


Abstract
Background/Aim: Intrapelvic bleeding after extended pelvic surgery is fatal, but few reports have addressed this serious situation. The objective of the present study was to evaluate the short-term clinical outcome of this complication. Patients and Methods: This study was a retrospective medical chart review of 130 patients who underwent extended pelvic surgery between 2000 and 2012 at our Institute. Based on the classification of the bleeding pelvic artery, how initial hemostasis and control of secondary pelvic abscess were mainly evaluated. Results: In 6 patients, bleeding involved a peripheral artery (peripheral group) and 4 a main artery (central group). For initial hemostasis, interventional radiology was efficacious. Compared to the peripheral group, even if initial hemostasis succeeded, unsatisfactory abscess drainage easily became fatal in the central group. Conclusion: Aggressive surgical abscess drainage should be considered at an appropriate time for optimal survival in patients with involvement of a main artery with insufficient tube drainage.
Because of recent advances in surgical technique, the morbidity and mortality rate for pelvic surgery including low anterior resection or Hartmann procedure for primary rectal cancer could be much lower. However, as typified by total pelvic exenteration and sacral bone resection for locally recurrent rectal cancer (LRRC), extended pelvic surgery has been reported to be a high-risk operation (1-3). Serious complications include pelvic abscesses (PAs), with a reported incidence of 20-30% in most series (4-6). PA frequently develops after extended pelvic surgery as a result of a large pelvic defect and can cause severe infection and septicemia (4). Most cases with PA can be treated with indwelling or additional percutaneous tube drainage, but prolonged insufficient abscess drainage can result in erosion of the intrapelvic artery and lead to intrapelvic bleeding (IPB). The complication rate of IPB has been reported to be 2.4-13% (7-10). This complication is often fatal and commonly requires multi-modal treatment including interventional radiology (IVR), such as transcatheter arterial embolization (TAE) and stent grafting (SG), or a surgical procedure. In the clinical setting, there is no consensus regarding the management of postoperative hemorrhage of arterial origin (11). Although the number of published reports on this complication in pelvic surgery is small (12, 13), further analysis has been carried out in the field of pancreatobiliary surgery (14, 15). The main cause of bleeding after a pancreatobiliary operation was found to be the rupture of arterial pseudo-aneurysms of the surgical field originating from an abdominal abscess because of a pancreatic fistula (16, 17). Hemostasis by IVR, such as with SG, has been quite efficacious for the emergency treatment of pseudo-aneurysms (18-20). Hemostasis by IVR and subsequent proper tube abscess drainage may be the best minimally-invasive treatment method for care in the field of pancreatobiliary surgery (21-23).
Compared to pancreatic surgery, in the field of pelvic surgery, even if IPB related to PA can be stopped by initial IVR, another problem remains regarding residual intrapelvic hematoma in a large pelvic defect that can exacerbate the PA. Moreover, insufficient PA drainage and the indwelling catheter as a foreign body, working together, can lead to refractory septicemia. There is a need to consider whether additional surgical hematoma drainage is necessary.
The aim of the present study was to document the etiology of IPB and evaluate management strategies for it.
Profiles of 10 patients suffering from intrapelvic bleeding after extended pelvic surgery.
Patients and Methods
From 2000 to 2012, a total of 130 patients underwent extended intrapelvic surgery at the Department of Gastroenterological Surgery, Osaka University Hospital. Extended intrapelvic surgery was defined: surgery with the resection of adjacent organs such as bladder, prostate, uterus and sacrococcygeal bone; re-operation for LRRC after curative resection of primary rectal cancer. Of the 130 patients eligible by these criteria, 10 (7.7%) suffered from postoperative IPB. To analyze the clinical features of IPB, we divided the patients into two groups: the central group, with bleeding from the internal iliac artery, external iliac artery, or common iliac artery; and the peripheral group, with bleeding from a peripheral branch of any of these three. Our study ultimately consisted of six patients in the peripheral group and four patients in the central group.
Table I gives a summary of the patient demographics in this study. Seven patients were female (70%), and the median age was 62 years (range=50-71 years). Diagnoses at initial surgery were locally recurrent rectal cancer (n=8), primary rectal cancer (n=1), and entero-urethral fistula post-surgery for LRRC (n=1). Nine out of 10 patients underwent preoperative treatment (chemo-radiation therapy in seven, chemotherapy in one, and heavy ion therapy in one). We started preoperative chemo-radiation therapy (CRT) since 2004 with the aim of preventing local re-recurrence after surgery for LRRC. Three-dimensional radiation administered five-times a week at a total radiation dose of 50 Gy with a daily fraction of 2 Gy with UFT/LV plus CPT 11 regimen. Radiation was targeted to the LRRC, the retroperitoneal soft tissue and the front of sacral coccygeal bone at the center of irradiation field.
