


Abstract
Background: The purpose of this study was to evaluate the significance of the combination of the carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9) levels as a prognostic indicator and for monitoring for recurrence and metastasis after potentially curative surgery for patients with stage II colorectal cancer. Patients and Methods: A total of 238 patients with stage II colorectal cancer who underwent potentially curative surgery were enrolled in the study. A high CEA level was defined as a level exceeding 5 ng/ml and a high CA19-9 level was defined as a level exceeding 37 U/ml. Results: Out of these 238 patients, 92 (38.7%) patients had high CEA levels, 23 (9.7%) patients had high CA19-9 levels and 15 (6.3%) patients had both high CEA and CA19-9 levels. The disease-free and overall survival rates were significantly worse in patients with both a high CEA level and high CA19-9 level. Tumor marker(s) elevated before the operation tended to be elevated again at the time of relapse. Conclusion: The combination of preoperative CEA and CA19-9 levels was useful for predicting the prognosis and for monitoring recurrence and metastasis after potentially curative surgery in patents with stage II colorectal cancer.
Although the benefit of adjuvant chemotherapy for stage III colorectal cancer has been established (1-3), the efficiency of adjuvant chemotherapy for stage II colorectal cancer remains controversial (4-7). According to the European and America guidelines (8-10), patients at high risk of recurrence after curative surgery for stage II colorectal cancer should undergo adjuvant chemotherapy. However, the definitions of high-risk patients differ in each guideline.
Carcinoembryonic antigen (CEA) has been used as a tumor marker for the diagnosis and surveillance of colorectal cancer (11-13), and CEA is considered to be a risk factor for recurrence in patients with stage II colorectal cancer in the European Society of Medical Oncology (ESMO) guidelines (8). Carbohydrate antigen 19-9 (CA19-9) has also been reported as a prognostic factor for colorectal cancer (14, 15). Therefore, the combination of these two tumor markers may provide a more sensitive biomarker for colorectal cancer.
The aim of the present study was to evaluate the prognostic significance of the combination of the preoperative CEA and CA19-9 levels in patients with stage II colorectal cancer. We also sought to clarify the correlation between the tumor marker levels and the site of recurrence or metastasis. Furthermore, we also considered the correlation between the values of preoperative tumor markers and the values at the time of relapse.
Patients and Methods
Patients. We retrospectively reviewed a database of 238 patients who had undergone curative surgery for stage II colorectal cancer in the Department of Surgical Oncology of Osaka City University between 2002 and 2009. Curative surgery was defined as the absence of any gross residual tumor from the surgical bed and a surgical resection margin which was pathologically negative for tumor invasion. Patients who received preoperative therapy were excluded from the analysis.
The patient population consisted of 138 males and 100 females, with a median age of 68 (range=32 to 90) years. One hundred and forty patients had tumors located in the colon and 98 had tumors located in the rectum.
All patients were followed-up regularly with physical and blood examinations and mandatory screening using colonoscopy and computed tomography until December 2013 or until death. A total of patients 32 patients developed recurrent disease and nine patients died.
The correlations between the preoperative Carcinoembryonic antigen (CEA)/Carbohydrate antigen 19-9 (CA19-9) levels and clinicopathological parameters.
The resected specimens were pathologically classified according to the seventh edition of the Union for International Cancer Control TNM classification of malignant tumors (16). The serum CEA and CA19-9 levels were measured using radioimmunoassay methods (Abbott, Chiba, Japan) (17, 18). The limit of detection of CEA was 0.5 ng/ml and that of CA19-9 was 2 U/ml. A high CEA level was defined as a level exceeding 5 ng/ml, and a high CA19-9 level was defined as a level exceeding 37 U/ml, according to the guidelines defined by the manufacturer of the test kit.
The significance of the correlations between the preoperative CEA/CA19-9 and the clinicopathological characteristics was analyzed using the χ2 test. The duration of survival was calculated according to the Kaplan–Meier method. Differences in the survival curves were assessed with the log-rank test. All statistical analyses were performed using the SPSS software package for Windows (SPSS Japan, Tokyo, Japan). Statistical significance was set at p<0.05.
Results
Out of the 238 patients, 92 (38.7%) patients had a high CEA level, 23 (9.7%) patients had a high CA19-9 level and 15 (6.3%) patients had both a high CEA and a high CA19-9 level. The correlations between the preoperative CEA/CA19-9 levels and the clinicopathological parameters are shown in Table I. A high CEA level did not exhibit a significant relationship with any of the clinicopathological parameters examined. A high CA19-9 level had a significant relationship only with tumor depth.
