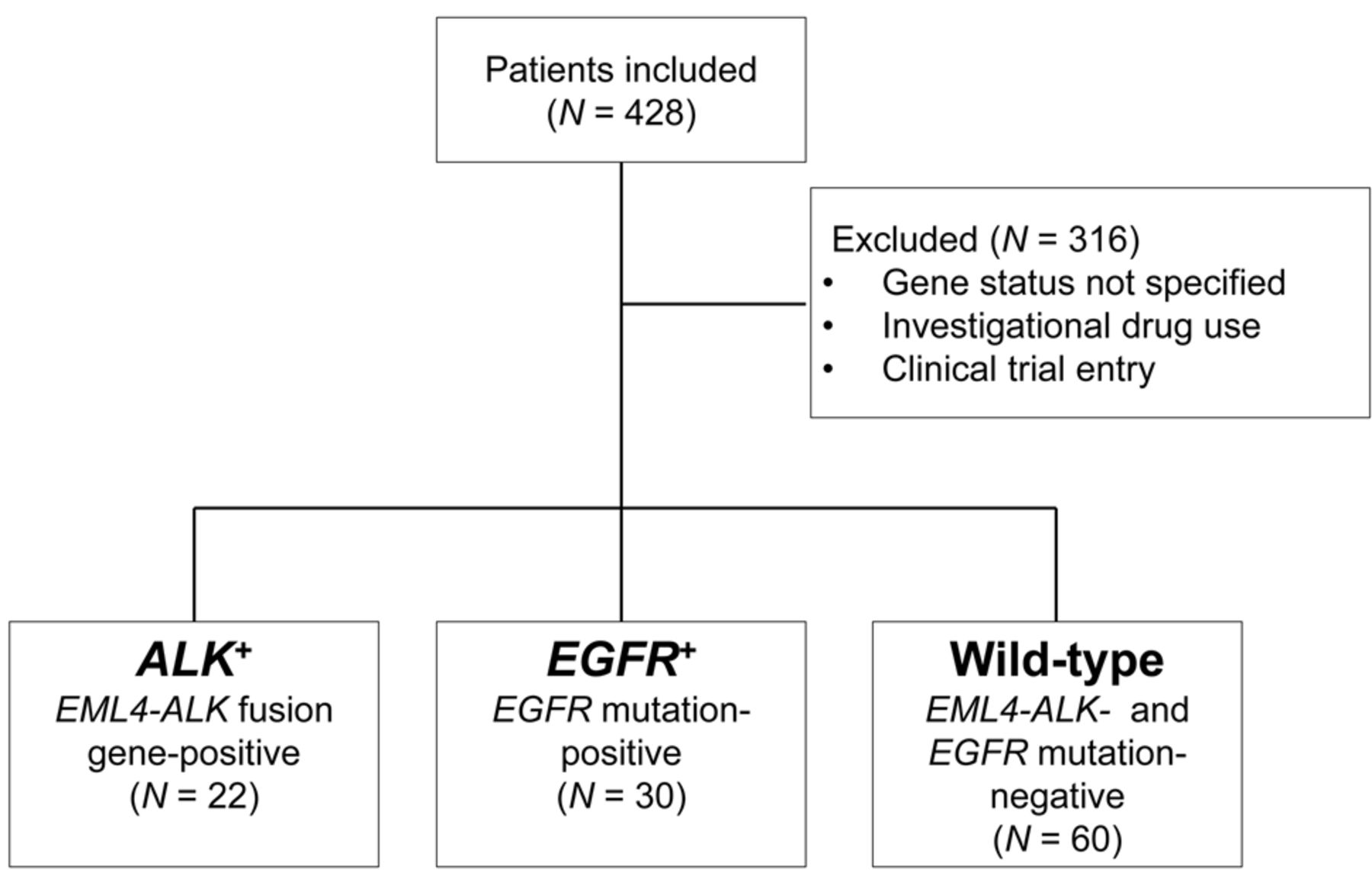
This retrospective study enrolled 428 patients with advanced or recurrent non-squamous NSCLC treated with first-line cytotoxic chemotherapy, excluding patients treated with molecular-targeted drugs such as EGFR-TKIs or ALK inhibitors, at the Kyushu Cancer Center between April 2009 and March 2012. Only patients who met the following inclusion criteria were registered: (i) screened for both EGFR mutation and EML4-ALK fusion gene status; (ii) not treated with any investigational drug and not registered on any other clinical study as first-line chemotherapy (Figure 1). Patients were classified into three groups: patients with the EML4-ALK fusion gene but without EGFR mutation (ALK+); patients with EGFR mutation but without EML4-ALK fusion gene (EGFR+); patients with neither EML4-ALK fusion gene nor EGFR mutation (wild-type). Written informed consent was obtained from all patients and the study was approved by the hospital ethics committee. The present study also conformed to the provisions of the Declaration of Helsinki.