The main surgical procedures were total pelvic exenteration in six patients (60%) and sacral bone resection in three (30%). In two patients, in order to fill the pelvic dead-space to prevent PA, an anal-preserving procedure was performed (4). Additional procedures such as omental flap/vertical myocutaneous rectus abdominis were performed in all patients. How to re-fill the pelvic dead space was individually decided intraoperatively. If possible, VRAM was performed. It was confirmed that the dead space was re-filled using omentum or VRAM in all cases. Drain tubes were placed at the bottom of the pelvic floor intraoperatively.
The clinical characteristics of the patients were collected, including age, gender, primary disease, preoperative treatment, surgical procedure, cause of IPB, the presence of septicemia, sentinel bleeding, bleeding site, massive bleeding day(day of onset of massive bleeding), initial treatment for IPB, additional percutaneous tube drainage, PA control and outcomes. PA was clinically diagnosed by fluid collection confirmed on computed tomographic (CT) scan without other infectious focus or purulent drainage in the patients under septicemia. Poor PA control was defined as follows: regardless of additional percutaneous drainage tube replacement, drains could not be withdrawn earlier than two months due to residual PA/prolonged purulent drainage. The treatment method of IVR for hemostasis was decided by the individual radiologists.
Results
Diagnosis of IPB. Table II shows the diagnoses of IPB. All patients except patient no. 6 suffered from PA for a long period of time leading to IPB and peripheral type IPB in patient no. 6 was due to delayed heat burn. Sentinel bleeding was found in three out of six patients in the peripheral group and in three out of eight patients in the central group. The median day of onset of sentinel bleeding was 23 postoperative days (POD) (range=22-43 POD) in the peripheral group and 5 POD (range=4-48 POD) in the central group. When massive bleeding occurred, enhanced CT scan was in most cases performed immediately before angiography. In detail, in the peripheral group, extravasation was detected in two, hematoma in one, bloody ascites in two, and PA in two patients. In the central group, extravasation and hematoma were not detected, bloody ascites was detected in one, and PA in two patients.
Diagnosis of intrapelvic bleeding.
Clinical course after initial treatment for intrapelvic bleeding.
In the peripheral group, IVR for the initial treatment with hemostasis was selected for five patients; angiography showed pseudo-aneurysm or extravasation in one and five patients, respectively. In the central group, IVR was performed in three patients; angiography showed pseudo-aneurysm or extravasation in one and three patients, respectively.
a: Angiography indicated extravasation from right external iliac artery at the site repaired during the initial operation (arrow). b: The covered stent graft fully expanded to shield the hole of external iliac artery. The post-stenting angiography showed diminishment of extravasation and good flow to the distal. c: Emergent enhanced pseudo-aneurysm (arrow) around the stent graft (arrow head) replacement site of the external iliac artery was shown on the enhanced CT scan.
Initial treatment for IPB and subsequent clinical course. Table III shows the initial treatment for IPB and the subsequent clinical course. In five peripheral cases with initial IVR, gel sponge, coiling, or n-butyl-2-cyanoacrylate (NBCA) was used for transcatheter embolization of the bleeding artery. Hemostasis was achieved with single IVR treatment, except for patient no. 3 who required IVR twice. Although having recovered from IPB by initial treatment, all patients required subsequent treatment for PA later and finally obtained good PA control by tube drainage-alone. All four patients in the central group who received IVR required SG replacement for hemostasis.