An assessment of the prognosis showed that the overall survival was significantly worse in patients of the high-CEA group, and the same result was obtained for CA19-9 (Figure 1).
We defined the tumor marker score (TMS) as follows: Patients with both a high CEA level and a high CA19-9 level were allocated a score of 2. Patients in whom only one marker (CEA or CA19-9) was high were allocated a score of 1. Patients with normal CEA and CA19-9 levels were allocated a score of 0. Figure 2 shows the survival curves of the patients sub-divided on the basis of their TMS. Although no significant difference was observed between the TMS 0 and TMS 1 groups (p=0.2768), the TMS 2 group had a significantly worse prognosis than the patients in the TMS 1 group (p=0.0043). Therefore, we divided the patients into two groups; those with TMS 0 or 1 (group A) and those with TMS 2 (group B). The disease-free and overall survival rates were significantly worse in group B than in group A (Figure 3).
The correlations between the overall survival and the various clinicopathological factors are shown in Table II. According to a univariate analysis, overall survival exhibited a significant relationship only with the TMS.
The correlations between the preoperative CEA/CA19-9 levels and the site of recurrence are shown in Table III, and the correlations between the CEA/CA19-9 levels at the time of relapse and the site of recurrence are provided in Table IV. No significant differences in these parameters were observed based on the levels of the tumor markers.
The correlation between the preoperative CEA/CA19-9 levels and the CEA/CA19-9 levels at the time of relapse is shown in Table V. The tumor marker level that was elevated before the operation tended to be elevated again at the time of relapse. Similarly, the tumor markers which exhibited a normal level were also normal at the time of relapse.

The Kaplan–Meier survival curves of the patients based on the preoperative Carcinoembryonic antigen (CEA) and Carbohydrate antigen 19-9 (CA19-9) levels. The overall survival was significantly worse in the patients with a high CEA level (p=0.0140) (A) and in the patients with a high CA19-9 level (p=0.0025) (B).
The correlations between the overall survival and the various clinicopathological factors.
Discussion
CEA and CA19-9 are the most well-known and most commonly used tumor markers for colorectal cancer. CEA is a complex glycoprotein that plays a role as an inter-cellular adhesion molecule (19). CA19-9 is the carbohydrate determinant that functions as an adhesion molecule and plays a role in the process of tumor progression (20).
These tumor markers have been used for diagnostic and surveillance purposes (21-23). Furthermore, in some previous reports, the significance of these tumor markers as prognostic factors was reported (15, 24-27). However, as CEA is included in the risk factors for stage II colorectal cancer in the ESMO guidelines (8), but is not included in the American Society of Clinical Oncology (ASCO) or the National Comprehensive Cancer Network (NCCN) guidelines (9, 10), its utility as a prognostic factor remains controversial.

Kaplan–Meier survival curves of patients subdivided on the basis of their tumor marker score (TMS). Although no significant difference was observed between the TMS 0 and TMS 1 groups (p=0.2768), patients with TMS 2 had a significantly worse prognosis than the patients with TMS 1 (p=0.0043).
