


Abstract
Background: Our previous study showed the prognostic impact of preoperative Glasgow prognostic score (GPS) in patients who underwent resection for non-small cell lung cancer (NSCLC). In the present study, the relationship between postoperative GPS and prognosis was also examined in patients with NSCLC with preoperative GPS 1 or 2. Patients and Methods: Three hundred and twelve consecutive patients resected for NSCLC with a follow-up period of more than five years were enrolled. The GPS was calculated as follows: patients with elevated C-reactive protein level (>1.0 mg/dl) and hypoalbuminemia (<3.5 g/dl) were assigned to GPS 2. Patients with one or no abnormal value were assigned to GPS 1 or GPS 0. Results: Study patients were allocated as follows: 264 (84.62%) to GPS 0; 31 (9.94%) to GPS 1; and 17 (5.45%) to GPS 2. The prognosis of the patients with preoperative GPS 2 was significantly poorer. Postoperative GPS was also examined for 48 patients with preoperative GPS 1 or 2. In 30/48 patients, postoperative GPS was improved to GPS 0, however, the postoperative GPS of the remaining 18 patients did not change to GPS 0. The 5-year survival of patients with postoperative GPS 0 and 1-2 were 73.02% and 11.11%, respectively. Conclusion: Preoperative GPS may be useful for postoperative prognosis of patients with NSCLC. Furthermore, persistently high GPS after surgery indicates poor prognosis in patients with NSCLC.
Although it is recognised that the development of cancer has a genetic basis, there is increasing evidence that the host inflammatory response plays an important role in the development and progression of cancer (1, 2). C-reactive protein (CRP) has been also proposed as a prognostic factor for patients with advanced non-small cell lung cancer (NSCLC) (3, 4) and to a lesser extent in those with operable disease (5, 6). In addition, hypoalbuminemia, a typical index of malnutrition, has also been reported to be associated with poor survival in NSCLC (7, 8). The Glasgow prognostic score (GPS), based on serum CRP and albumin levels, was developed to aid in the assessment of cancer prognosis (9). An elevated GPS has been shown to be associated with worse prognosis for patents with inoperable NSCLC (9, 10).
Until recently, the clinical application of GPS in patients who have undergone complete resection for NSCLC has rarely been studied. We previously studied the prognostic significance of preoperative GPS for patients with operable NSCLC, and found that it is a useful prognostic determinant (11).
In addition to GPS, our previous studies also reported the prognostic significance of serum carcinoembryonic antigen (CEA) and neutrophil-to-lymphocyte ratio (NLR) for operable NSCLC (12, 13). Furthermore, it has also been reported that patients with a persistently high CEA level or NLR after surgery for NSCLC had a poor prognosis (14, 15). As far as we know, there have been few reports concerning the influence of postoperative GPS. Therefore, in addition to preoperative GPS, we examined the postoperative GPS for patients with preoperatively high GPS.
Patients and Methods
Three hundred and twelve patients who underwent surgery for NSCLC from 2004 to 2008 at. our hospital and for whom preoperative laboratory data for CRP and albumin were available were enrolled into the present retrospective study. Patients who did not undergo complete resection, died of other diseases within five years after surgery or were lost to follow-up were excluded. For evaluation of the GPS, the results of blood tests determined as part of the routine preoperative examination were used. The GPS was calculated as previously described (9, 10). Patients with both an elevated CRP level (>1.0 mg/dl) and hypoalbuminemia (<3.5 g/dl) were allocated a score of 2. Accordingly, patients with neither of these abnormalities were allocated a score of 0. The remaining patients, in whom only one of the biochemical parameter was abnormal, were assigned a score of 1. For patients with preoperative GPS 1 or 2, the postoperative GPS was also measured at one to two months after surgery for each patient. Pathological (p) tumor-node-metastasis (TNM) staging was recorded in all patients based on the seventh edition of the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) classification (16).
Follow-up information, including cause of death, was ascertained through a review of clinic notes and direct or family contact. The chi-square test with Yates' correction was used to correlate clinicopathological parameters with the GPS. The survival curves of the patients were plotted by using the Kaplan–Meier method and analyzed using the log-rank test. The Cox regression hazard model was used for univariate and multivariate analyses to assess the prognostic value of GPS. Statistical calculations were conducted with JMP (SAS Institute Inc., Cary, NC, USA) and values of p less than 0.05 were accepted as being significant.
Results
The baseline characteristics are summarized in Table I. Study patients were allocated as follows: 264 (84.62%) to GPS 0; 31 (9.94%) to GPS 1; and 17 (5.45%) to GPS 2. Relationships between GPS and clinicopathological features are also shown in Table I. Age, gender, histology, pStage, pT status, pN status and serum CEA level showed no significant relationship with GPS classification.
