


Abstract
Aim: Survival of patients with stage I hepatocellular carcinoma (HCC) is higher than in patients with more advanced disease, however many of them will ultimately die of tumor recurrence and liver failure. Our objective focuses on identifying the pathological and clinical factors that could affect disease-free (DFS) and overall survival (OS). In addition we reviewed the treatment offered for recurrence and its impact on OS. Patients and Methods: Between January 1992 and December 2002, a total of 473 patients who underwent hepatectomy for HCC at the Kaohsiung Chang Gung Memorial Hospital were enrolled in this study. Relevant clinicopathological and perioperative variables were subjected to univariate and multivariate analysis. Results: A total of 224 patients with a mean follow-up period of 4.6 years were analyzed. The 1-, 3-, 5-, and 10-year DFS rates were 82.5%, 57.6%, 46.9% and 32.0% respectively. The 1-, 3-, 5-, and 10-year OS rates were 91.5%, 83.0%, 70.1% and 56.3% respectively. The multivariate analysis identified age >50 yeas, Indocyanine Green (ICG) clearance test and cirrhosis as independent factors that negatively impact DFS and age ≥50 years, resection type, presence of complications and tumor recurrence as factors affecting OS. In patients with recurrence (n=130), the factors that negatively impact OS were blood transfusion, age ≥50, blood loss and presence of surgical complications. Conclusion: Meticulous surgical technique is the key to improving the outcome of patients with stage I HCC. The presence of complications was the only modifiable clinicopathological factor that affected the OS in our study.
Hepatocellular carcinoma (HCC) is ranked as the fifth malignancy in men and the seventh in women in the world, making it one of the most lethal types of solid-organ cancer (1). The majority of HCC are hepatitis B or C virus infection-related, hence active surveillance for HCC has resulted in a growing number of patients with early HCC. These early cases have the greatest chance of curative treatment, including that with locoregional therapies, mainly radio-frequency ablation (RFA), surgical resection or transplantation. For patients with compensated cirrhosis and early-stage disease, the best treatment options are the first two of these, with surgical resection offering a disease-free survival (DFS) advantage over RFA in some studies (2). From previous studies, we have learned that the survival of patients with AJCC stage I HCC, defined as single tumor without vascular invasion (seventh edition) (3), was superior to that for other stages but many patients ultimately died of tumor recurrence and liver failure (4). There are many well-known prognostic factors (5) for HCC but very few are described in early cases and we found none for patients with AJCC stage I disease.
In the present study, we aimed to identify the pathological and clinical factors that might affect DFS and overall survival (OS) in this group of patients, searching for new modifiable factors we could improve and put into practice, in addition we reviewed the treatment and the patterns of recurrence of this selected group of patients and their impact on OS.
Patients and Methods
Between January 1992 and December 2002, a total of 473 patients underwent hepatectomy for HCC at the Kaohsiung Chang Gung Memorial Hospital, Taiwan.(6) Of these, 224 patients with pathologically-classified AJCC stage I HCCs were included in this study. All of the patients were operated when the seventh edition of the AJCC was not in use; this is why the pathological diagnosis with the former AJCC editions was revised to fit the seventh edition the AJCC definition of stage I criteria. All relevant data were taken from a prospective computer database for the cancer registry of the hospital. Perioperative and postoperative care evaluation were conducted according to established institutional criteria (6). The intraoperative management and technique in hepatectomy have already been reviewed (5). In major hepatectomy, such as right and left lobectomy, resections were usually anatomical; extended right or left lobectomies were usually non-anatomical; the majority of minor resections were non-anatomical. The mean follow-up period was 4.6 years.
Demographics of 224 patients with stage 1 hepatocellular carcinoma.
Clinicopathological variables. Major resections were defined as removal of more than three segments, whereas, minor resections consisted of removal of fewer than three segments. Cirrhosis was determined by histological examination of the adjacent non-tumorous liver. Histologically, cirrhosis was considered in specimens with fibrosis score of 5-6 using the Ishak scoring system. (7). Tumor differentiation was determined using the Edmonson-Steiner criteria (8). Complications were defined as follows. Prolonged ascites: when the ascitic fluid drainage was more than 500 cc on postoperative day 5 with adequate diuretic treatment; intra-abdominal sepsis: any culture-positive drainage with significant clinical symptoms; liver failure: validated by the 50-50 criteria (9); pulmonary complication: either pleural effusion requiring drainage or culture-proven pneumonia; cardiac complications: mostly arrhythmias necessitating pharmacological treatment; GI complications: gastrointestinal bleeding that prompted endoscopic treatment.