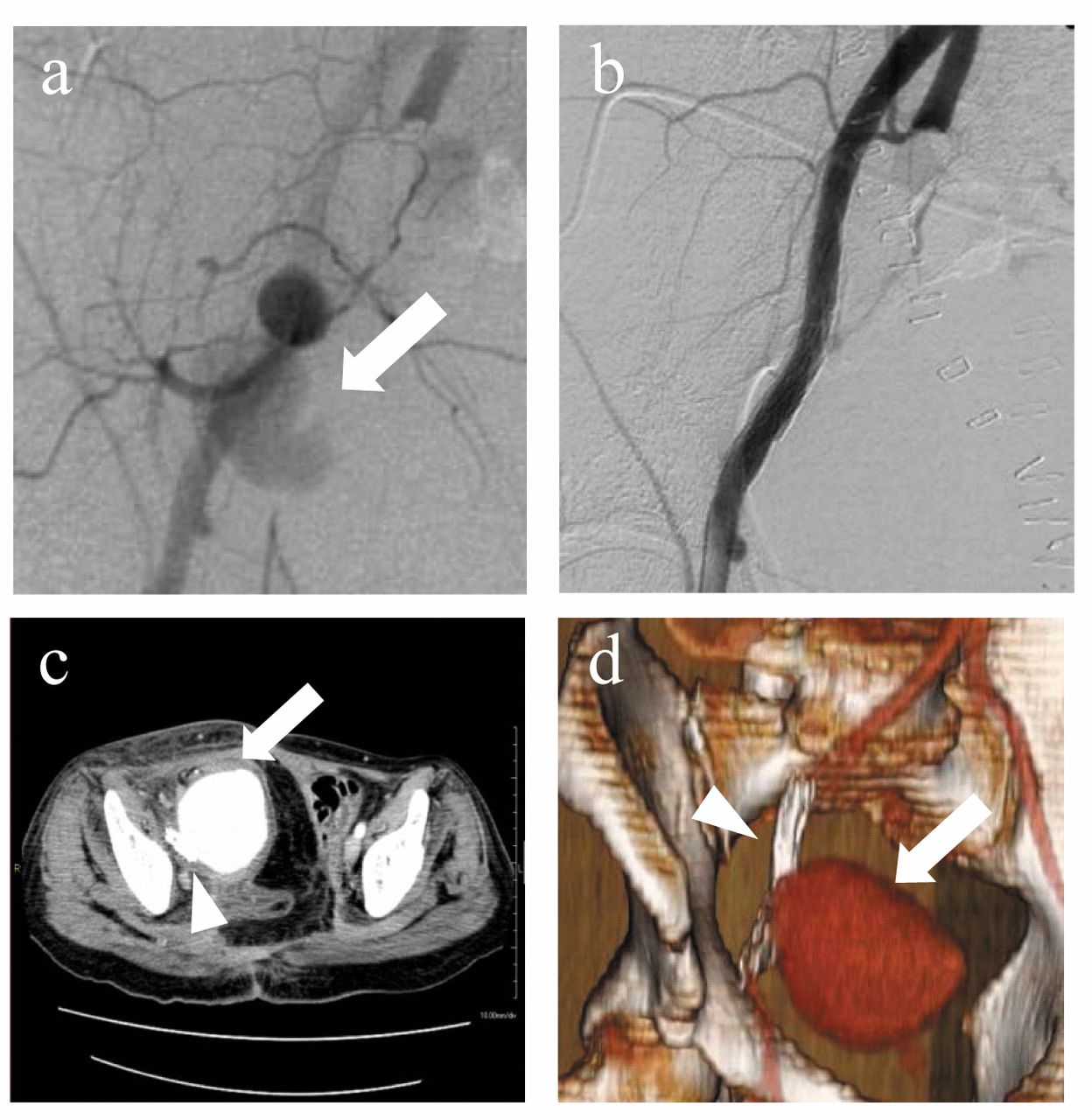
Compared to the peripheral group, only one patient obtained good PA control by tube drainage alone, the remaining two had to undergo prolonged tube drainage. In one out of these two, secondary hemorrhage from insufficient tube drainage occurred at 67 POD, and immediate enhanced CT scan revealed a giant pseudo-aneurysm around the SG replacement. Emergency surgical drainage and F-F bypass were performed, resulting in survival (Figure 1). On the other hand, although another patient progressed through the clinical course with insufficient tube drainage, there was neither secondary hemorrhage nor formation of pseudo-aneurysm, but there was an enlargement of the PA around the SG detected on the enhanced CT scan (Figure 2). Finally, the patient died from untreatable septic shock at 128 POD.
Overview of the short-term clinical outcomes and prognosis in this study. Figure 3 provides an overview of the clinical courses in this study. Initial TAE with gel sponge, coiling, NBCA, and subsequent tube drainage was the appropriate strategy in the peripheral group. In contrast, in the central group, insufficient PA control did lead to secondary events including re-hemorrhage or untreatable septicemia. In those cases with insufficient tube drainage, additional surgical drainage should be considered with appropriate timing.
