


Abstract
Endometrial cancer is the most common gynecological cancer in the Western world. In early-stage disease, surgery remains the mainstay of treatment. Adjuvant pelvic radiotherapy reduces the risk of pelvic recurrence, however, without improvement in overall survival. The aim of the present study was to assess the efficacy and toxicity of carboplatin and epirubicin combination chemotherapy for patients with advanced and high-risk endometrial cancer. Patients and Methods: Between 1999 and 2007, 43 patients with endometrial cancer were treated with carboplatin and epirubicin. Two groups were identified: Group 1 (n=34) included patients with stage III endometrial cancer receiving adjuvant chemotherapy; and group 2 included those with metastatic endometrial cancer (n=9). Results: After a median follow-up of 37 months, disease in 19 patients had progressed/relapsed (12 patients from group 1; 7 from group 2) and 23 patients had died (15 from group 1; 8 from group 2). The median time-to-progression was 62 months and median overall survival was 64 months. The median survival for patients in group 1 was 69 months and for those in group 2 was 22 months. Ten patients (27.9%) experienced grade 3 or 4 toxicities. There were no cases of treatment-related cardiac failure or neuropathy. Conclusion: Cisplatin, carboplatin, anthracyclines and taxanes are the most active agents in endometrial cancer. Combination chemotherapy leads to better progression-free survival and overall survival, however, this is at the expense of increased toxicity. Results from our study show that the combination of carboplatin and epirubicin is an effective alternative regimen for patients with advanced endometrial cancer. In addition, treatment-related toxicity is minimal when compared to anthracyclines and platinum agents. There is a particular advantage of this regimen over taxane-based regimens, including minimal neuropathy, less use of steroids and low risk of allergic reaction and alopecia.
Endometrial cancer is the most common gynecological cancer in the Western world, with incidence increasing in the UK by over 40% since 1993 (1). It is the second most common gynecological malignancy in the UK, with around 6,430 cases diagnosed each year (2, 3). Overall, 75 to 80% of patients present with early-stage disease and total abdominal hysterectomy with bilateral salpingo-oophorectomy remains the mainstay of treatment, with 5-year survival rates exceeding 70%. Adjuvant pelvic radiotherapy has been shown to reduce the risk of pelvic recurrence in patients with poor prognostic features, although none of the randomized trials have shown any improvement in overall survival (4-6).
A number of cytotoxic chemotherapeutic agents have shown activity in endometrial cancer, although the optimal standardized chemotherapy regimen, whether for palliation or adjuvant treatment, still remains to be determined. The following agents have been used as single agents or in combination: doxorubicin, liposomal doxorubicin, epirubicin, cisplatin, carboplatin, etoposide, cyclophosphamide, ifosfamide, paclitaxel, docetaxel, methotrexate, melphalan and vinblastine (7). Although the majority of trials investigating the role chemotherapy in endometrial cancer have included patients with advanced, recurrent, or distant metastatic disease, there is evidence to support the role of chemotherapy in the adjuvant setting either alone or in combination with radiotherapy.
Single-agent carboplatin has led to response rates of between 28 and 33%, with median survival ranging from 7.1 to 10 months in patients with advanced, recurrent or metastatic endometrial cancer (7). Single-agent epirubicin demonstrated a response rate of 25.9% and led to a median survival of 9.5 months in a small phase II study of 27 patients with advanced endometrial cancer (12). However, there are no studies using the combination of carboplatin and epirubicin chemotherapy in patients with endometrial cancer as far as we are aware of.
The aim of this retrospective study was to assess the efficacy and toxicity of carboplatin and epirubicin combination chemotherapy for patients with endometrial cancer.
Patients and Methods
Between 1999 and 2007, 43 patients with endometrial cancer were treated with carboplatin and epirubicin combination chemotherapy at our Institution. Two distinct patient groups were identified: Group 1 (n=34) included patients with endometrial cancer stage III receiving adjuvant chemotherapy; group 2 included patients with stage IV endometrial cancer (n=9). All patients in group 1 underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy with peritoneal washings with or without lymph node sampling or dissection; all patients in group 2 had biopsy-confirmed disease. Additionally, 94% of patients in group 1 (n=32) received postoperative pelvic external beam radiotherapy and vault brachytherapy. External beam therapy was delivered to a dose of 45 Gy in 25 fractions, five days a week in 1.8 Gy fractions over five weeks using an isocentric technique with standard 3- or 4-field plans. Following external-beam radiotherapy, vault irradiation was delivered using low-dose rate selectron delivering 15 Gy to 0.5 cm from the surface of applicator. Baseline characteristics of the 43 patients are summarized in Table I.