The time to recurrence was computed from the day of surgery to the first follow-up visit at which the recurrent tumor was detected. Patients who died of causes unrelated to HCC were considered disease-free. Survival outcome, tallied from the date of surgery to the date of death or the last follow-up, was verified using the same database and telephone interviews. Hospital deaths, which corresponded to the time when the resection was performed, were included in the overall survival.
Statistical analyses. Continuous variables are expressed as the mean with standard deviation and range values, while categorical variable are presented as frequencies and proportions. The differences between groups were assessed using X2 test for binary variables and t-test for continuous variables. The OS and DFS were estimated using Kaplan–Meier survival method and the differences were compared by log-rank test. All variables with a p-value of less than 0.10 in univariate analysis were further used for multivariate analyses using Cox's proportional hazard model. The threshold for significance was a valve of p<0.05. Statistical analysis was performed using commercially available SPSS software (SPSS, version 15.0; SPSS, Inc, Chicago, IL, USA).
Results
Demographics. A total of 224 patients with pathologically-proven stage I HCC were included in the analyses. The majority of patients were male (79%), aged more than 50 years (62%), with an AFP <400 ng/ml (79%). The mean ICG was less than 10% in 171 (76%) of the patients. A total of 127 (56%) of the patients were HBsAg-positive. Major resections were performed in 136 (60%) of the patients; 97% of the patients had blood loss <1,000 ml and only 