


Abstract
Perivascular epithelioid cell tumors (PEComas) are rare tumors driven by tuberous sclerosis complex gene mutations causing up-regulation of mTOR. We report the outcome of ten consecutive patients treated with sirolimus or temsirolimus. Patients and Methods: A retrospective analysis was performed on patients seen between 2007 and 2013. Demographic and treatment data were collected and radiological response was assessed. Results: Ten patients were investigated, eight females, with median age of 47.5 years. Nine patients received sirolimus, one temsirolimus. The median treatment duration was 128 (range=7-1,366 days). Temsirolimus was given at 25 mg IV weekly and median starting dose of sirolimus was 3 mg daily. Seven patients were evaluable for response by RECIST: 5 showed partial response (50%), 1 stable disease (10%) and 1 progressive disease (10%). Two patients progressed rapidly on treatment. One patient stopped due to grade 3 hyperlipidaemia although CT scan shows maintained response. Three patients continue on treatment while the remainder stopped due to disease progression. Conclusion: Our study confirms that mTOR inhibition with sirolimus/temsirolimus is well-tolerated with good radiological responses, albeit short-lived, and supports its use in PEComas.
Sarcomas are an uncommon and varied group of neoplasms of mesenchymal origin. Perivascular epithelioid cell tumors (PEComas) represent a very rare subset of sarcoma and comprise a family of related mesenchymal neoplasms including angiomyolipoma (AML), lymphangiomyomatosis (LAM) and clear cell sugar tumor of the lung. This family of tumors may sometimes occur in patients with tuberous sclerosis complex (TSC). PEComas tend to arise in middle age and there is a marked female predominance. They most commonly arise in the gynaecologic tract, pelvis and retroperitoneum and are of varying malignant potential (1-3).
Histologically PEComas have a perivascular distribution and may infiltrate the muscle of small- and medium-sized vessels. The precise cell type from which PEComas arise remains an enigma. PEComas are immunoreactive for both smooth muscle and melanocytic markers and exhibit a spectrum of differing behaviours. Those that arise in association with TSC are less likely to behave aggressively whilst so-called malignant PEComas tend to be of larger size (>5 cm) and to show nuclear atypia with marked pleomorphism, frequent mitoses, necrosis and evidence of vascular invasion.
The genes that are mutated in TSC are TSC1 and TSC2. The products of these two genes, hamartin and tuberin, form a heterodimer with GTPase activity that acts as an inhibitor of mTOR. Mutations leading to loss of function result in up-regulation of mTORC1 resulting in increased activity of the mTOR/S6K1/4E-BP1 metabolic pathway with increased cell growth and smooth muscle differentiation (4). Inhibition of mTOR has been reported to be of therapeutic benefit in a limited number of patients with metastatic PEComa (5-7). In the present article we describe the clinical outcomes of ten consecutive patients with metastatic PEComa treated with the mTOR inhibitors sirolimus and temsirolimus.
Patients and Methods
From 2007 until January 2013 patients with metastatic progressing PEComa were treated with sirolimus or temsirolimus at our Institution. Histological diagnosis of PEComa was reviewed and confirmed in all cases by a designated sarcoma unit histopathologist.
Treatment. All patients gave their informed consent for treatment. Sirolimus was started at 3 mg orally once daily and escalated up to 5 mg according to patient tolerability. Temsirolimus was administered at the standard weekly 25 mg intravenous dose. Patients were treated continuously until disease progression or unacceptable toxicities. Treatment breaks and dose reductions were implemented for moderate or severe toxicity.
Assessments
Efficacy. Computerized tomography (CT) or magnetic resonance imaging (MRI) scanning of the thorax, abdomen and pelvis was performed after every 2 cycles of treatment. Response assessment to treatment was evaluated according to RECIST criteria 1.1 (8) by a designated radiologist. Overall response rate (RR) was defined as the proportion of patients who achieved complete response (CR), partial response (PR) or stable disease (SD).