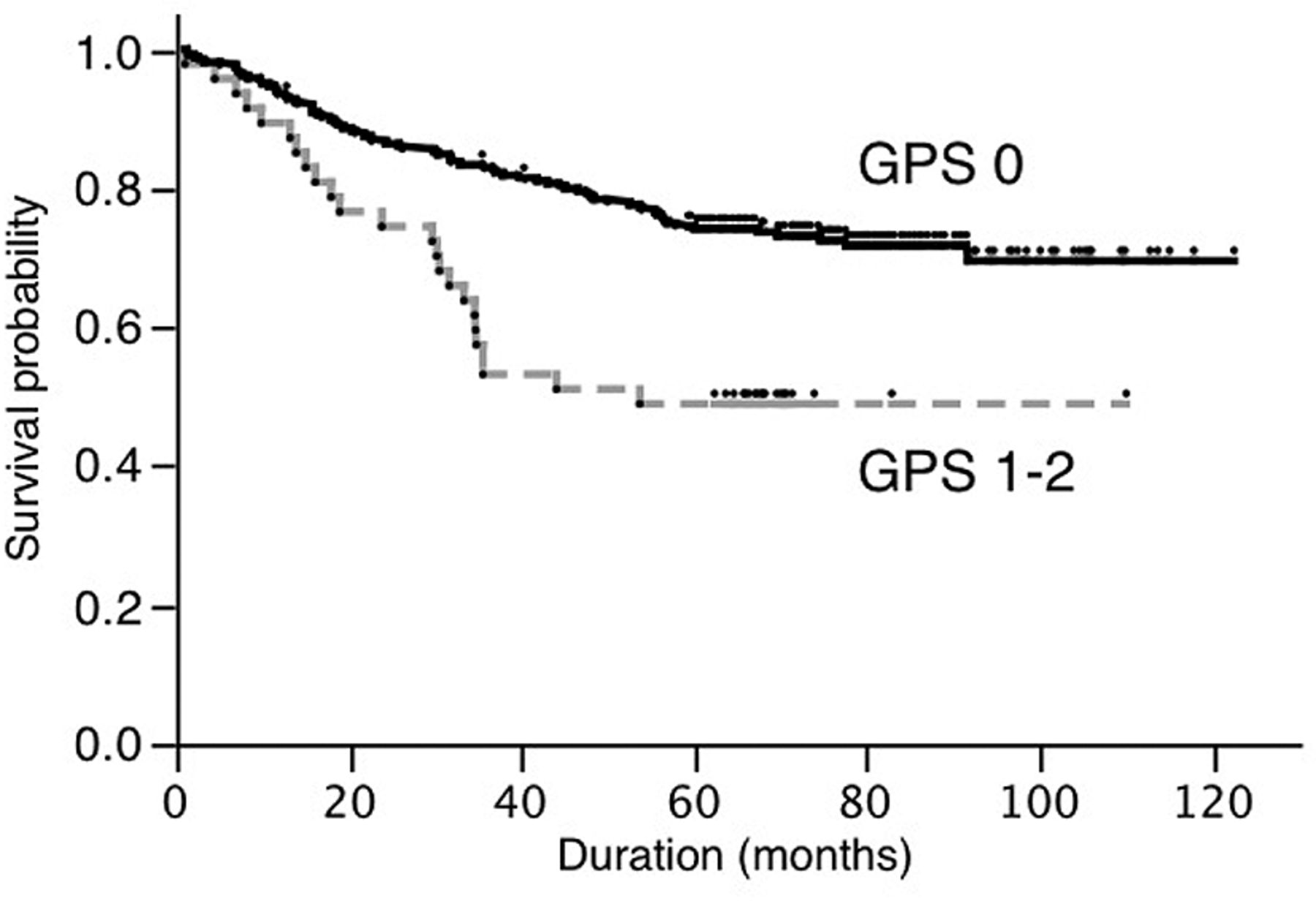
The 5-year survival rates of patients with GPS 0, GPS 1 and GPS 2 were 74.30%, 56.67%, and 31.25%, respectively. Since the number of patients with GPS 1 and 2 was small, we compared the patients with GPS 0 to those with GPS 1-2. As shown in Figure 1, the 5-year survival of the patients with GPS 1-2 was significantly poorer (p<0.0002).