Discussion
Faced with IPB after extended pelvic surgery, we should determine the treatment approach considering two important aspects: the necessity for urgent hemostasis and prevention of secondary PA formation from residual hematoma. Arterial hemorrhage can easily be fatal if emergency hemostasis within the stable hemodynamic state is not possible. In addition, not only hemostasis but also prevention and treatment of PA are important for survival. As a characteristic of extended pelvic surgery, a large dead space in the pelvis can accelerate the formation of PA from residual hematoma (24, 25).

a: Emergent angiography demonstrated extravasation from right common iliac Artery (arrow). b: Angiography demonstrated covering the extravasation site using stent graft resulted in successful hemostasis. c: Follow-up enhanced CT scan showed gradual enlargement of infectious hematoma around the stent graft replacement site (arrow).
The present study showed that the incidence of IPB was 7.7%, comparable with other previous reports (7, 8, 10). Although IPB after extended pelvic surgery is a serious situation, requiring for appropriate and quick decision-making, there have been no reports clearly describing treatment strategies. Thus, we retrospectively examined the clinical course of our case experiences at our facility.
In diagnosis of IPB, sentinel bleeding was helpful. Sentinel bleeding was defined as gastrointestinal or intra-abdominal intermittent and small-volume hemorrhage occurring 6 h to 10 days prior to massive arterial hemorrhage (26). Some reports have demonstrated the possibility of sentinel bleeding as being an important preceding sign of massive arterial hemorrhage (27, 28). In our study, sentinel bleeding was detected more in the central group than in the peripheral group (3/6 vs. 3/4). In these patients with sentinel bleeding, an enhanced CT scan on the day that the sentinel bleeding occurred revealed PA.
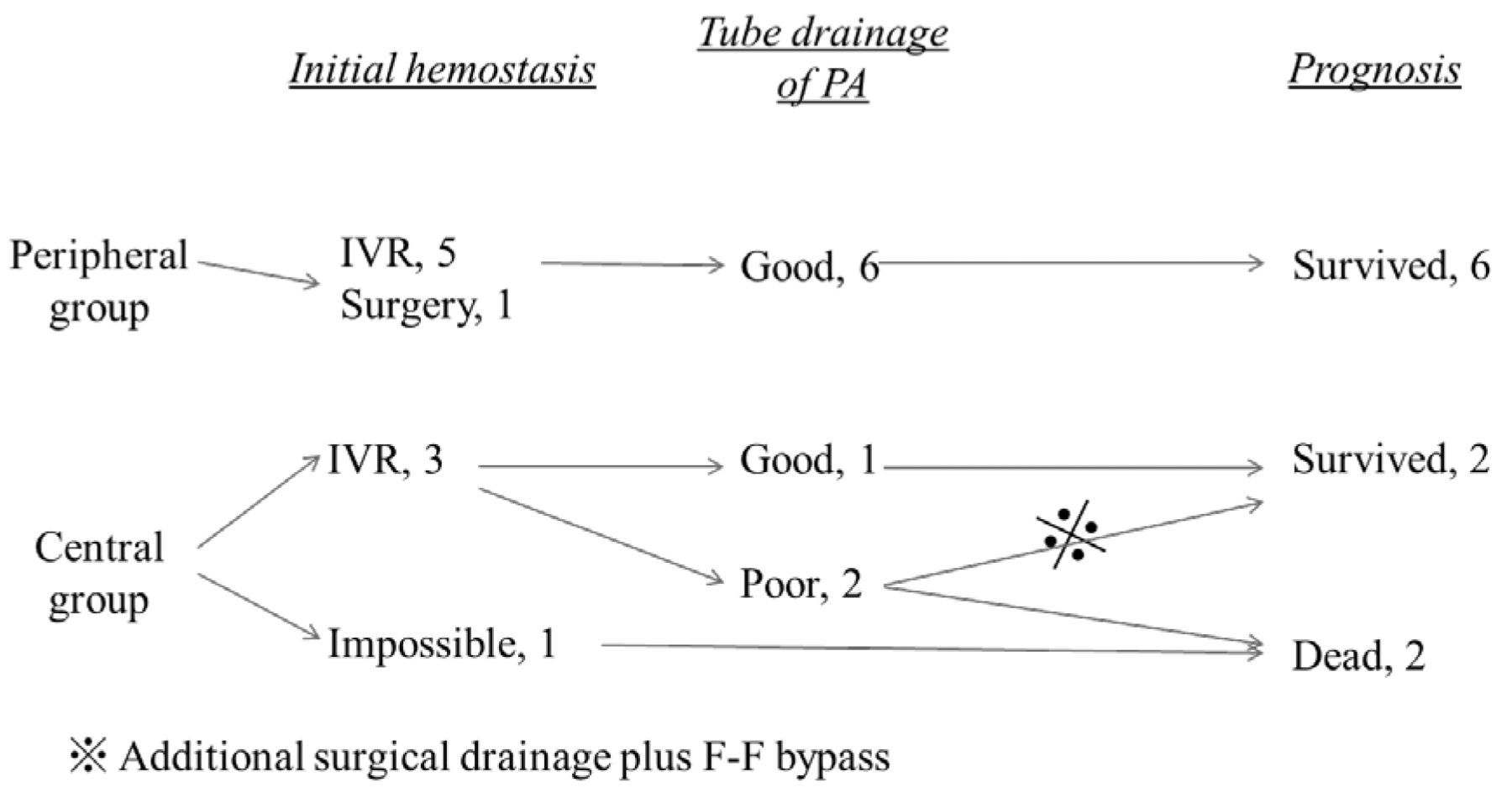
Overview of the short-term clinical outcomes and prognosis in this study.