12% required blood transfusion. Tumor recurrence occurred in 130 (58%) patients, with most [105 (80.7%)] being intra-hepatic. Postoperative complications developed in 28 (12.5%) cases. The complications consisted of prolonged ascites in 10 (35%), intraabdominal sepsis in 3 (10.7%), liver failure in 4 (14.3%), pulmonary adversities in 4 (14.3%), cardiac adversities in 2 (7.1%), gastrointestinal complications in 3 (10.7%), urinary tract infection in 1 (3.5%) and multiple organ failure due to unknown cause in 1 (3.5%). In-hospital mortality was 2.3% Three patients died of liver failure while the other 2 died of multiple organ failure due to sepsis and unknown cause (Table I).
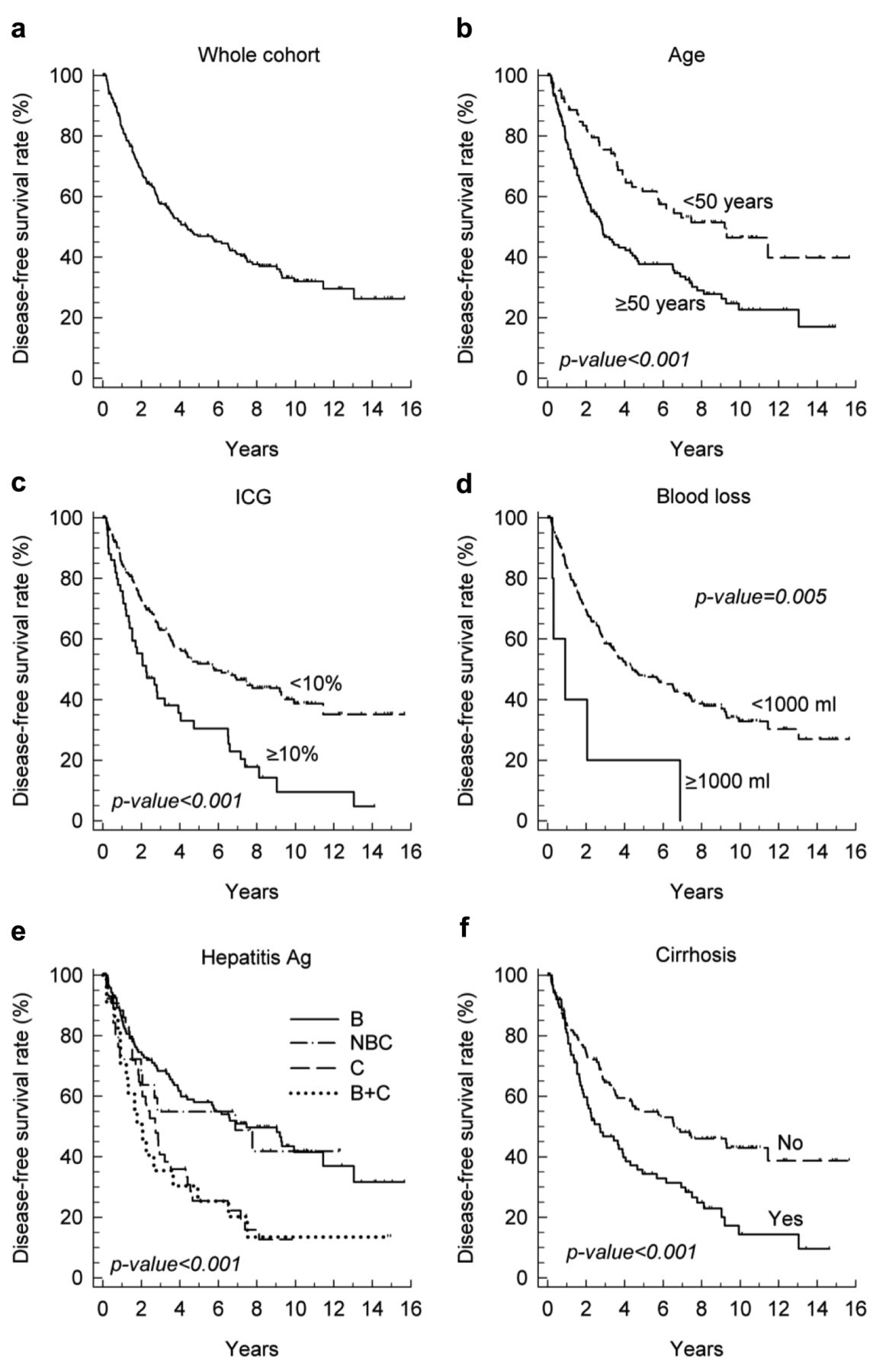
DFS. The 1-, 3-, 5-, and 10-year DFS rates were 82.5%, 57.6%, 46.9% and 32.0%, respectively (Figure 1) (Table II). In the univariate analysis, only age <50 years, ICG≤10%, HBsAg negativity, blood loss <1000 ml and lack of pathological cirrhosis increased the DFS (with p-values of <0.001 to, 0.005. After the univariate analyses, 6 out of 15 variables with p<0.10, including age, ICG, blood loss, blood transfusion, hepatitis infection status, and cirrhosis, subsequently underwent multivariate analysis. After the multivariate analysis, only three variables age <50 years, ICG ≤10% and lack of pathological cirrhosis were ultimately considered independent factors predicting better DFS (Table III).
Recurrence. The mean time in years for local and distant recurrence was 3.0 and 2.3 years, respectively. The overall rate for intrahepatic recurrence at 1, 3, 5 and 10 years was 26%, 42%, 13% and 20% and that for distant metastasis was 42%, 28%, 28% and 0% (Figure 2, TabIe I).