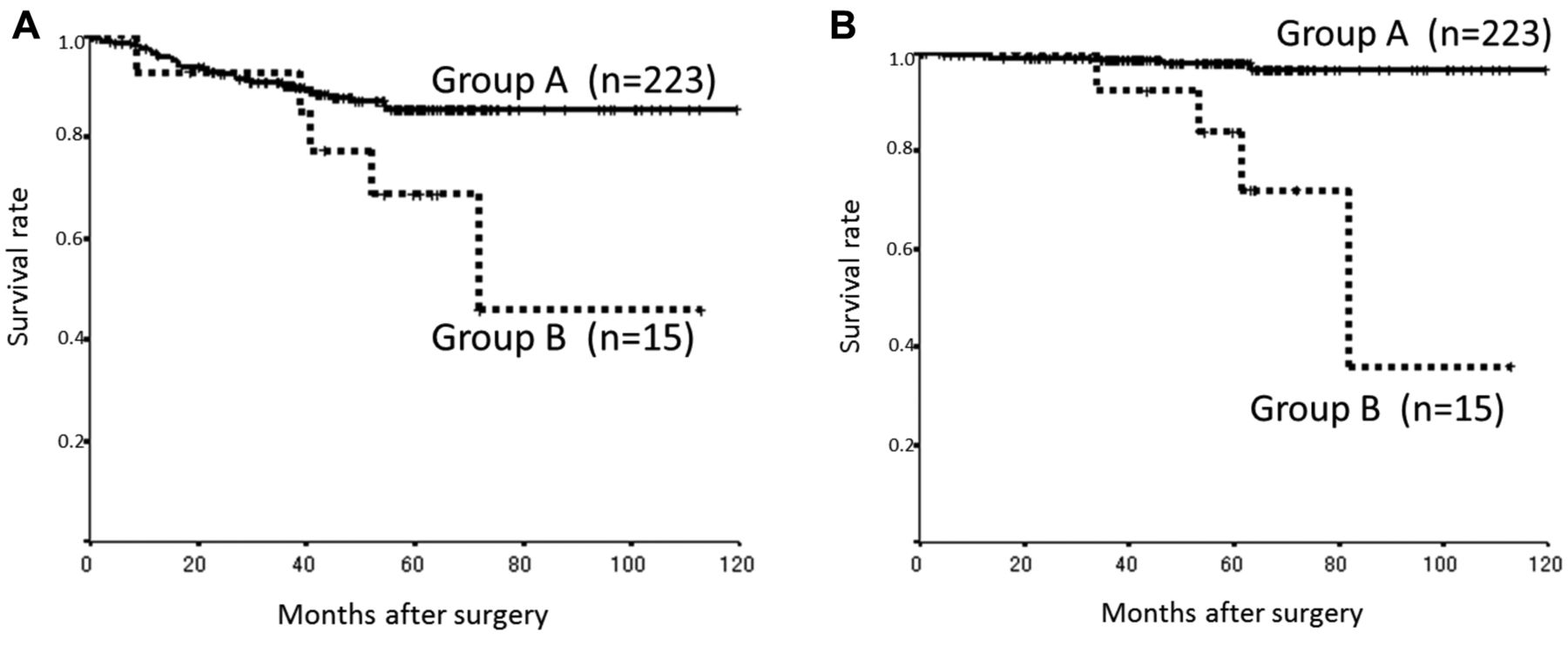
The Kaplan–Meier survival curves of the patients in the different tumor marker score (TMS) groups. The group A consists of patients with TMS 0 or 1 and the group B consists of those with TMS 2. The disease-free survival was significantly worse in group B (p=0.0339) (A). (B) The overall survival was also significantly worse in group B (p<0.0001).
The correlations between the preoperative carcinoembryonic antigen (CEA)/carbohydrate antigen 19-9 (CA19-9) levels and the site of recurrence.
In the present study, although levels of both CEA and CA19-9 were prognostic factors in patients with stage II colorectal cancer, no significant differences were observed in the disease-free survival for CEA. However, for both the overall and disease-free survival, significant differences were observed for the combination of CEA and CA19-9.
The significance and utility of monitoring the serum CEA and CA19-9 levels to detect and exclude a recurrence of colorectal cancer after potentially curative surgery have been reported in previous studies (11, 28). However, both tumor markers do not necessarily increase in all cases; sometimes only one of the two tumor markers increases. In the present study, the tumor marker which was elevated before the operation tended to be elevated again at the time of relapse. For patients with an elevation of only one out of two markers, it may be possible to increase the accuracy for detecting recurrence or metastasis by using both tumor markers for surveillance. As mentioned above, the diagnostic and prognostic utility are considered to be increased by using both CEA and CA19-9.
The correlations between the carcinoembryonic antigen (CEA)/carbohydrate antigen 19-9 (CA19-9) levels at the time of relapse and the site of recurrence.
The correlation between the preoperative carcinoembryonic antigen (CEA)/carbohydrate antigen 19-9 (CA19-9) levels and the levels at the time of relapse.
In conclusion, the combination of preoperative CEA and CA19-9 levels was useful for predicting prognosis in patients with stage II colorectal cancer. This information contributed to the identification of patients who were at high risk of recurrence and were recommended to receive adjuvant chemotherapy after potentially curative surgery. Furthermore, the combination of the preoperative levels of CEA and CA19-9 was also useful for detecting and exclude a recurrence or metastasis of colorectal cancer after a potentially curative operation.
- Received March 4, 2014.
- Revision received May 9, 2014.
- Accepted May 12, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}