Detection of EGFR mutations and EML4-ALK rearrangements. Tumor specimens were grossly dissected by a pathologist. Genomic DNA was extracted and purified from formalin-fixed paraffin-embedded tissues. EGFR mutations were detected using the peptide nucleic acid-locked nucleic acid polymerase chain reaction clamp method (10). ALK re-arrangements, were detected by fluorescence in situ hybridization, immunohistochemistry or reverse transcription-polymerase chain reaction, according to previous reports (11).
Treatment response. Imaging studies, including chest computed tomography scans, were performed after every two cycles of treatment (or sooner if needed) to evaluate response and document disease progression. Responses were classified according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Treatment response was defined as the best response recorded during the period from the start of treatment to the time of disease progression or treatment discontinuation. Treatment responses were evaluated according to RECIST, and were defined as complete response (CR), partial response (PR), stable disease (SD) or progressive disease (PD).
Statistical analysis. Associations among clinical characteristics and treatment responses between two subgroups were analyzed by χ2 or Fisher's exact tests. PFS was defined as the time elapsed between treatment initiation and tumor progression or death from any cause, and was calculated using the Kaplan–Meier method. The log-rank test was used to obtain p-values for univariate survival analysis, with appropriate adjustment for multiplicity. A p-value <0.05 was considered statistically significant. Statistical analysis was performed using JMP pro 9.0 (SAS Institute INC., Cary, NC, USA).
Results
Patients' characteristics. The demographic and clinical characteristics of patients are summarized in Table I. The median age of the patients at study entry was 58.5 years (range, 27-75 years). The majority of patients were female (64.3%), had a performance status of 0 (76.7%), had adenocarcinoma (96.4%), were a current or former smoker (60.7%), and had clinical stage IV disease (79.5%). ALK+ patients (median age, 53 years) were significantly younger than EGFR+ (median age, 65 years; p<0.001) and wild-type patients (median age, 61 years; p<0.001). No patients had both an EGFR mutation and EML4-ALK rearrangement. Genetic status was strongly related to smoking history (p<0.001) and sex (p=0.0109).
Clinical response to cytotoxic chemotherapy according to genetic subtype of NSCLC. Treatment response was evaluated in all patients (Table II). Out of the 112 patients who met the inclusion criteria and were analyzed, none (0%) had CR, 47 patients (42.0%) had PR, 39 (34.8%) had SD and 26 (23.2%) had PD. The overall response rate (RR) was 42.0% (95% confidence interval (CI)= 33.6-51.6%). The RRs in the three cohorts were 18.1% in the ALK+ cohort, 53.3% in the EGFR+, and 45.0% in the wild-type cohort. The RR in the ALK+ cohort was significantly lower than in the other two cohorts (p=0.0198 for EGFR+ cohort, p=0.0225 for wild-type cohort), but there was no significant difference in RR between the EGFR+ and wild-type cohorts. There were no patients in the EGFR+ cohort with PD.

Criteria for patient selection. Patients were grouped into three cohorts according to genetic status.
We also analyzed the correlation between chemotherapy regimen and clinical response (Figure 2). We classified the different types of chemotherapy and evaluated the influence of genetic status on sensitivity to cytotoxic chemotherapy according to the presence and type of gene abnormalities. Chemotherapy was classified into platinum doublet, platinum doublet-plus-bevacizumab, and others. ‘Others’ included patients who were treated by single-agent therapy, including three patients treated with docetaxel and three with pemetrexed. The combination of platinum doublet and bevacizumab achieved relatively good responses among patients in the EGFR+ and wild-type cohorts, while relatively few ALK+ patients achieved a partial response.
Some studies have suggested that the ALK fusion gene is a sensitivity biomarker for pemetrexed (12, 13), and pemetrexed-containing regimens were thus analyzed in detail in this cohort (Figure 3). However, only 22% of patients in the ALK+ cohort achieved a partial response with a pemetrexed-containing regimen, which was still lower than in the other cohorts. There was no significant difference in response to pemetrexed-containing regimens between the ALK+ and wild-type cohorts (p=0.438).
Analysis of PFS according to genetic status. PFS curves of sub-groups according to genetic status are shown in Figure 4. The median PFS times were 105 days for the ALK+ cohort (95%CI=57-161 days), 154 days for the wild-type cohort (95%CI=101-227 days) and 186 days for the EGFR+ cohort (95%CI=149-330 days) after a median follow-up period of 173.1 days (range=11-768 days). PFS was significantly shorter in the ALK+ cohort compared with the wild-type (p=0.0121) and EGFR+ cohorts (p<0.001). There was no significant difference between the wild-type and EGFR+ cohorts according to survival analysis, though PFS tended to be higher in the EGFR+ cohort compared with the wild-type cohort (p=0.091) (Figure 4).
Characteristics and patients' genetic statuses.
Clinical response to first-line chemotherapy according to genetic status.
Discussion
We investigated the efficacy of cytotoxic chemotherapy in patients with NSCLC with driver-gene mutations, including EGFR mutations and EML4-ALK gene fusion. The results suggest that NSCLC patients with the EML4-ALK fusion gene may be more resistant to conventional cytotoxic chemotherapy than those with EGFR mutations or with neither abnormality, while patients with EGFR mutations showed a relatively good response to cytotoxic chemotherapy. In contrast to the results of a previous report, NCSLC patients with the EML4-ALK fusion gene did not have a better response to pemetrexed than other cohorts.