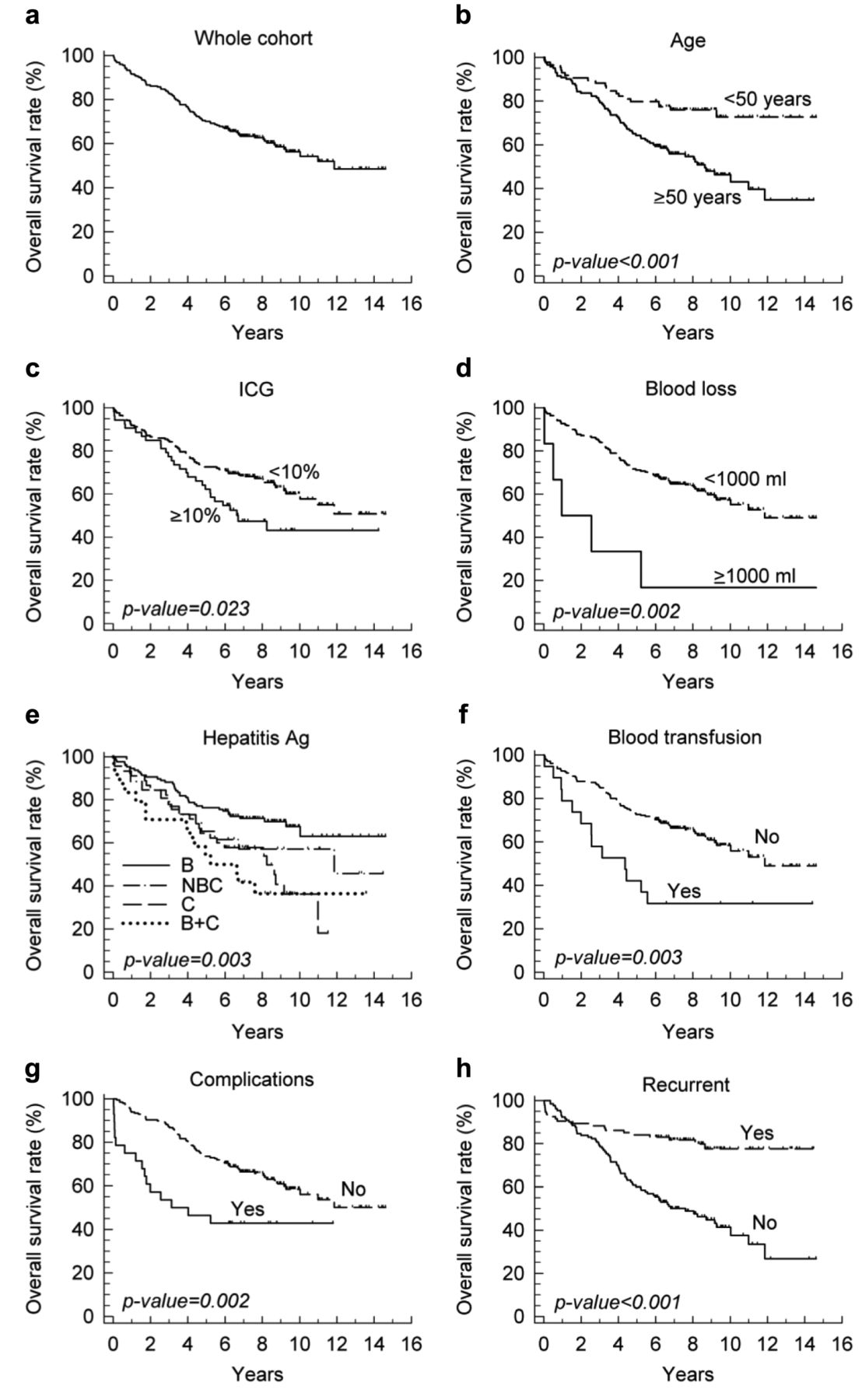
OS. The 1-, 3-, 5-, and 10-year OS rates were 91.5%, 83.0%, 70.1% and 56.3%, respectively (Figure 3), (Tables III, IV). In the univariate analysis, the most significant variables negatively affecting OS were presence of recurrence and age ≥50 years with p<0.001, followed by the presence of complications with p=0.002 and HBV infection with p=0.05. Other variables with p-values less than 0.1 were blood loss (p=0.05), type of resection (p=0.09), preoperative TAE (p=0.085), Child A (p=0.075) and ICG (p=0.05).
After the multivariate analysis, only four variables, namely age, Child's Pugh status, occurrence of complications and tumor recurrence were ultimately independent factors affecting OS. Intra-hepatic tumor recurrence is the most significant factor with a HR of 3.6 (95% CI=2.1-6.3, p<0.05).
Clinicopathological differences in patients with and without recurrence. In a comparison of OS in patients in stage I HCC with recurrence (n=130) versus patients without recurrence (n=94), the results of the univariate and multivariate analyses were the following (Table V).
In patients with recurrence, the OS at 1, 3, 5 and 10 years was 92%, 79%, 60% and 41%, compared with 90%, 88%, 84% and 77% in patients without recurrence.
In patients without recurrence, the factors that affected OS were age ≥50 years, blood loss and the most significant being the presence of complications, with a HR=5.3 (95% CI=2.0-13.9) p=0.001. The only patient that lost more than 1000 ml of blood died.
