


Abstract
The prognosis of advanced gastric cancer (AGC) remains poor despite therapeutic advances in recent decades. Several recent positive phase III trials established the efficacy of second-line chemotherapy for metastatic gastric cancer in prolonging overall survival. However, malnutrition and poor performance of AGC in late stages usually preclude such patients from intensive treatment. Many targeted-therapies failed to show a significant survival benefit in AGC, but have regained attention after the positive result of ramucirumab was announced last year. Among all targeted agents, only trastuzumab, a monoclonal antibody against Human epidermal growth factor receptor-2 (HER2) protein, has been proven as having survival benefit by addition to first-line chemotherapy. Herein we reported a patient who benefited from adding trastuzumab to the same second-line combination chemotherapy (paclitaxel, 5-fluorouracil, and leucovorin) upon progression of bulky liver metastases. At least five months of progression-free survival were achieved without any additional toxicity. We also reviewed literature of molecularly-targeted therapy for chemotherapy-refractory gastric cancer, including several large phase III trials (REGARD, GRANITE-1, EXPAND, and REAL-3) published in 2013-2014.
Gastric cancer (GC) is the fourth leading cause of cancer-related death and around 750,000 deaths occur each year worldwide (1). Surgical resection remains the gold standard of curative treatment, but most patients still succumb to this disease due to incurable local and distant relapses. In addition to acquired chemoresistance to this lethal disease, poor performance and malnutrition of patients with late-stage disease contribute to a grave prognosis. A platinum compound with a fluoropyrimidine is the most commonly used backbone of combination chemotherapy worldwide. Under combination chemotherapy, median overall survival for metastatic GC is still mostly less than 12 months and has not improve much in the past decade (2). For patients eligible for second-line chemotherapy, an additional one to two months of overall survival may be achieved (3-5).
Despite limited biologically-meaningful targets being found in GC, non-myelosuppressive molecularly-targeted agents remain one of the most tolerable and promising treatment choices. Trastuzumab, a human mouse chimeric monoclonal antibody specifically targeting the Human epidermal growth factor receptor-2 (HER2) protein, has been proven effective in the treatment of HER2-overexpressing breast cancer in 2001 (6). Compared to breast cancer, the rate of HER2 positivity in advanced GC is lower and varies widely with geographic distribution, ranging from 6.1% in East Asia (7) to 22.1% in Western countries (8). The pivotal phase III ToGA trial established the modest survival benefit (increase of 2.7 months of overall survival) by adding trastuzumab to first-line chemotherapy for HER2-positive advanced GC compared to combination chemotherapy-alone [5-fluorouracil (5-FU) or capecitabine with cisplatin] (8). However, the role of combination of trastuzumab to second-line chemotherapy remains unclear. Herein we report a patient who benefited from the addition of trastuzumab to the same second-line chemotherapy and at least five months of progression-free survival was achieved.
Case Report
A 62-year-old man presented to our Hospital with abdominal distension and postprandial epigastralgia of two months' duration. A huge ulcerative tumor of 15 cm in diameter, Borrmann's type II, was found at the gastric body by upper gastrointestinal panendoscopy, and pathological examination of the gastric tumor showed a well-differentiated adenocarcinoma, of the intestinal type. Staging computed tomography (CT) revealed a gastric tumor of the gastric body and multiple enlarged lymph nodes at the para-aortic region. There were also several nodules at the omentum and hypodense lesions in both hepatic lobes, and those were compatible with distant metastasis of GC. Palliative radical laparoscopy-assisted total gastrectomy with Roux-en-Y reconstruction was performed in July 2011. The pathological stage was pT4aN3bM1, stage IV. Since August 2011, low-dose everolimus (RAD001, Afinitor) plus weekly cisplatin and 24-h infusion of high-dose 5-FU (2000 mg/m2/24-h) and leucovorin (LV, 300 mg/m2/24-hour) (HDFL24) were administered as first-line chemotherapy under a clinical trial setting (9). However, scheduled assessment by CT scan showed progression of liver metastases after two cycles of treatment. Weekly paclitaxel plus 48-h infusion of higher-dose 5-FU (2750 mg/m2/48-h) and LV (HDFL48) (both on days 1 and 8, every 21 days) were given as second-line chemotherapy from September 2011 for 11 cycles. Regular evaluation of tumor response by CT scans revealed stable disease until April 2012, when they showed disease progression in multiple liver metastases.