First-line chemotherapy regimens and best responses among the three cohorts. Vertical axis indicates number of patients. Bv, bevacizumab.

Proportion of best response to pemetrexed. Data for pemetrexed-containing regimens were extracted from Figure 2 and re-analyzed in terms of sensitivity.
Our data suggest that patients with the EML4-ALK fusion gene show increased resistance to cytotoxic chemotherapy, which may translate into a poor prognosis for NSCLC patients harboring this re-arrangement. Recent reports have indicated an association between NSCLC prognosis and the ALK fusion gene. Although different opinions have been expressed (14), the ALK rearrangement is generally thought to be associated with a poorer prognosis (8, 15).
Our current results suggest the existence of a relationship between driver-gene mutation and chemosensitivity. Previous studies have reported that EGFR mutation status could be a biomarker of response to cytotoxic chemotherapy (7, 16, 17), as is suggested by the tendency identified in our study. However, our results demonstrated that ALK+ NSCLC was more resistant to cytotoxic chemotherapy than EGFR+ and wild-type tumors. This is in contrast to the results of Takeda et al. (9), who found similar overall survival rates in wild-type and ALK+ NSCLC patients in terms of first-line chemotherapy, or those of Lee et al. (8), who found no differences in PFS after first-line chemotherapy, irrespective of genetic status. There are several possible explanations for these discrepancies. These studies, including the present one, were subject to limitations, such as a retrospective design, single-institution study, small EML4-ALK cohort size, or selection bias in that not all patients were examined for EGFR and EML4-ALK gene status. Moreover, the different outcomes may have been attributable to effects of EML4-ALK variants or racial variation on sensitivity to cytotoxic chemotherapy. More recently, Shaw et al. reported a RR of only 7% with docetaxel in second-line chemotherapy in ALK+ patients (18), indicating the refractory nature of ALK+ cancer. However, the effects of the EML4-ALK fusion gene on the response of patients with NSCLC to cytotoxic chemotherapy remain controversial, and further prospective studies or meta-analyses are needed to clarify the predictive value of gene mutation status for cytotoxic chemotherapy.

Kaplan–Meier survival curve of progression-free survival (PFS) for patients in the three cohorts. The thick line indicates ALK+ cohort, thin line indicates wild-type cohort, broken line indicates EGFR+ cohort.
The mechanism responsible for the relationship between EML4-ALK and chemosensitivity remains unclear. Some studies have reported that the EML4-ALK fusion gene was predictive of a favorable response to pemetrexed in NSCLC (12, 13). They suggested that the increase in sensitivity to pemetrexed was the result of activation of the folate-pathway enzyme 5-aminoimidazole-4-carboxamide ribonucleotide formyltransferase/inosine monophosphate cyclohydrolase, and inhibition of the DNA-synthesis enzyme thymidylate synthase, rendering ALK+ carcinoma more sensitive to pemetrexed (12, 18, 19), in contrast with the results of the current study. This discrepancy could be caused by differences among ALK variants in terms of their effects on sensitivity to cytotoxic chemotherapy. Heuckmann et al. showed that different ALK fusion variants had different protein stabilities, with consequent effects on sensitivity to ALK inhibitors (20). It is possible that this phenomenon could also impact on the effects of cytotoxic chemotherapy. Further basic studies are required to investigate these speculations.
Despite the need for further studies, the current results suggest that gene-mutation status should be considered when choosing for an appropriate chemotherapeutic regimen in patients with NSCLC. Yamashita et al. and Kalikaki et al. reported that NSCLC patients with EGFR mutations were sensitive to chemotherapy (17, 21). The result of the NEJ002 study might thus infer that NSCLC patients with EGFR mutations could be treated with EGFR-TKIs after cytotoxic chemotherapy (22). In contrast, if NSCLC patients with ALK rearrangements are resistant to cytotoxic chemotherapy, as suggested by our results, they might progress during the course of first-line chemotherapy, and could thus miss the opportunity to be treated with ALK inhibitors. Shaw et al. (23) reported that EML4-ALK+ patients treated with the ALK inhibitor crizotinib had a more favorable prognosis than those without crizotinib. The administration of cytotoxic agents as first-line chemotherapy should, therefore, be carefully planned and discussed in patients with NSCLC with EML4-ALK rearrangements.
In conclusion, through the present study we report an association between the EML4-ALK fusion gene and insensitivity to cytotoxic chemotherapy in NSCLC. Our results suggest that EML4-ALK+ patients might be more insensitive to cytotoxic chemotherapy than patients with EGFR mutations or those with neither abnormality. EML4-ALK re-arrangement and EGFR-mutation status might be useful predictive biomarkers for the efficacy of cytotoxic chemotherapy.
Acknowledgements
We gratefully acknowledge Ms. Oshima and Ms. Maruyama for their helpful assistance with gathering clinical data.
Footnotes
-
Conflicts of Interest
The Authors have declared no conflicts of interest.
- Received March 8, 2014.
- Revision received May 9, 2014.
- Accepted May 12, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.