In patients with recurrence, the factors that affected OS were blood transfusion with a HR 2.2(1.2-4.3), p=0.06 and tumor differentiation HR 2 (1.1-3.5), p=0.025.
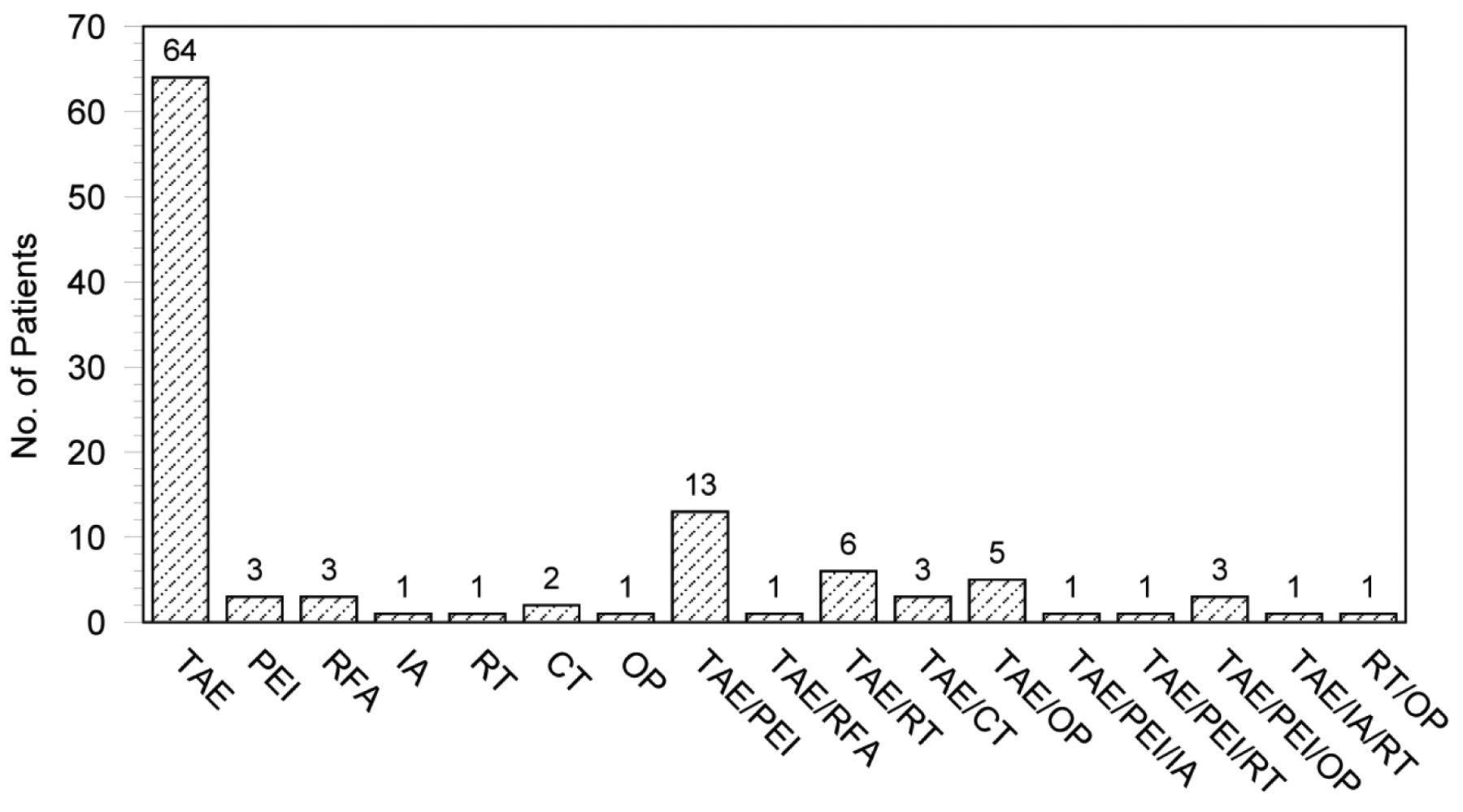
Treatment of recurrent HCC. Sixty-four (61%) patients with recurrence received TAE, 13 (12%) receiving a combination of TAE and percutaneous ethanol injection. Ten (8%) were submitted to re-resection. Three (2%) patients underwent RFA. Figure 4 showed multimodalities of treatment of recurrent HCC.