Progression-free survival (PFS) was defined from date of starting treatment to date of objective progressive disease or death. Any surviving progression-free patients were censored at last follow-up. Overall survival (OS) was defined from date of starting treatment to date of death from any cause where any surviving patients were censored at last follow-up. Kaplan-Meier methods were used to calculate OS and PFS and the inverse Kaplan-Meier method was used to calculate median follow-up. SPSS version 21.0 was used to summarise any descriptive statistics and to determine OS and PFS.
Safety. All patients were evaluated for safety and were monitored closely at monthly intervals. The incidence, nature and severity of adverse events (AEs) and serious AEs (SAEs) were recorded and graded using the NCI Common Toxicity Criteria for Adverse Events version 4.0.
Results
Demographics. Ten patients with metastatic PEComa were seen between 2007 and 2013. Five had metastatic disease at first presentation to our hospital. The majority were women (70%) with a median age of 47.5 years. Most patients had a WHO performance status 0-1 at baseline (90%). Primary sites of origin were renal, gynaecological or gastrointestinal tract. Most patients had prior surgery (70%). Lung, liver and bone were the most frequent metastatic sites. None of these patients had a history of tuberous sclerosis or demonstrated any signs of symptoms compatible with this disease. Patient demographics are summarised in Table I.
Treatment. Nine patients received an mTOR inhibitor in the first-line metastatic setting. One patient (patient 7), with renal PEComa, was previously treated with chemotherapy. He achieved a partial response after 2 cycles of doxorubicin which was sustained after a total of 8 cycles. However the response was short-lived and the patient progressed within 2 months of chemotherapy cessation. He was subsequently treated with temsirolimus which was available through an expanded access programme. The remaining nine patients received sirolimus. The median dose attained was 4 mg daily and median duration of treatment was 128 days (range 7-1366 days), mean 296 days. Individual results are summarised in Table II.
Patient demographics
Following disease progression three patients received further systemic treatment. Two patients received conventional ‘sarcoma-type’ chemotherapy with doxorubicin resulting in clinical and radiological disease progression after ≤2 cycles. Two patients took part in Phase I clinical trials and one received thalidomide, also with subsequent disease progression
Safety and toxicity. Treatment toxicity was managed by dose reductions and treatment breaks. Of the nine patients on sirolimus, five had dose reductions and four had dose interruptions. One patient (Patient 2), who received sirolimus for the longest period of time, developed clinically significant hyperlipidaemia with grade 3 hypertriglyceridaemia, grade 4 hypercholesterolaemia and grade 2 hyperglycaemia. The patient was commenced on atorvastatin and gliclazide with subsequent improvement in these parameters and has now been off sirolimus for 275 days. Subsequent radiological assessment has shown maintained partial response.
Treatment was discontinued in seven patients. The primary reason for discontinuation was disease progression in six patients and grade 3 thrombocytopenia in the remaining one patient. Three patients remain on treatment at the time of reporting.
Treatment toxicities were generally mild and manageable. Oral mucositis was most commonly reported and responded well to both local measures and also dose reduction. Treatment-related toxicities are summarised in Table III. No treatment related deaths were recorded.
Efficacy. Seven patients were evaluable for response by the RECIST criteria. Of the remaining three patients two had clinically significant deterioration within the first 16 days of treatment and sirolimus therapy was withdrawn. The final patient moved to another institution and derived clinical benefit with symptomatic improvement from treatment with sirolimus for 217 days until disease progression. However imaging was not available for radiological review.
