


Abstract
Gastric serrated adenoma is an apparently rare adenoma phenotype characterized by branched villi exhibiting lateral saw-tooth indentations lined with dysplastic cells. Out of the 21 gastric serrated adenomas now in record, including the case reported here, 76% (n=16) exhibited invasive carcinoma. In contrast, only 15% of the gastric tubular/villous (that is, non-serrated) adenomas reported in the literature revealed invasive growth. Although the cause for the virulent behaviour of gastric serrated adenomas remains elusive, it would appear that not only the degree of severity of the cellular dysplasia but also the serrated ornamental configurations might play a particular role in the unusual virulence of these adenomas.
Despite declining gastric cancer incidence in past decades, the absolute incidence of gastric cancer has continued to increase because of worldwide increasing age (1).
There is much discussion regarding the histological lesions that precede invasive carcinoma. It has been claimed that gastric carcinoma of intestinal type develops through a multi-step process initiated by Helicobacter pylori-induced chronic gastritis, leading to mucosal atrophy, intestinal metaplasia, dysplasia and ultimately, invasive carcinoma (2). However, African countries with a high incidence of H. pylori infection have a low-rate of gastric cancer, a phenomenon referred to as “The African enigma” (3, 4). In addition, the histological neoplastic transformation of intestinal metaplasia into dysplasia has not been convincingly demonstrated (5). Moreover, no histological precursors to gastric carcinoma of diffuse phenotype (accounting for 30%-40% of all gastric carcinomas) have been found.
Gastric cancer is more common in populations dwelling in the Pacific basin than in the Atlantic basin (6). Moreover, antro-pyloric cancer is more common in Asia and in Eastern Europe, while cancer of the proximal stomach dominates in North America and in Northern Europe. The different cancer frequency in disparate geographical regions and the various cancer locations within the stomach in different populations substantiate the notion that gastric carcinoma is induced by (unknown) environmental or lifestyle factors (1, 6).
On the other hand, progression from gastric adenomas to gastric carcinoma has been well-documented in the literature; it is referred to as “the gastric adenoma–carcinoma pathway” (7). In Western countries, gastric polyps are detected in 1-4% of patients undergoing gastric biopsies (8). Several histological classifications of gastric adenoma have been proposed (9-13).
In 2001, we reported a novel histological phenotype of gastric adenoma characterized by branched villi having lateral saw-tooth indentations (14). The serrated elongations were lined with stratified dysplastic cells with eosinophilic cytoplasm. This novel phenotype was called gastric serrated adenoma, as it mimicked serrated adenomas in other organs of the gastrointestinal tract, such as the colon (15), appendix (16), duodenum (17), pancreas duct (18), and esophagus (19). Importantly, serrated adenomas were not listed in any of the aforementioned classifications of gastric polyps (9-13), nor in any of the large series of gastric adenomas in the literature (8, 20, 21). One possible explanation for this conundrum could be that gastric serrated adenomas were classified together with gastric villous adenomas. Another possible explanation could be that this histological phenotype is rare in the stomach. However, several cases of gastric serrated adenomas were recently reported from disparate geographical regions such as Sweden (22-24), Tunisia (25), Turkey (26), Japan (27), and Korea (28).
The aim of the present study was to report an additional case of gastric serrated adenoma and to review the literature on this adenoma phenotype, particular attention being paid to the occurrence of invasive carcinoma.
Case Report
This case was sent from another Hospital to this Department for consultation. The patient was a 77-year-old female, complaining of nausea, anorexia and weight loss for the previous three months. A gastroscopy showed a non-ulcerated polyp in the proximal corpus. Endoscopic biopsies disclosed a serrated adenoma with high-grade dysplasia. The patient was subsequently operated upon, and a 10 cm-long gastric resection was performed. Gross examination of the resected specimen showed a 17 mm sessile polyp. Histology revealed serrated indentations (Figure 1) lined by intraepithelial carcinoma (carcinoma in situ), characterized by pseudo-stratified layers of pleomorphic cells with hypochromatic vesicular nuclei carrying at least one enlarged conspicuous nucleolus (Figure 2). Invasive carcinoma was present (Figure 3). Notably, no high-grade dysplasia, characterized by nuclear pseudo-stratification with enlarged hyperchromatic nuclei and loss of nuclear polarity extending beyond the middle aspect of the cellular lining, (29, 30) was found.