Discussion
In the seventh edition of the AJCC TNM staging, stage I HCC is distinguished as an early disease as it is represented by a single tumor in the absence of vascular invasion (10-12). The distinction of prognosis between patients with AJCC stage I HCC and more advanced HCC has been clearly illustrated in several studies (1). However, despite the superior survival, many of the patients ultimately die of tumor recurrence and liver failure within five years after resection (13). In our series, the DFS and OS at five years for patients with stage I disease were 46.9% and 70% compared to 39% and 40% for those with stage II (6).

Kaplan–Meier curves of the clinicopathological factors that affected the disease-free survival in the univariate analysis: a: AJCC stage I HCC patients; b: age <50 years; c: ICG <10%; d: blood loss <1000 ml; e: hepatitis B positive; f: Absence of cirrhosis. B: hepatitis B virus, NBC: non-B and non-C virus, C: hepatitis C virus, B+C: hepatitis B and C virus.
Univariate analysis of disease-free survival rate.

a: Recurrence rate of local, distant and local plus distant metastasis. The rate of local recurrence can be seen to climb steadily, reaching a 5-year rate of 50%. The curve of distant and local plus distant metastasis is less pronounced and remains constant at about 5% to 10% per year. b: Timing of recurrences according to type; total: 130 patients; intrahepatic: 105 patients; extrahepatic: 7 patients; both intra- and extrahepatic recurrences: 18 patients. Intrahepatic metastasis tended to occur within the first three years.
Following the multivariate analysis, only 4 variables were ultimately considered independent factors affecting the DFS and OS rates in that order. DFS was significantly inferior in older patients (≥50 years old), with worsened liver function (ICG ≥10%) and cirrhosis. The OS was also significantly reduced by old age (≥50 years old), Child B status, perioperative complications and tumor recurrences.
Of all the clinicopathological factors that affected OS, only the presence of complications was modifiable. Similarly, by carraying out a univariate and later a multivariate analysis of the factors, only blood transfusion in the patients with recurrence patients and the presence of complications and blood loss greater than 1,000 ml in the recurrence-free patients had an impact on OS. The other factors were unmodifiable, such as age, tumor recurrence, ICG and the presence of cirrhosis.
Multivariate analysis for overall and disease-free survival.

Kaplan–Meier curves of the clinicopathological factors that affect the overall survival in the univariate analysis: a: AJCC stage I HCC; b: age<50 years; c: ICG<10%; d: blood loss <1,000 ml; e: hepatitis B-positive; f: blood transfusion; g: presence of complications; h: tumor recurrence.
Univariate analysis of overall survival rate by Kaplan-Meier method.
Multivariate analysis of overall survival rate by Cox regression for patients with recurrence (n=130) of hepatocellular carcinoma and recurrence-free (n=94).
The role of cirrhosis in predicting survival of patients with tumors has been demonstrated in several series and was emphasized in the AJCC staging (10-14). Once established, this pathology poses the risk of developing tumor recurrences as a result of multiple carcinogenesis within the diseased liver (14, 15); and its progression can lead to the deterioration of liver function and subsequent liver failure (15). Many authors agreed that since tumor recurrences in a cirrhotic liver emanate from multicentric carcinogenesis and occur at sites distant from the original mass, huge hepatic resections should not be performed in patients with cirrhosis to avert the risk of liver failure, in particular in patients with limited liver function (16). Likewise, several studies have demonstrated that treating such tumors locally, by means of hepatic resection, TAE and RFA, would not halt the progression of the disease. Given these reasons, it is therefore sensible to conclude that the extent of tumor resection, as well as resection margins, would not positively impact patient survival (17).
Interestingly, similar to the current AJCC staging, our findings revealed that sizable tumors (>5 cm) in the absence of tumor thrombosis has no significant effect on the patients' prognosis.
Vascular invasion represents one of the most important risk factors for developing recurrence after complete resection, this might explain the differences in outcome between patients with stage I and those with stage II disease, but even taking this factor out of the analysis, we still had a local recurrence rate of 50% at five years. Hence there must be other important factors that lead to such a high recurrence rate.