Results treatment duration and response
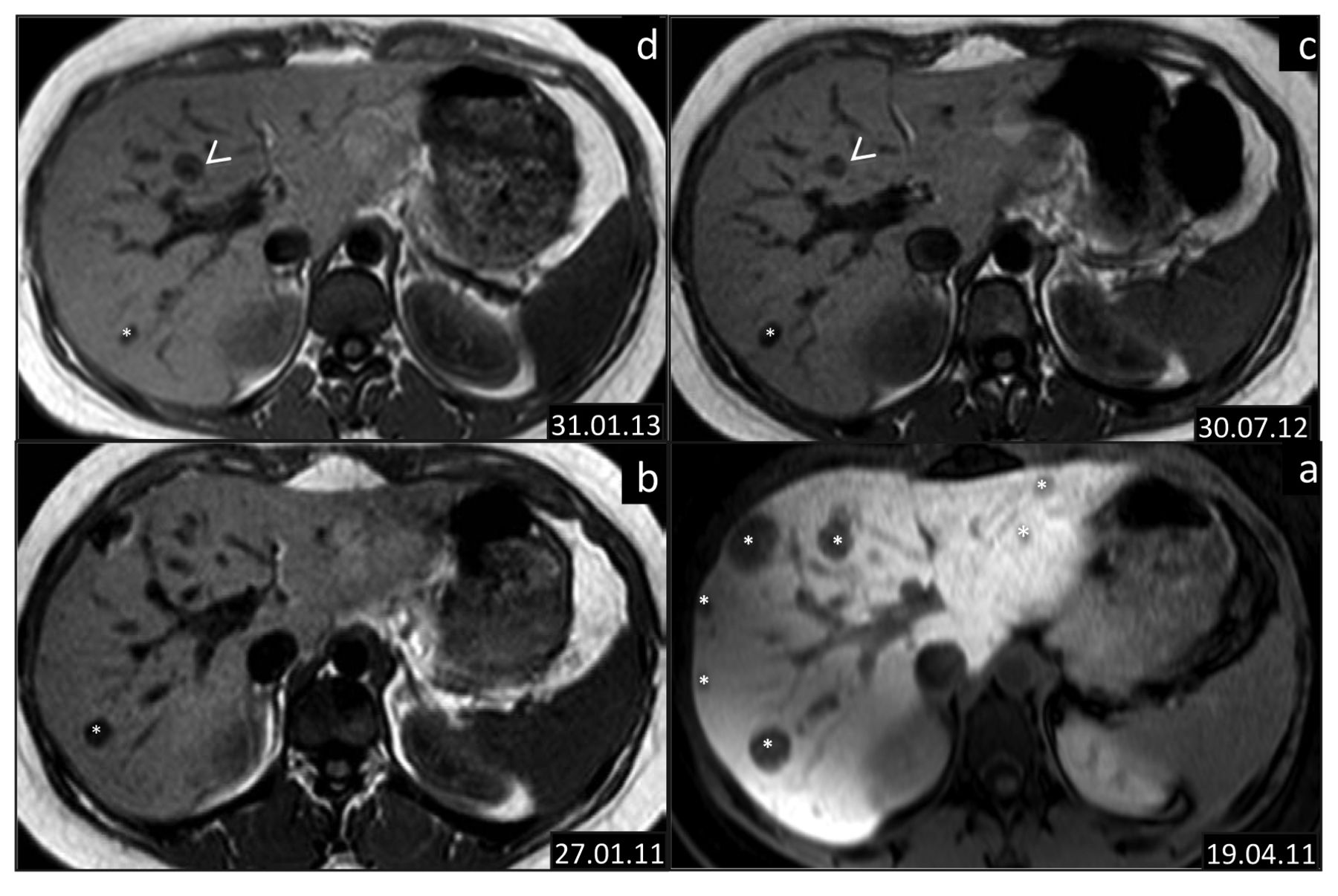
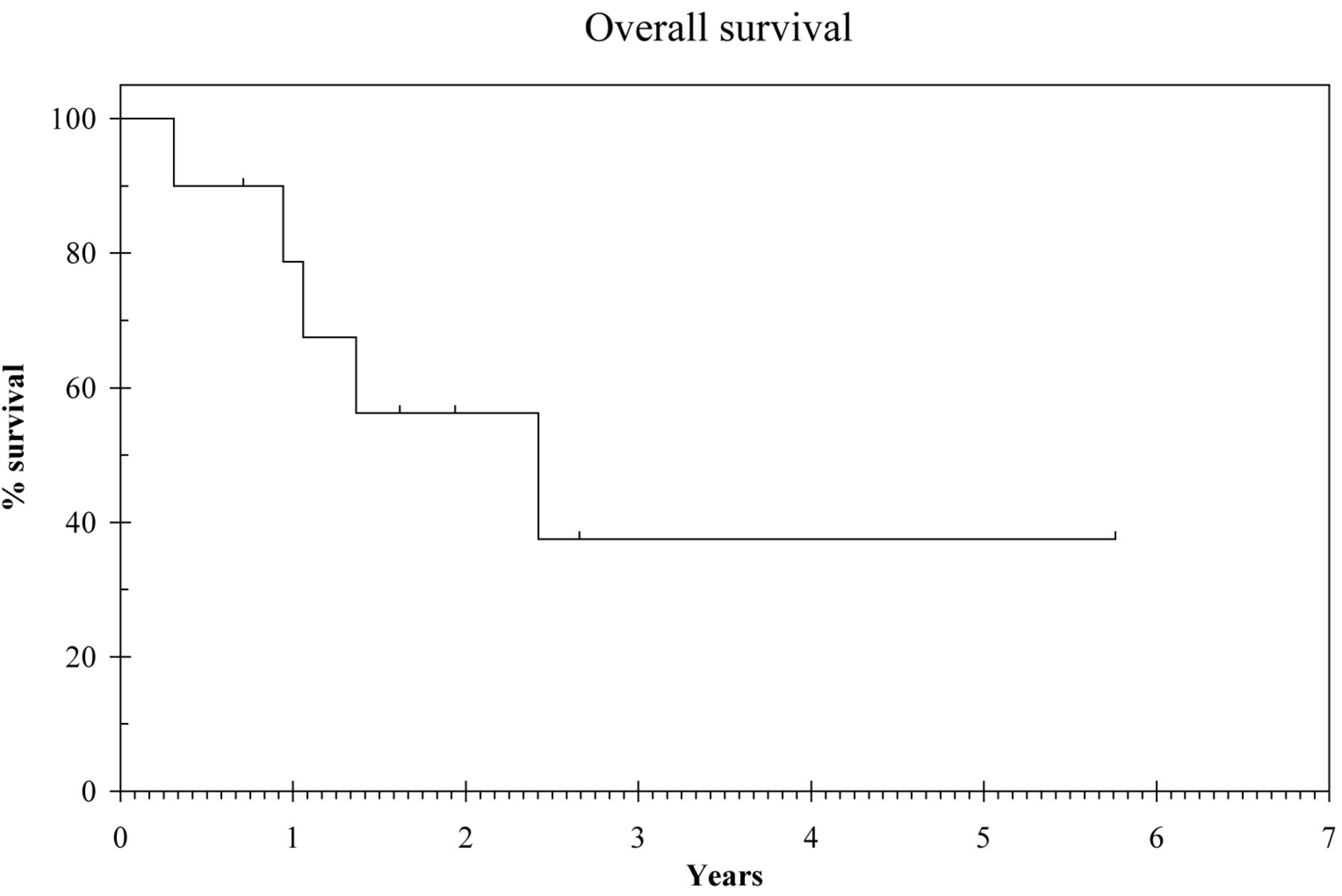
RECIST partial response was observed in 5 out of the 7 evaluable patients with reduction in tumour size and contrast enhancement (density) (Figure 1). Furthermore symptomatic responses were documented in 7 out of 10 of patients with reduction in analgesic requirements on chart review. Median duration on treatment was 187.5 days. The 1-year survival rate was calculated at 78.8% with a median overall survival of 2.4 years (95% CI 0.3-4.5) and a median follow up of 1.9 years (Figure 2).