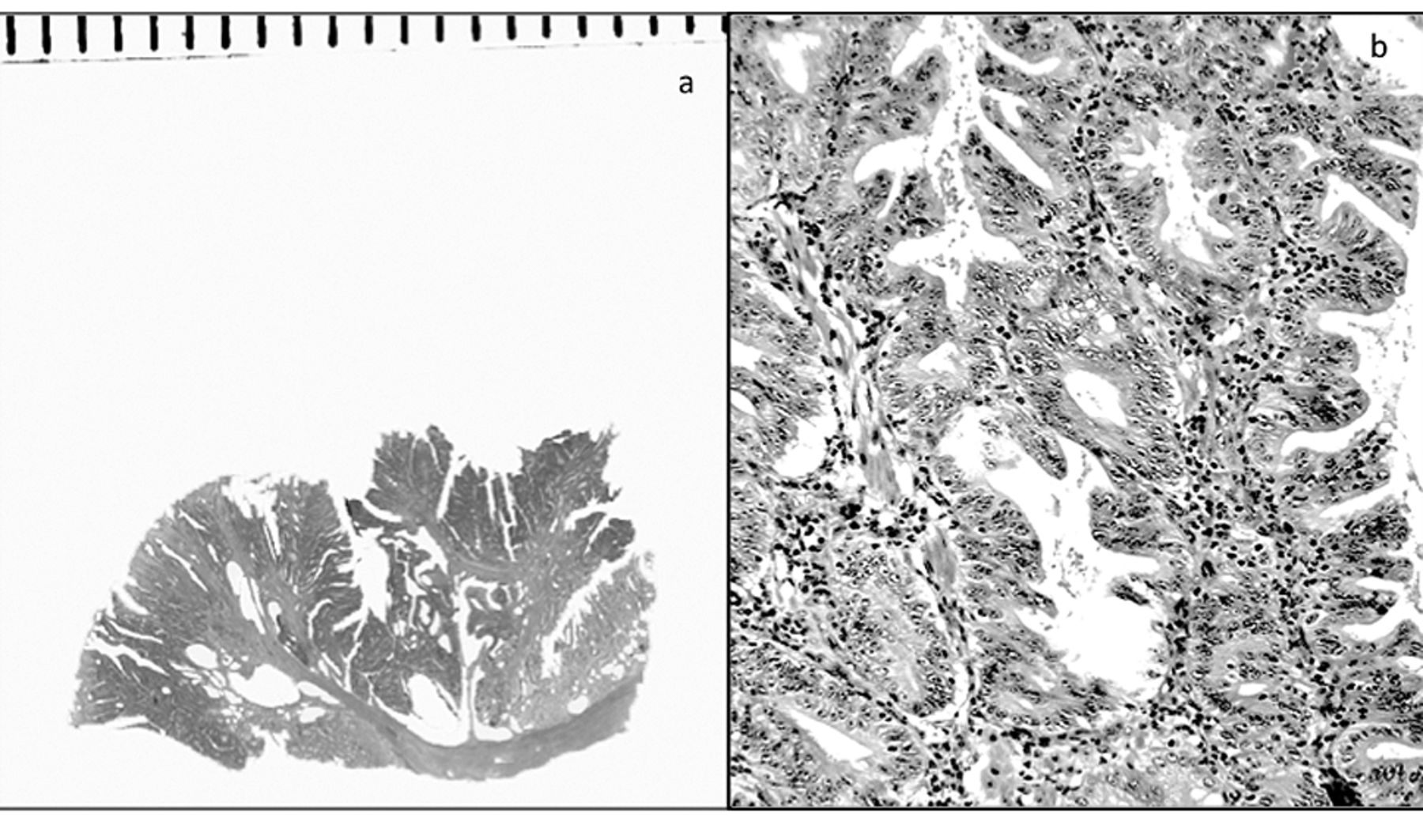
a: Low-power view of a section from the reported adenoma showing a serrated profile (H&E, ×1). b: Higher magnification to demonstrate serrated configurations (H&E, ×10).
Discussion
Several authors have reported the frequency of invasive carcinoma in gastric adenomas: Abraham et al. found invasive carcinoma in 15% of 61 gastric tubular/villous adenomas (31), Park et al. in 15% of 26 gastric tubular/villous adenomas (32), and Rubio and Kato in 18% of 17 gastric tubular/villous adenomas (33). On the other hand, 76% out of 21 gastric serrated adenomas reported in the literature, including the present case, had invasive carcinoma.
There is a plethora of literature concerning the accumulation of cellular mutations that take place during carcinogenesis, but the molecular mechanisms that generate morphological ornamental elements in the crypts of adenomas [e.g. tubular, villous, serrated or microtubular (34)], remain poorly-investigated. In this context, it has been found that morphogenesis is controlled by the interaction between the Sonic hedgehog and bone morphogenetic protein-2 (35, 36). It seems that the accumulation of cellular mutations leading to invasive carcinoma (that is, carcinogenesis) might act independently of the molecular signals that orchestrate different structural configurations in dysplastic crypts (that is, morphogenesis).