The glomerular filtration rate was calculated using the Cockcroft-Gault formula. The chemotherapy regimen consisted of a combination of carboplatin Area Under the Curve (AUC 5) and epirubicin (50 mg/m2) delivered intravenously every three weeks for 4-6 cycles. The primary end-point was progression-free survival (PFS), and secondary end-points were toxicity and overall survival (OS). PFS was calculated from the date of surgery to the date of disease recurrence or progression. Overall survival was calculated using Kaplan–Meier method and defined as the time from initial surgery to death from any cause or censored at the date of last follow-up visit.
Chemotherapy-related toxicities were evaluated by means of the common Toxicity Criteria of the National Cancer Institute (version 3.0) (13) All patients were reviewed three-weekly during chemotherapy and weekly during radiotherapy. Data for overall survival was obtained from the National Health Service strategic tracking service. Median OS and PFS were analyzed by means of the Kaplan–Meier method. Response was assessed by means of Response Evaluation Criteria in Solid Tumors (RECIST) criteria (17).
Results
Patients' characteristics. Forty-three patients with a median age of 62 years (range=47-76 years) were included for analysis in this study. All patients received chemotherapy of carboplatin with epirubicin with a median of four cycles per patient (range=1-6).
Outcomes. After a median follow-up of 37 months (range=2 to 118 months), disease in 19 patients had progressed/relapsed (12 patients from group 1; seven from group 2) and 23 patients had died (15 from group 1; eight from group 2). Out of the 19 patients in whom disease had progressed, seven (44%) had local recurrence (five patients from group 1; two from group 2), 10 (33%) had distant recurrence (seven patients from group 1; three from group 2), two patients had both local and distant recurrence (11%), and for four patients, the initial site of relapse was not documented. Out of the nine patients with papillary serous histology, disease had progressed in five; eight patients were from group 1 and one from group 2. Of all group 2 patients, 33% (3/9) had partial response, 22% (2/9) stable disease and 11% (1/9) had progressive disease; three patients were not assessable for response to chemotherapy.
Baseline demographics and characteristics of 43 patients.
The median time-to-progression was 62 months and median OS was 64 months. The median survival for patients in group 1 (adjuvant chemotherapy) was 69 months. The median survival for patients in group 2 (palliative chemotherapy) was 22 months. Cumulative PFS and OS for the entire cohort and individual groups are illustrated in Figures 1 and 2, respectively.
Toxicity. Ten patients (27.9%) experienced grade 3 or 4 toxicities. Grade 3 or 4 neutropenia was observed in 18% of patients (n=8). There were no cases of neutropenic sepsis or enteritis requiring hospitalization. Two patients were admitted and subsequently died of possibly unrelated causes. One patient developed bowel obstruction, possibly secondary to tumor progression, and another patient suffered a cerebrovascular incident, but she was known to be hypertensive. There were no cases of treatment-related cardiac failure or neuropathy. Details of chemotherapy-related adverse events are summarized in Table II.
Chemotherapy-related grade 3 and 4 toxicities.
Discussion
A number of trials have evaluated the efficacy of adjuvant chemotherapy in the adjuvant setting. In a randomized trial by the Gynecologic Oncology Group (GOG 122), doxorubicin and cisplatin combination chemotherapy was compared to whole-abdominal radiotherapy in 422 patients with advanced endometrial cancer (FIGO stage III/IV, residual tumor up to 2 cm allowed), with results showing superior PFS (50% vs. 38%) and OS (55% vs. 42%) at five years for the chemotherapy arm (8). The statistically significant benefit was seen in patients with endometrioid cancer, as opposed to serous and clear-cell histology. Our results do suggest a poor outcome for patients treated with epirubicin and carboplatin in this sub-group. However, the doxorubicin and cisplatin combination chemotherapy arm was associated with a significant increase in toxicity and high rate of pelvic relapses when compared to abdominal/pelvic radiotherapy.
A subsequent Italian randomized controlled trial comparing adjuvant cisplatin/doxorubicin/cyclophosphamide chemotherapy with standard pelvic radiotherapy in patients with stage IC, II and III endometrial cancer failed to demonstrate a disease-free or OS benefit for the chemotherapy arm (9). The Japanese GOG 2033 trial also compared pelvic radiotherapy with cisplatin-based combination chemotherapy in patients with stages IC-IIIC endometrial cancer and failed to show a benefit for the chemotherapy arm. However, in an unplanned sub-group analysis of 120 patients in the high-intermediate risk group, patients receiving chemotherapy had an improvement in OS (90% vs. 74%) and PFS (84% vs. 66%) when compared to the radiotherapy arm (10).