Discussion
The investigated cohort of 10 patients with PEComa treated with the mTOR inhibitors sirolimus or temsirolimus represents the largest single case series to date. Response to mTOR inhibition in PEComas was first published by Wagner et al. in 2010 reporting a series of 3 patients with metastatic disease (5). Radiological responses were noted in all 3 patients with complete response noted in one, and disease control, albeit short-lived noted in the remaining two. Furthermore correlative studies were performed on patient tumour sections revealing activation of mTORC1, providing a strong biological rationale for treatment. This report directly followed on from a series of 25 patients with the closely-associated disease types AML and LAM who were treated with sirolimus for 12 months. A significant decrease in tumour volume was noted whilst on treatment. (53.2%+/- 26.6%, p<0.001) which then increased in most but not all patients when treatment was stopped (9). Two other small PEComa case series have since been published confirming the activity of sirolimus in this disease (6, 7). A case of neo-adjuvant response to sirolimus in a locally-advanced PEComa has been reported, as well (10). Prior to this discovery, experience in treating metastatic PEComa confirmed that there was no proven role for chemotherapy, and the prognosis for patients with metastatic disease was poor.
Treatment toxicities
Clearly in a group of patients with such limited therapeutic options, optimising therapy is critical. In our own group of patients on sirolimus we pragmatically used development of oral mucositis, a common mTOR inhibitor side-effect, as a surrogate for pharmacologically-active drug levels. Other groups have incorporated therapeutic drug level monitoring into their dosing strategy. Much of the pharmacokinetic data for sirolimus has been extrapolated from earlier studies in renal transplant patients. A phase I study with sirolimus (rapamycin) in patients with solid tumours defined a maximum tolerated dose of 6mg and pharmacokinetic analysis showed that drug exposure increased proportionally with dose (11). Some groups have used the renal transplant therapeutic trough plasma level range of 15-20 ng/ml as a guide to therapeutic dosing (6, 7) with dose escalation of sirolimus where necessary. CYP3A4 inhibition with either ciproxin or grapefruit juice has also been explored in order to increase sirolimus trough levels (6, 12). Certainly in a patient who does not initially respond to sirolimus, dose escalation seems a reasonable approach, perhaps in conjunction with assessment of trough levels of drug.