Due to strong positivity of HER2 expression (3+) by immunohistochemical staining of the gastric tumor (Figure 1), trastuzumab (8 mg/kg, day 1 and 8, every 21 days) was added to the same regimen of second-line chemotherapy upon progression as third-line salvage therapy from June 2012 (Figure 2). No additional toxicity was observed after adding trastuzumab. During regular follow-ups, his clinical condition remained stable and the last CT scan (Figure 3) in November 2012 showed stable liver metastases. After the patient received 10 cycles of trastuzumab added to paclitaxel-HDFL48 chemotherapy, he was admitted for best supportive care in January 2013 due to progressive deterioration of peritoneal carcinomatosis, generalized ileus, and poor performance status. He tired in February 2013 due to gastrointestinal bleeding with multiple organ failure.
Discussion
The role of salvage chemotherapy as second-line treatment for advanced GC remained undetermined until 2011 when several phase III studies from Europe (3, 5) and East Asia (4) demonstrated the modest survival benefit of administering single-agent chemotherapy after failure of first-line treatment. However, for many patients, poor performance status, poor marrow function, and frequent infection resulting from peritoneal carcinomatosis contribute to their ineligibility for such therapy. Compared to cytotoxic chemotherapy, non-myelosuppressive agents could reduce the risk of infection and become a more tolerable treatment choice.
Several agents targeting different signaling pathways in GC have been investigated in first-line and second-line settings (Table I). For chemotherapy-naïve patients, the AVAGAST trial, which was conducted in 774 patients, did not meet its primary endpoint of overall survival benefit by adding bevacizumab (targeting vascular endothelial growth factor A (VEGF-A)) to cisplatin and 5-FU (12.2 months versus 10.1 months, hazard ratio(HR)=0.87, p=0.1002) (10). The EXPAND and REAL-3 trials explored the efficacy of anti-epidermal growth factor receptor (EGFR) antibodies (cetuximab and panitumumab) and both demonstrated disappointing results. Total 904 patients were enrolled in the EXPAND trial which added cetuximab to cisplatin and capecitabine. The study failed to achieve its primary end-point of median progression-free survival, which was 4.4 months in the cetuximab-containing group compared with 5.6 months in the control group (without cetuximab) (11). With a similar design, the REAL-3 study, which added panitumumab to epirubicin, oxaliplatin and capecitabine, led to even shorter overall survival in the panitumumab-containing group compared to the control group (8.8 months versus 11.3 months, HR=1.37, p=0.013) (12). The only approved targeted agent for chemotherapy-naïve GC was trastuzumab, a monoclonal antibody targeting HER2-overexpressing tumors, as mentioned above (8). The possible reason for difficulty in showing any significant superior efficacy to most agents is the lack of reliable predictive biomarkers (13). Thus, the success of trastuzumab might partially be due to its enriched patient population.
After failure of first-line treatments, only few agents have been tested in clinical trials. In the GRANITE-1 study, everolimus, an oral mammalian target of rapamycin inhibitor, did not lead to better overall survival compared to best supportive care-alone (5.4 months versus 4.3 months, HR=0.9, p=0.124) (14). The efficacy of trastuzumab as second-line treatment remains under, but lapatinib, an oral dual inhibitor targeting EGFR and HER2, did not show promising results in combination with weekly paclitaxel in the TyTAN study. The median overall survival was 11.0 months in the lapatinib-containing group compared to 8.9 months of the control group (HR=0.85, p=0.2441) (15). However, a pre-planned subgroup of patients with HER2 3+ by immunochemistry showed significantly better overall survival (14.0 months versus 7.6 months, HR=0.59; p=0.0176). Regional differences between Chinese and Japanese patients were also disclosed in this study (16) and contributed to the complexity of the results. After several disappointing results, the REGARD trial, which randomized 355 patients to ramucirumab, a monoclonal antibody VEGFR2 antagonist, or best supportive care-alone finally showed superior overall survival (17). Based on the above result, the US Food and Drug Administration granted a priority review to ramucirumab in second-line treatment of advanced GC. This is the only targeted-agent proven as having survival benefit for patients with GC who failed first-line treatment.

