


Abstract
Aim: To clarify the prognostic value of predominant histological subtypes for small-sized lung adenocarcinoma. Materials and Methods: Sixty-four specimens of resected invasive lung adenocarcinoma less than 20 mm in diameter with no lymph node metastasis were studied. These specimens were microscopically classified into predominant histological subtypes (21 lepidic, 16 acinar, 24 papillary, and three solid) according to the International association for the study of lung cancer/American thoracic society/European respiratory society adenocarcinoma classification. The relationships between tumor relapse and predominant histological subtypes were statistically analyzed. In addition the relationships between several pathological factors and predominant histological subtypes were statistically assessed. Results: Kaplan-Meier relapse-free curves showed a five-year relapse-free rate of 100% in 64 patients with lepidic-predominant adenocarcinoma, compared with a rate of 73.7% (p=0.035 by log rank test) in patients with non-lepidic-predominant adenocarcinoma (papillary, acinar, and solid). The only statistically significant pathological factor between lepidic-predominant and non-lepidic-predominant histological subtypes was lymphatic vessel invasion as assessed by logistic regression analysis. Conclusion: In small-sized lung adenocarcinoma, lepidic-predominant histological subtype is the best prognostic factor, and a low incidence of lymphatic vessel invasion in the histological subtype is a key factor for an excellent prognosis.
- Prognostic factor
- small lung adenocarcinoma
- lepidic-predominant
- histological subtype
- lymphatic vessel invasion
Lung cancer is the most common malignant neoplasm in many countries. A major histological type of lung cancer is adenocarcinoma, which is frequently detected by chest tomographic scan at a time when it is still small in size. The prognosis of lung adenocarcinoma remains unsatisfactory, even with complete clinical resection at an early stage with no lymph node metastasis (1). There is a great concern to identify the pathological features that will eventually lead to survival benefit in patients with resected invasive lung adenocarcinoma.
A new classification of invasive lung adenocarcinoma was recently proposed by the International association for the study of lung cancer/American thoracic society/European respiratory society (IASLC/ATS/ERS) (2). The predominant histological subtypes in invasive adenocarcinoma are classified as follows: lepidic (formerly called bronchioloalveolar growth), acinar, papillary, micropapillary, solid with mucin production, and other variants. These predominant histological subtypes may reflect tumor aggressiveness and prognosis.
In this study, we attempted to elucidate the prognostic implication of predominant histological subtypes and pathological factors.
Materials and Methods
Seventy-one specimens of invasive lung adenocarcinoma less than 20 mm in diameter without lymph node metastases consecutively resected between 2005 and 2009 were studied. These specimens of invasive lung adenocarcinoma were surgically resected in 41 cases by lobectomy, in 10 by segmentectomy, and in 20 by partial wedge resection. We classified the 71 specimens of invasive adenocarcinoma into predominant histological subtypes according to the new IASLC/ATS/ERS lung adenocarcinoma classification (2) as follows: 21 lepidic, 16 acinar, 24 papillary, three solid with mucin production, and seven invasive mucinous adenocarcinoma (Figure 1). We retrospectively examined 64 specimens of invasive lung adenocarcinoma, excluding the seven residual specimens of invasive mucinous adenocarcinoma.
The probability of relapse-free survival by predominant histological subtype was determined by the Kaplan-Meier method. The significance of the relationships between tumor relapse and predominant histological subtypes was statistically examined by the log-rank test. In addition, the relationships between predominant histological subtypes and pathological factors, including tumor size (under 15 mm/above 15 mm), pleural invasion, lymphatic vessel invasion, blood vessel invasion, and pleural lavage cytology on thoracotomy, were statistically assessed by univariate and multivariate analyses. Univariate and multivariate analyses were respectively conducted by chi-square test and logistic regression analysis. All p-values less than 0.05 were considered significant.
Results
Tumor relapse (relapse rate) was seen in 10 patients (23.3%) with tumor of the following predominant histological subtypes: three of acinar (18.8%), six of papillary (25.0%), and one of solid (33.3%) type. None of the patients with lepidic-predominant histological subtype experienced relapse (Table I).