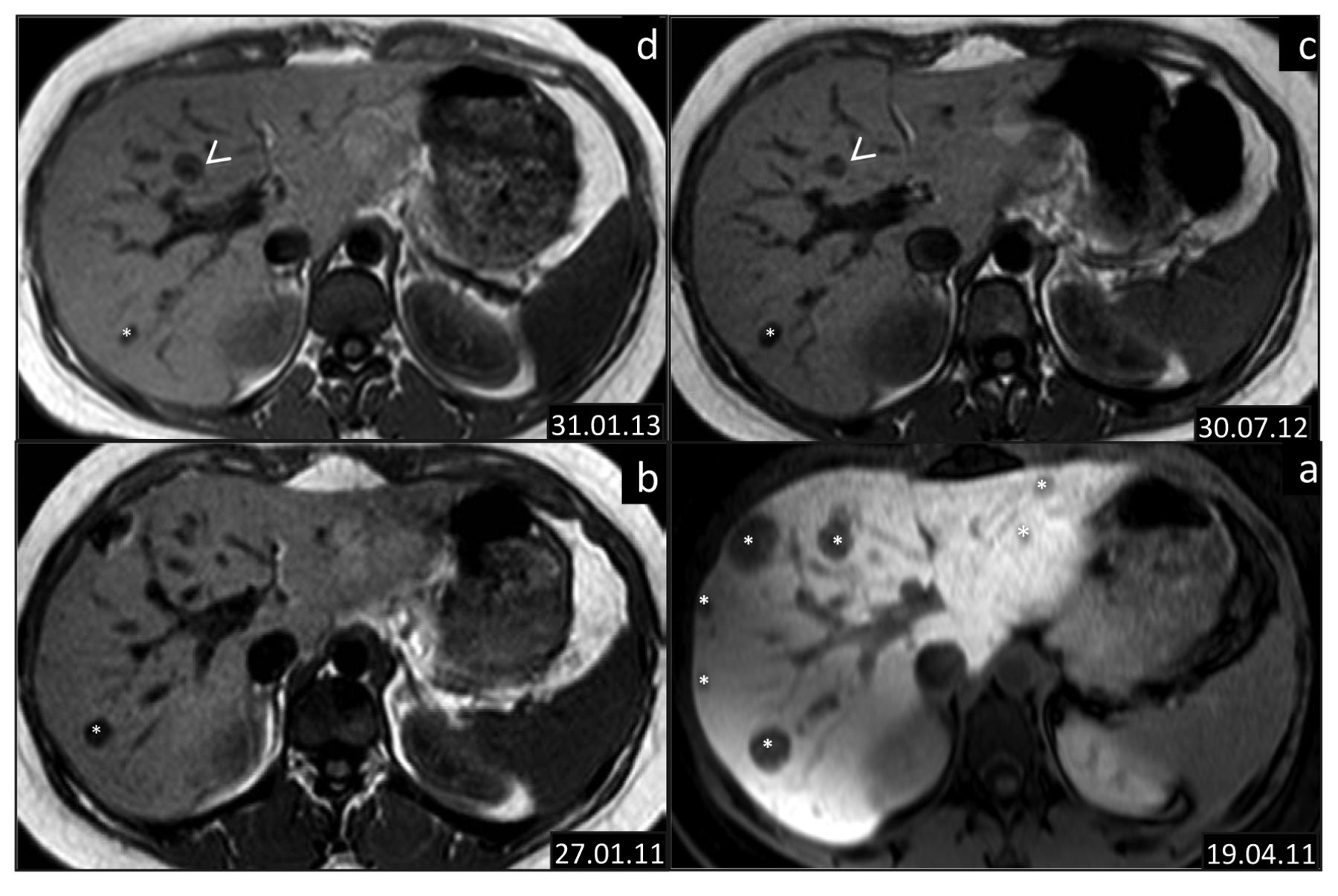
Serial axial T1weighted MRI images though the liver in a 26 years old PEComa patient treated with sirolimus. The baseline examination at the referring hospital was performed following Gadolinium administration. Subsequent examinations at our institution were performed without administration of Gadolinium. (a) The baseline examination shows multiple liver metastases (*); an excellent response after 3months on sirolimus (b) with reduction in size and number of the liver metastases; a target lesion in segment VII measures 13mm compared to 20mm at baseline. July 2012 MRI (c) shows a maintained response in the preexistent metastatic liver disease with further reduction in size of the target lesion (10mm) but development of a new 8mm liver lesion (arrow). In view of the excellent response elsewhere the patient continued on Sirolimus until January 2013 (d) when treatment is discontinued due to progression in the pelvic disease (not shown); note is made that the target Segment VII lesion continues to decrease in size (7 mm) whilst the new lesion has moderately enlarged measuring 10 mm.
The original phase I study incorporated pharmacodynamic markers with inhibition of p70SK expression in peripheral blood, skin and tumour biopsies although no pharmacokinetic/pharmacodynamic correlation was seen (12). Other immunohistochemical analyses of tumours have been performed, in particular to understand why some patients are irresponsive. The role of correlative studies in future studies in this group of patients might help to predict both response and resistance to treatment.
RECIST v.1.1 criteria were used to assess the effects of sirolimus in this cohort and is the most commonly used system in oncology for response analysis. Given the response characteristics of this tumour group there could well be a role for incorporation of Choi criteria which also takes into account CT contrast enhancement/tumour density and has already been incorporated into assessment of other sarcoma subtypes especially gastrointestinal stromal tumour (GIST), as first described (13). Magnetic resonance imaging (MRI) with diffusion-weighted imaging sequences may also be a valuable tool, especially as treatment-related intra-tumoral haemorrhage has been observed in our cohort of patients. The role of other functional imaging would be interesting to explore in the context of prospective clinical trials.