Univariate Cox proportional hazard regression analysis revealed that age (<65 vs. ≥65), gender (male vs. female), histological subtype (adenocarcinoma vs. other), pT status (pT1 vs. pT2-3), pN status (pN0 vs. pN1-2), serum CEA level (normal vs. high) and GPS (GPS 0 vs. GPS 1-2) were related to better patient prognosis (Table II). The results of multivariate analysis including all variables for which p<0.05 on univariate analysis are also summarized in Table II. Of the variables that were included in the multivariate analysis, age (<65 vs. ≥65), gender (female vs. male), pT status (pT1 vs. pT2-3), pN status (pN0 vs. pN1-2), serum CEA level (normal vs. high) and GPS (GPS 0-1 vs. GPS 2) were independent predictors of survival (Table II).
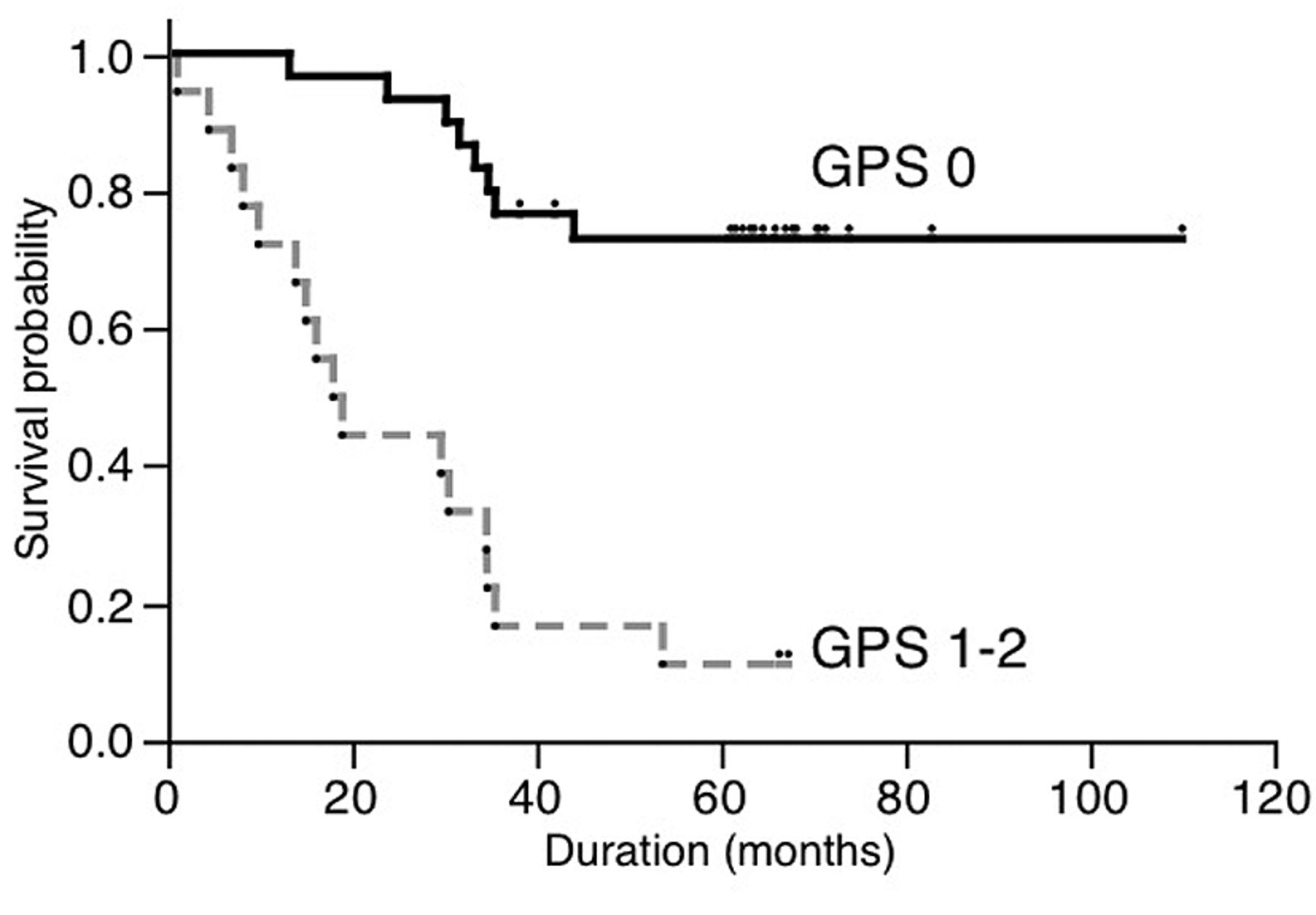
The postoperative GPS was also measured one to two months after surgery for 48 patients with preoperative GPS 1 or 2. As shown in Table III, 30 out of 48 patients with preoperative GPS 1 or 2 had postoperative GPS 0. However, postoperative GPS of other 18 patients was GPS 1 or 2. The survival curve based on postoperative survival is shown in Figure 2. The 5-year survival of the patients with postoperative GPS 1 or 2 was significantly poorer than that of those with postoperative GPS 0 (p<0.0001). Univariate and multivariate analyses for patients with preoperative GPS 1 or 2 also revealed that postoperative GPS was an independent prognostic determinant (Table IV).