Kaplan-Meier survival curves showed a five-year relapse-free rate of 100% in 64 patients with lepidic-predominant compared with a rate of 73.7% in patients with non-lepidic-predominant (papillary, acinar, and solid) (Figure 2). A significant difference was found between the two relapse-free rates (p=0.035 by the log-rank test). The follow-up period in this study ranged from 10 to 92 months, with a median follow-up period of 54 months.
The statistically significant pathological factors between lepidic and non-lepidic-predominant histological subtypes assessed by univariate logistic regression analysis were lymphatic vessel invasion (p<0.001) and blood vessel invasion (p=0.023) (Table II). Multivariate logistic regression analysis showed that lymphatic vessel invasion was the only statistically significant pathological factor between the two predominant histological subtypes (p=0.013), which had a lower incidence in the lepidic-predominant histological subtype (Table III).
Discussion
A new histological classification of lung adenocarcinoma has been proposed by IASLC/ATS/ERS (2). Invasive adenocarcinoma is classified into the following predominant histological subtypes: lepidic, acinar, papillary, micropapillary, solid with mucin production, and other variants. The lepidic-predominant histological subtype is likely to be identical to type C adenocarcinoma, according to the classification of small-sized lung adenocarcinoma by Noguchi et al. (3) or bronchioloalveolar carcinoma containing invasive components. Minimally-invasive adenocarcinoma (MIA), defined as a small adenocarcinoma (≤3 cm) with a predominantly lepidic pattern and ≤5 mm invasion dimension in any one focus (2), is thought to have an excellent prognosis (4). At our Institute, the specimens of 31 patients with MIA were surgically resected by lobectomy, segmentectomy, or partial wedge resection between 2005 and 2008. No patients diagnosed with MIA had a tumor relapse after surgical resection (data not shown). Invasive adenocarcinoma with lepidic-predominant histological subtype and MIA are considered to have mild tumor aggressiveness and an excellent prognosis (4). As expected, this study also revealed a higher 5-year relapse-free rate for patients with ≤2 cm invasive adenocarcinoma with lepidic-predominant histological subtype (100%) than that for those with non-lepidic-predominant histological subtype (73.7%). The details of the 10 cases of relapse among the 43 patients with non-lepidic-predominant histological subtypes are as follows: 3 out of 16 acinar cases (18.8%), 6 out of 24 papillary cases (25.0%), and 1 out of three solid cases (33.3%). Despite the small size of this study, the results suggest that acinar, papillary, and solid predominant histological subtypes confer a poorer prognosis than the lepidic-predominant histological subtype. The findings are consistent with recent studies (4, 5), which have shown that solid-predominant histological subtype is expected to have the strongest tumor aggressiveness among small-sized invasive lung adenocarcinomas.
Summary of predominant histological subtypes and postoperative tumor relapse rate in 64 patients with small-sized lung adenocarcinomas.
We excluded seven cases of the variant histological type of invasive mucinous adenocarcinoma from this study, because this histological type showed an intrapulmonary relapsing form through bronchioloalveolar spread unlike the common relapsing form of metastasizing to intrapulmonary lesion (6). There were no cases of micropapillary-predominant histological subtype at our Institute, because the micropapillary form is usually a minor component even when present in invasive adenocarcinoma. Nonetheless, the micropapillary component was often floating on the periphery of the tumor site, despite the fact there were no micropapillary-predominant histological subtypes. We believe that the micropapillary component is one of the worse prognostic factors, since most of the 10 cases of relapse in this study had a micropapillary component floating on the periphery of the tumor site to some extent (data not shown).

Predominant histological subtypes proposed by the new lung adenocarcinoma histological classification: lepidic-predominant (a), acinar-predominant (b), papillary-predominant (c) and (d) solid-predominant with mucin production (original magnification, × 10).