The presence of complications has already been shown to be an independent predictor of poor OS in patients with HCC (18), the cause of this is not well-understood but it is hypothesized that complications lead to a state of immunosuppression which might aid in the proliferation of cancer cells (19). The rate of complications after hepatic surgery has been reported to be around 10-20% (19) up to 40%;8 our rate of complications for AJCC stage I HCC is 12.5% (Table I) and although relatively low, it was shown in our multivariate analysis to influence the OS, with an HR of 2.3 (Table II). Ascites complicates 5% to 56% of liver resections (20) cirrhosis and portal hypertension with low platelet count; intraoperative bleeding and major resections are well-known risk factors. Even hepatitis C status carries a significant risk (20). Cirrhosis was present in 41% of our patients, and 90% of our patients had some form of hepatitis and major hepatic resections comprised 60% of our series; this might explain why it was our most common complication. Blood loss in major hepatectomies has diminished through innovative surgical instruments and techniques, including minimally invasive surgery, fast track surgery, and liver-preserving surgery, among others (21-23). On the contrary, not so many advances have been made in the treatment of established liver failure, although we are better now in recognizing and predicting it early in the postoperative period, there is no solid proof that the current prophylactic interventions have diminished its occurrence, (19, 24) and once established, the only curative treatment is liver transplant. Even though all the patients had stage I disease, most of them (60%) were subject to major resections, which consequently carries a greater risk of complications. This can partly be explained by the tumor size, which in 60% was greater than 3 cm and in 30% greater than 5 cm. In addition, there is the fact that at that time, we preferred major anatomical resection to ensure adequate resection margins. This issue continues to highlight the importance of good surgical technique, in order to diminish the occurrence of complications and achieve better outcomes. The in-hospital mortality in the current series was 2.3%, which is in accordance with matched related historical series, (25) and continues to be an accepted result in current literature (26).

Types of treatment for recurrent HCC.
The treatment-of-choice for recurrence is re-resection when the functional liver remnant and the Child score allows it, followed by locoregional therapies. With this type of therapy, we have achieved a 5-year OS for patients with stage I disease of 60%. In the time period the study took place, the most accepted locoregional therapy was TAE; RFA was just starting to gain acceptance. The advantage with TAE is that it can be repeated as the recurrences appear, extending the OS. RFA is gaining more and more evidence as a curative treatment of HCC, especially in stage I disease (early, very early stage) (27). Its place in the management of recurrences is now well established (28, 29).
Recurrences that appear in the first two years after surgery are said to be due to re-growth of remaining microscopic intrahepatic metastatic foci and those that appear after two years are said to be due to multicentric carcinogenesis (30). Our series show that most intrahepatic recurrences present during the first three years (Figure 2).
Patients with stage I disease tend to have better DFS rates than patients with disease in other stages This in fact is the basis for offering salvage transplantation to patients with unfavorable histology and vascular invasion (31, 32). Our pattern clearly shows that the intra-hepatic and extra-hepatic recurrences tend to appear early, even in patients with stage I disease.
It is evident from our analyses that despite the current advances in the treatment of HCC, controlling the rate of tumor recurrence and eventual death following resection remains an urgent task. Our current strategy has provided acceptable OS (70% at five years) and an in-hospital mortality of 2.3% in stage I HCC. Considering our findings, we believe that death from HCC can be reduced through the following approach: proper patient selection and adequate preoperative planning, intensive perioperative care and meticulous dissection to prevent perioperative complications, including bleeding, and in doing so, diminishing the chance of necessitating blood transfusion. Regarding these last recommendations, we strongly emphasize these since they are the only modifiable factors that our analysis showed to have a real impact on the OS in stage I HCC.
Conclusion
In patients with stage I HCC, the DFS is affected by innate patient factors: age, liver function and cirrhosis. The OS is mostly affected by age but also by operative factors and tumor recurrence. In patients without recurrence, perioperative factors and age play a major role in survival, whereas in patients with recurrence, blood loss is major issue.
Meticulous surgical technique and dedicated postoperative care are the keys to improving the outcome of patients with stage I HCC. The presence of complications was the only modifiable clinicopathological factor that affected OS in our study.
Footnotes
-
↵* These Authors contributed equally in the preparation of this article.
-
Conflicts of Interest
None of the Authors have any conflicts to declare.
- Received January 16, 2014.
- Revision received April 10, 2014.
- Accepted April 11, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.