Comparison of acute and late chemotherapy-related toxicities
Subsequently, presented at ASCO and later published in The European Journal of Cancer (EJC) in 2007 was the NSGO-EC-9501/EORTC55991 trial of radiation alone versus adjuvant chemotherapy before or after radiation in 383 patients with stage I, II, IIIA (positive peritoneal cytology only), or IIIC disease who had high-risk factors for recurrence (14). Chemotherapy was not standardized, most patients (138/166, 83%) received doxorubicin/epirubicin with cisplatin, six patients (3.6%) epirubicin with carboplatin, five (3%) paclitaxel, epirubicin and carboplatin, and 17 (10%) paclitaxel with carboplatin. Results showed an improvement in PFS with the chemotherapy arm (7% improvement at 5 years, p=0.03), but survival data were too early to draw any conclusions (11).
GOG-177 was the first phase III trial of doxorubicin plus cisplatin with or without paclitaxel plus filgrastim in advanced endometrial carcinoma which showed that a combination with paclitaxel significantly improved Response rates (RR), PFS, and OS compared with AP. However, this was associated significantly increased neurotoxicity and hence not used routinely (15).
A Cochrane systematic review looked at 11 randomized controlled studies (2,288 patients) for the use of cytotoxic chemotherapy in patients with advanced, recurrent or metastatic endometrial cancer (6). The most commonly investigated agents were platinums, anthracyclines and taxanes, either alone or in combination. Keeping in mind the heterogeneity of the inclusion criteria and the absence of a randomized control group, the authors were unable to reach a conclusion regarding the most superior regimen in terms of PFS, OS, or effect on Quality of life (QOL). Results showed a median PFS ranging from 2.5 to 8 months and median OS ranging from 7 to 15 months demonstrating the heterogeneity, as previously discussed. Response rates ranged between 17 and 34% for single-agent and between 30 and 69% for combination-regimen. Meta-analysis of six of these trials showed that the PFS was significantly improved (p=0.004) with intensive chemotherapy regimen but this did not translate into a survival advantage. However, doxorubicin and cisplatin in combination with other drugs did offer a modest survival benefit when compared to doxorubicin and cisplatin alone. In addition, more intense chemotherapy regimens were associated with a significant increase in grade 3 or 4 toxicities when compared to less intense regimens. Similarly, the combination of paclitaxel and cisplatin, although leading to an improvement of median survival to 17.6 months, was associated with a significant increase in neurotoxicity. Although the GOG trial (7) recommended doxorubicin and cisplatin chemotherapy, this regimen was associated with a significant toxicity with 8% incident of treatment-related mortality. Grade 3 or 4 hematological toxicities reported with doxorubicin and cisplatin regimen included leukopenia (62%), neutropenia (85%) and thrombocytopenia (21%). In addition, the incidence of grade 3 or 4 gastrointestinal, cardiac and neurological toxicity was 20%, 15% and 7%, respectively.

Cumulative progression-free survival for the entire cohort and individual groups.
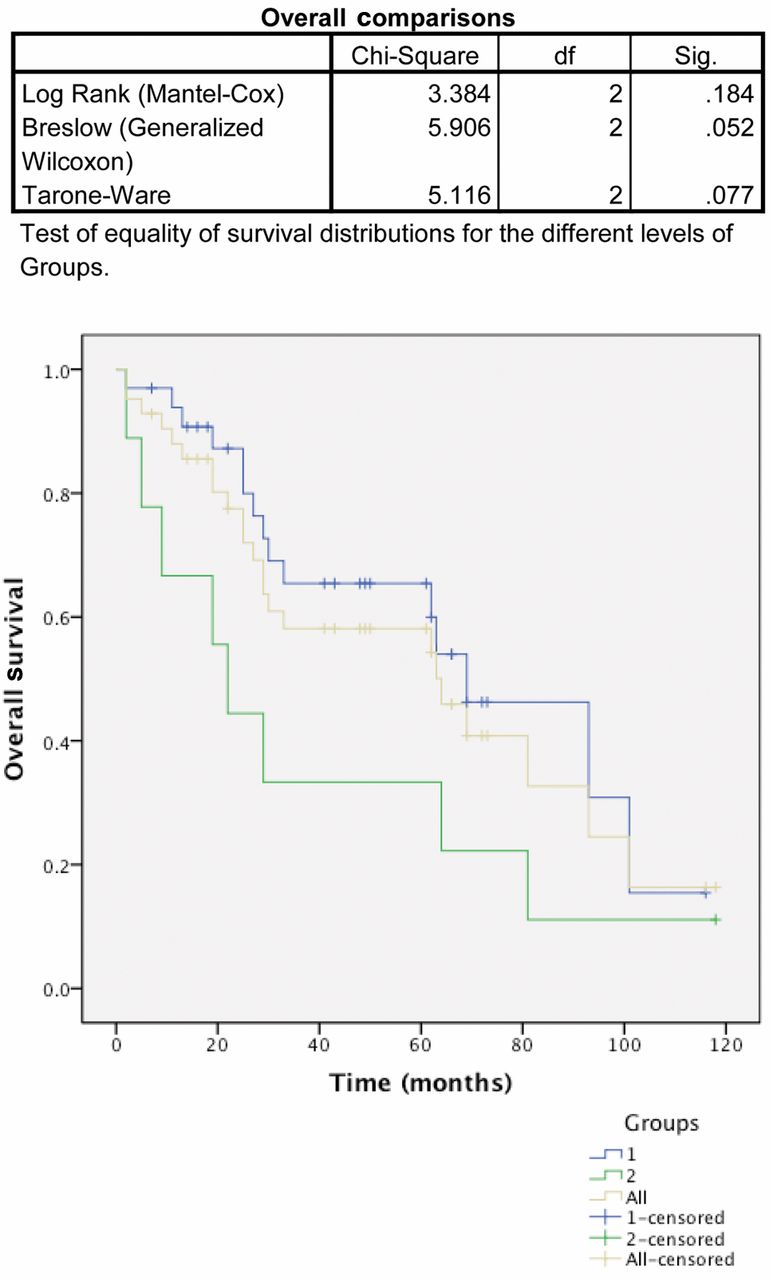
Cumulative overall survival for the entire cohort and individual groups.
Comparison of PFS and OS with published studies.