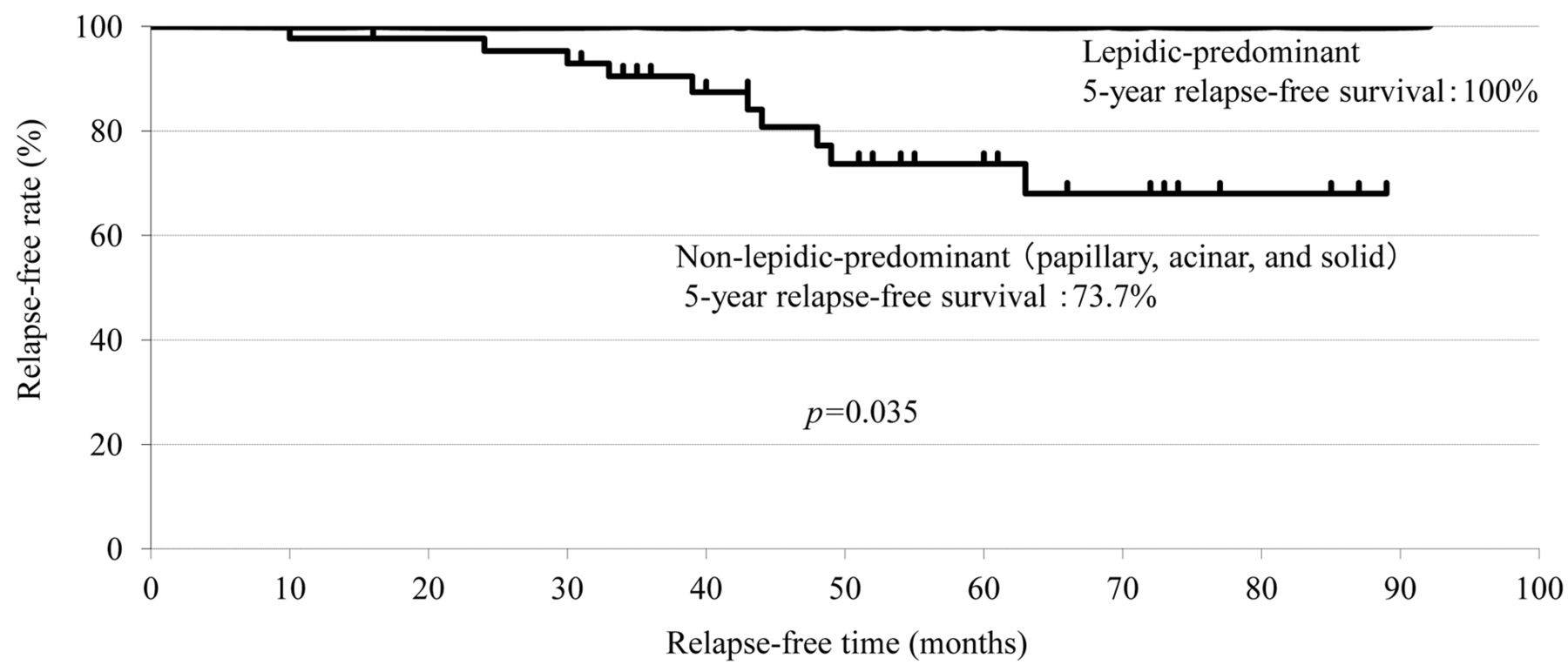
Kaplan-Meier relapse-free curves after surgery for 64 patients with lepidic and non-lepidic-predominant histological subtype small-sized invasive lung adenocarcinomas. Median follow-up time: 54 months.
Comparison of lepidic-vs. non-lepidic-predominant histological subtypes and pathological factors by univariate statistical analysis.
Lymphatic vessel invasion had a lower incidence in lepidic-predominant histological subtype than in non-lepidic-predominant histological subtypes in this study. We previously reported that lymphatic vessel invasion, not blood vessel invasion, was an independent prognostic factor in lung adenocarcinoma (7). In another study, it was also shown that lymphatic vessel invasion was an extremely useful factor in surveying the biological malignant behavior of lung adenocarcinoma (8, 9). Therefore, this study demonstrated that lymphatic vessel invasion is a very important prognostic factor associated with predominant histological subtypes in small-sized invasive lung adenocarcinoma.
Finally, we consider that the new IASLC/ATS/ERS lung adenocarcinoma histological classifications are very useful predictors of tumor relapse in small-sized invasive lung adenocarcinoma, particularly between lepidic and non-lepidic-predominant histological subtypes, and lymphatic vessel invasion is strongly associated with pathological factors reflecting differences in tumor aggressiveness between the two predominant histological subtypes.
Comparison of lepidic- vs. non-lepidic-predominant histological subtypes and pathological factors by multivariate logistic analysis.
Footnotes
-
This article is freely accessible online.
- Received February 24, 2014.
- Revision received April 29, 2014.
- Accepted April 30, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}