Moderately-differentiated adenocarcinoma, intestinal type, consisting of tumor cells in irregular tubular structures with lumens surrounded by reduced stroma (a; ×200). Immunohistochemical staining was strongly positive for Human epidermal growth factor receptor-2 (HER2) (b; ×200).

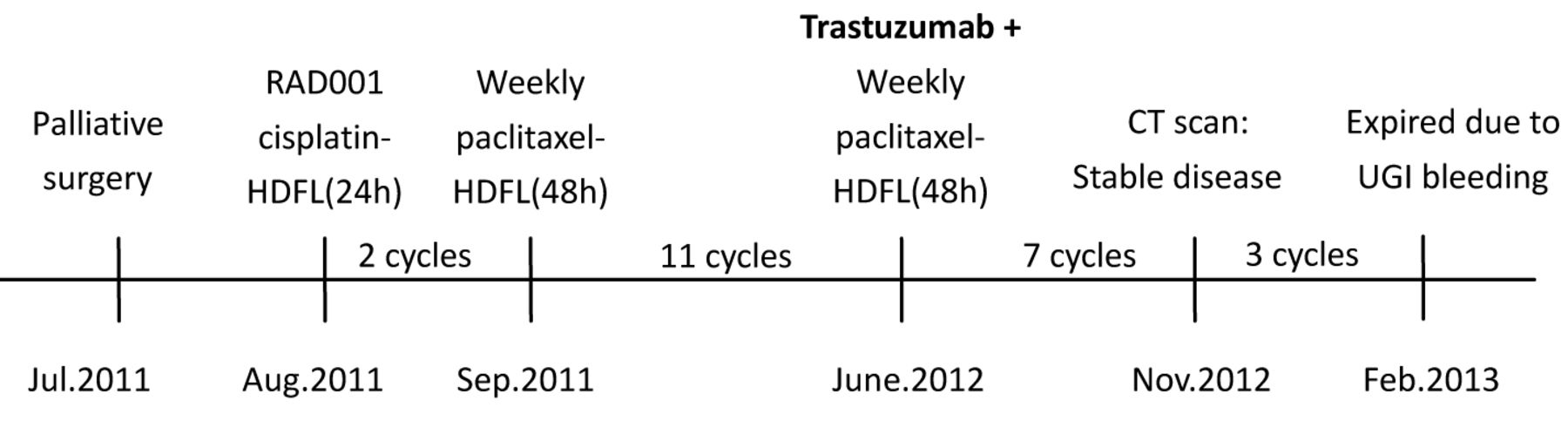
The patient received second-line chemotherapy with paclitaxel-HDFL from September 2011, and we added trastuzumab to the same regimen upon disease progression in June 2012. Follow-up computed tomographic scans in January 2013 showed mild progression of liver metastases (stable disease by RECIST 1.1). RAD001, everolimus; HDFL(24h), 24-h infusion of high-dose fluorouracil and leucovorin; HDFL(48h), 48-h infusion of high-dose fluorouracil and leucovorin.

Liver metastases of gastric cancer by computed tomography before adding trastuzumab in June 2012 (a) and five months after adding trastuzumab in November 2012 (b).
Phase III clinical trials of targeted therapies for advanced gastric cancer.
For the patient we reported above, the prolongation of progression-free survival by adding trastuzumab alone to the same second-line chemotherapy could be due merely to the single-agent activity of trastuzumab (18) or its ability to reverse resistance to chemotherapy. We administered trastuzumab with combination chemotherapy for a patient with critical liver metastases due to lack of strong evidence of the efficacy of trastuzumab monotherapy. Successful stabilization of bulky liver metastases by this adding-on strategy resulted in five months of progression-free survival and implied the value of trastuzumab in chemotherapy-refractory GC.
Current research efforts highlight the importance of solving trastuzumab resistance rather than the role of anti-HER2 therapy as second-line treatment, and a huge unmet need still exists for treatment options in second- or third-line therapies of advanced GC. With the advance of genomic analysis, the heterogeneity of GC will gradually be unveiled. When we know more about the differences in each patient, we will be closer to precise and effective treatment.
- Received March 25, 2014.
- Revision received May 21, 2014.
- Accepted May 22, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}