On the other hand, the present study also showed that when massive hemorrhage after sentinel bleeding happened, a second enhanced CT scan was not necessary. An enhanced CT scan at the time of massive bleeding was performed in two out of four patients in the central group and four out of six in the peripheral group. However, CT scan was unable to pinpoint the extravasation of contrast medium. On the other hand, angiography fully identified the source of extravasation in all patients in both groups and also demonstrated the existence of ruptured pseudo-aneurysm and re-bleeding from intraoperative hemostatic sites. Thus, at the time of IPB, especially in a hemodynamically unstable state, angiography should firstly be chosen for proper diagnosis and subsequent IVR treatment. IVR should be chosen initially for hemostasis when massive hemorrhage occurs. TAE has been proven to be an efficacious and minimally-invasive alternative to open surgery in the field of pancreatobiliary surgery (29, 30). In the clinical setting, without considering the blood flow to the peripheral arteries, TAE using gel sponge, NBCA, or coiling could become first-line treatment. SG replacement has the advantage of providing continued perfusion to the end-organ. Previous reports have shown the efficiency of SG replacement for hemorrhagic pseudo-aneurysm in serious situations where the consequence of arterial occlusion may be disastrous (31-33). On the other hand, this procedure carries a serious risk due to the possibility of rupturing the artery because of its fragile vascular wall and of infection involving the stent itself, as the vessel is affected by septic conditions. To improve the post-hemorrhagic clinical course, in addition to initial hemostasis, control of PA from residual infectious hematoma is another important factor.
Previous reports have shown that radiation can induce tissue fibrosis, leading to prolonged infectious complications such as PA (34-36). Even if preoperative chemoradiation therapy is introduced, good PA control by tube drainage alone is possible in almost cases. From the results of the patients with TAE treatment in the peripheral group, tube drainage alone could be sufficient for PA control. However, in the central group with SG replacement, although in this study there was no treatment-related complication including stent occlusion, stent de-formation, or kinking and exclusion of branch vessels, if tube drainage was insufficient, re-bleeding or refractory septicemia could occur because of the fragility of insulted arteries due to PA. Consequently, the untreatable perivascular abscess at the SG replacement site was fatal. Thus, considering patients' background, including the presence of preoperative chemoradiotherapy and SG graft stenting, surgical drainage before the artery at the SG replacement site eroded should have been applied with appropriate timing in the central group with SG replacement.
In conclusion, postoperative intra-pelvic arterial hemorrhage is an uncommon but life-threatening event after extended pelvic surgery. Based on our results, we should keep in mind the necessity of urgent hemostasis and proper drainage of residual infectious hematoma which can lead to secondary arterial hemorrhage or septicemia. For urgent hemostasis, IVR may be adequate, and TAE in the peripheral group and SG replacement in those with central bleeding could become a standard treatment. To prevent secondary serious events from residual infectious hematoma, proper drainage is indispensable. In considering the patient's individual background, surgical drainage of infectious hematoma should be planned for an appropriate time in those with central bleeding treated by SG replacement for survival.
- Received March 5, 2014.
- Revision received April 4, 2014.
- Accepted April 7, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.