Other available mTOR inhibitors such as everolimus have also been reported to be active in this tumour type confirming that what has been observed is an mTOR class effect (14). Furthermore the role of everolimus has been confirmed in a large randomised placebo controlled trial in patients with AML (15). Everolimus might be more effective than sirolimus given its improved pharmacokinetic profile but any such benefit is currently limited by increased cost, as sirolimus is available as a generic agent.

Overall survival: at a median follow-up of 1.9 years, median OS was 2.4 years (95% IC: 0.3-4.5), with a 1-year survival rate of 78.8%.
As demonstrated in the present and other series, prolonged responses to sirolimus may be seen. Therefore, management of treatment toxicity is an important consideration utilising both dose reductions and drug holidays. In our experience sirolimus is well-tolerated with no major impact on quality of life. Initial monthly monitoring of laboratory values is recommended which may then be stretched out to 3-monthly administration. As demonstrated by our long responder glucose and lipid profiles should be measured regularly. A recent review has been published raising awareness of metabolic effects of patients receiving drugs targeting the PI3 kinase-AKT-mTOR pathway. Regular monitoring of blood glucose and lipid profile is recommended and timely intervention with lipid lowering agents and oral hypoglycaemics in the first instance prior to dose modification or discontinuation of treatment (16). The risk of pneumonitis with temsirolimus should also be highlighted although not seen in our patient (17).
The role of mTOR inhibition has recently shown promise in other sarcoma sub-types. The SUCCEED investigated the use of maintenance treatment with the mTOR inhibitor ridaforolimus versus placebo in patients with metastatic sarcoma following benefit from prior chemotherapy (18). The toxicity profile was similar to that of sirolimus and there was a small but statistically significant benefit in progression free survival of 3 weeks duration. Haemangioendothelioma, another rare sarcoma subtype with varying clinical behaviour and a paucity of proven treatment strategies may also respond to treatment with sirolimus (12, 19).
The question of which therapeutic options to consider in PEComa following disease progression is a difficult one, particularly as the mechanism of drug resistance is poorly-understood. Options include dual mTORC1/2 inhibitors currently in early clinical trials, or PI3 kinase inhibition, or possibly combinations of mTOR and insulin like growth factor-1 receptor (IGF1R) inhibitors. Pragmatically this may depend on availability of phase I trials locally. The principal difficulty surrounding such research is the extreme rarity of this disease type and outlines the importance of collaboration through organisations such as the EORTC, SARC (Sarcoma Alliance for Research through Collaboration) and World Sarcoma Network.
Conclusion
This is the largest series to date of patients with PEComa treated with mTOR inhibitors and confirms that this should be the recommended first-line treatment in this rare disease type. Further studies are required with correlative markers and functional imaging to understand the determinants of response and mechanisms of acquired resistance.
Acknowledgements
Clinical nurse specialists: Alison Dunlop, Rolyn Alvarado, Cerys Propert Lewis and Sam Hackett. We acknowledge support from the NIHR RM/ICR Biomedical Research Centre.
Footnotes
-
Conflicts of Interest
None.
- Received March 26, 2014.
- Revision received May 23, 2014.
- Accepted May 26, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Acute haemorrhage from a large renal epithelioid angiomyolipoma: diagnostic and management considerations in a teenage patient with a rare cancer
- Primary retroperitoneal PEComa: an incidental finding
- Role of Chemotherapy, VEGFR Inhibitors, and mTOR Inhibitors in Advanced Perivascular Epithelioid Cell Tumors (PEComas)
- 2018 ESMO Sarcoma and GIST Symposium: 'take-home messages in soft tissue sarcoma
- Treatment of Advanced Malignant Uterine Perivascular Epithelioid Cell Tumor with mTOR Inhibitors: Single-institution Experience and Review of the Literature
- Soft Tissue Sarcoma, Version 2.2016, NCCN Clinical Practice Guidelines in Oncology
- Perivascular epithelioid tumours (PEComas) of the gynaecological tract