Clinicopathological characteristics of study participants.
Discussion
The host inflammatory response has an important role in the development and progression of cancer (1, 2, 17, 18). Inflammation might promote secretion of CRP. A high CRP level may reflect an inflammatory response to tumor. Numerous studies have reported that elevated CRP levels are indicative of a poor outcome in NSCLC (3-6). It is now well-known that inflammatory processes almost always accompany cancer, and persistence of inflammation-like processes within cancer tissue causes suppression of antitumor immunity (17, 18). Hypo-albuminemia is often reported in patients with NSCLC and is usually regarded as a good index of malnutrition and cachexia. Serum albumin has also been described as an independent prognostic factor for survival in NSCLC (7, 8). Previous studies have indicated that hypo-albuminemia is likely to develop secondary to an increase in serum CRP level (19). Accordingly, hypoalbuminemia and a high level of CRP may be regarded as a paraneoplastic phenomenon.
The GPS, which is based on both serum elevation of CRP and hypoalbuminemia, may enable a better appreciation of the effects of tumor on both ongoing systemic inflammation and malnutrition (9, 10). The GPS has been introduced to predict prognosis of patients with very advanced NSCLC (9, 10). Although there are no previous studies on the significance of the GPS for operable NSCLC, we recently demonstrated the prognostic value of the GPS in patients with operable NSCLC (11). The present study also revealed that a preoperatively high GPS was associated with poorer survival in patients with operable NSCLC. In spite of several reports for the prognostic significance of the pre-treatment GPS (9-11), little information is available regarding the prognostic role of the postoperative GPS in patients undergoing surgical resection. In the present study, we also evaluated the prognostic role of postoperative GPS, and found that patients with NSCLC with a persistently high GPS after surgery had a poor prognosis. A high GPS might be regarded as a para-neoplastic phenomenon. If the surgical extirpation of a tumor is complete and if no residual tumor is present, there would be no cause for a high GPS. If residual tumor cells exist, the GPS value does not decrease, and its value is maintained, which represents the number of residual tumor cells. Therefore, a postoperative GPS of 1 or 2 might mean the presence of residual tumor cells in the body. In this regard, many of patients with NSCLC with preoperative GPS of 1 or 2 and postoperative GPS of 0 might have had local disease cured by surgical extirpation, whereas those with postoperative GPS 1 or 2 might have unrecognized extrapulmonary disease.

Survival of patients based on preoperative Glasgow prognostic score (GPS) (p<0.0002).

Survival of patients with preoperative Glasgow prognostic score (GPS) 1 or 2 based on the postoperative GPS (p<0.0001).
Univariate and multivariate analyses to assess the prognostic factors for overall patients.
The number of patients with GPS 1 or 2 in our series is smaller than that in previous work. The reason for this might be due to differences in stage of this patient population. That is, the present study focused on patients with operable NSCLC, whereas most previous work included many patients with advanced stage disease. Further studies with a greater number of patients are warranted.
Postoperative Glasgow prognostic score (GPS) for patients with preoperative GPS 1 or 2.
Currently, blood tests for serum albumin and CRP level are inexpensive and routine determinations. Thus GPS should be included in routine preoperative clinical assessment and treatment planning. In addition to the prognostic significance of preoperative GPS, postoperative GPS was also an important prognostic determinant for patients with preoperative GPS 1 or 2.
Limitations of our study include the relatively small study population, which was recruited at a single institution. However, our patient population is uniform, as the study cohort consisted only of patients with operable NSCLC who underwent complete resection.
Univariate and multivariate analyses for patients with preoperative Glasgow prognostic score (GPS) 1 or 2.
In conclusion, the preoperative GPS is a significant prognostic determinant for operable NSCLC. Furthermore, a persistently high GPS after surgery for NSCLC indicates a poor prognosis.
- Received February 16, 2014.
- Revision received April 16, 2014.
- Accepted April 22, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Significance of Glasgow Prognostic Scores in NSCLC Patients Treated With Immunotherapy After Platinum-based Cytotoxic Chemotherapy
- A Genitourinary Cancer-specific Scoring System for the Prediction of Survival in Patients with Bone Metastasis: A Retrospective Analysis of Prostate Cancer, Renal Cell Carcinoma, and Urothelial Carcinoma
- Systemic Immune-inflammation Index Predicts Survival of Patients After Curative Resection for Non-small Cell Lung Cancer