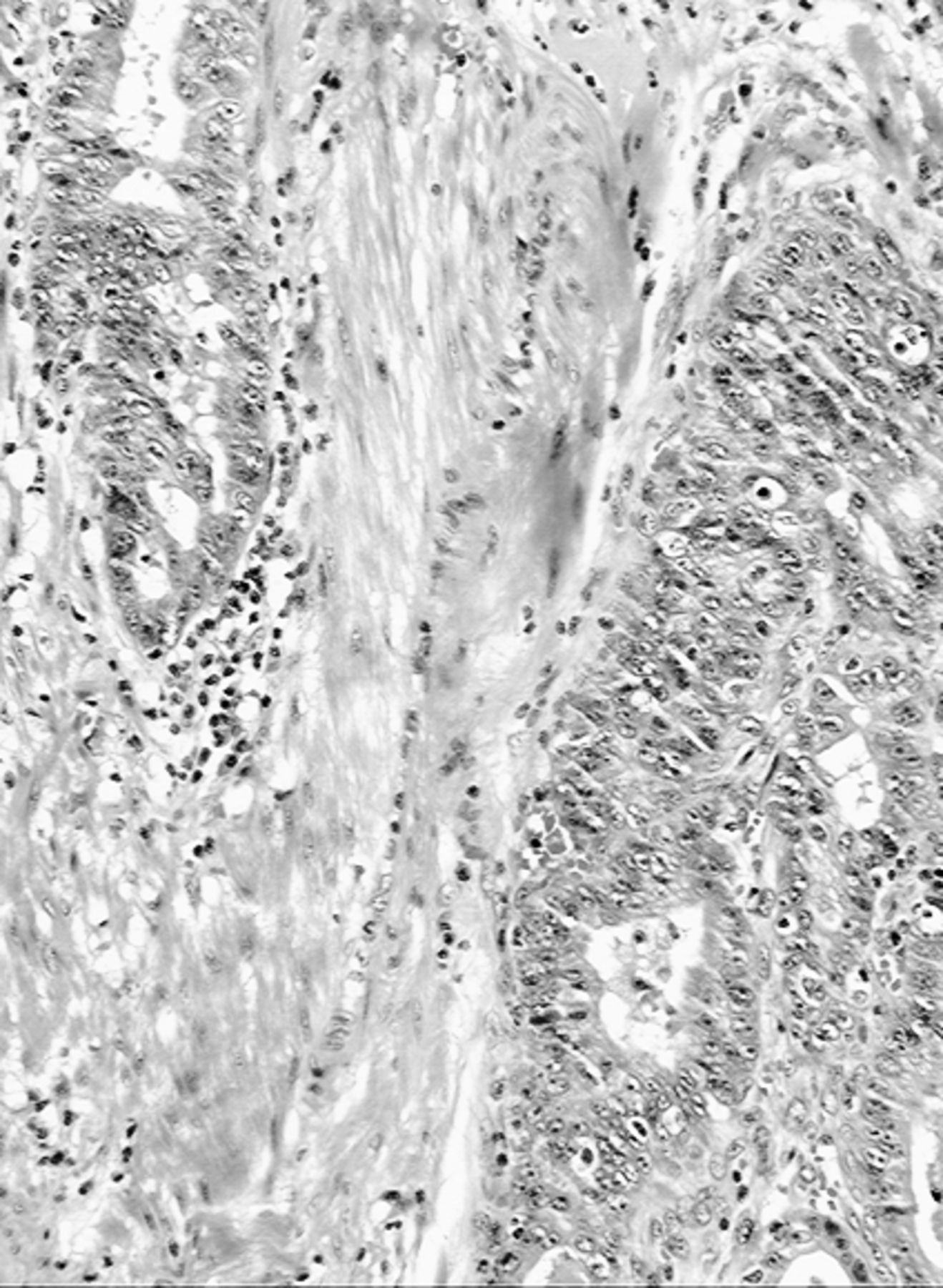
High-power view of the adenomatous component, showing serrated glands with indentations lined with intraepithelial carcinoma (carcinoma in situ), characterized by pseudo-stratified layers of pleomorphic cells with hypochromatic vesicular nuclei carrying at least one enlarged conspicuous nucleolus (H&E, ×40).

Invasive carcinoma arising in the serrated adenoma (H&E, ×10).
The cases of gastric serrated adenoma so far reported showed a particular propensity to progress to invasive carcinoma. Although the cause(s) for this behaviour remains elusive, it would appear that not only the severity of the cellular dysplasia but also the serrated ornamental configurations might play a particular role in the unusual virulence of these adenomas. This assumption is not surprising, considering that the presence of villous ornamental configurations in colorectal adenomas increases the risk to develop invasive carcinoma (29). It should be stressed that villous ornamental configurations are not present in the normal colorectal mucosa.
Paradoxically, 86% (18/21) of the cases of gastric serrated adenoma now in record, have been reported from two Institutions located in disparate geographical regions (14, 24-28). Increased awareness of the existence of this aggressive gastric adenoma phenotype may result in more cases being reported from other Institutions in the future. The molecular signals that elicit serrated ornamental configurations in gastric adenomas are being explored at this laboratory.
- Received February 26, 2014.
- Revision received May 2, 2014.
- Accepted May 5, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}