Miller et al. recently published results of a randomized phase III noninferiority trial of first-line chemotherapy for metastatic or recurrent endometrial carcinoma comparing carboplatin and paclitaxel with doxorubicin, cisplatin, and paclitaxel. Interim results showed that the former is not inferior in terms of PFS and OS (16).
Results from our study show a significant reduction in toxicities when compared to the regimens used in the GOG trials. Table III shows the comparison of acute and late chemotherapy-related toxicities of epirubicin/carboplatin, doxorubicin/cisplatin and carboplatin/paclitaxel regimens.
In the present study, carboplatin and epirubicin chemotherapy led to a median OS of 69 and 22 months in the adjuvant and palliative setting, respectively, for patients with high-risk early-stage or advanced-stage endometrial cancer. The results appear to be better with the endometrioid group as opposed to serous and clear-cell groups. This result is consistent with the GOG trial from 2006 (8). Even though the number of patients in the study is small, our results compare well with the previously published studies in terms of survival results with chemotherapy, but with a significant reduction in toxicity. Table IV shows the comparison of PFS and OS with the published studies. Advantages of this regimen over taxanes include minimal neuropathy, less use of steroids and low risk of allergic reaction and alopecia.
Conclusion
In summary, cisplatin, carboplatin, anthracyclines and taxanes appear to be the most active agents in endometrial cancer, and combination chemotherapy leads to improved response rates. There has only been one randomized trial showing superiority of chemotherapy over radiotherapy in advanced endometrial cancer. However, the chemotherapy arm was associated with significant toxicity (8).
Although there is better PFS and OS with more intense regimens, this is at the expense of increased toxicity (15).
Results from our study show that the combination of carboplatin and epirubicin is an effective alternative regimen for patients with endometrial cancer who are not fit for therapy with doxorubicin and cisplatin and where taxanes are contraindicated. This has been used in the Hogberg et al. study however where the number of patients was small (14). We are particularly likely to use this combination in endometrial endometrioid adenocarcinoma. Although we do not recommend its use for patients with papillary serous or clear-cell histology, as these may be more effectively treated with taxanes/platinum combination. In addition, treatment-related toxicity with the combination of carboplatin and epirubicin regimen is minimal when compared to published studies using anthracycline-, platinum- and taxane-containing regimens.
Nevertheless, future randomized controlled trials will be vital in deciding the most efficacious combination chemotherapy regimen with minimal toxicity for adjuvant or palliative treatment in patients with endometrial cancer. The PORTEC 3 trial is currently recruiting and comparing OS and PFS of patients with high-risk and advanced-stage endometrial carcinoma treated after surgery with concurrent radiotherapy and chemotherapy, followed by adjuvant chemotherapy, in comparison with patients treated with pelvic radiation alone (17). Patients who are not fit for this trial could be considered for this combination and its advantages over taxane-based regimens have already been discussed.
- Received March 15, 2014.
- Revision received May 15, 2014.
- Accepted May 16, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.