


Abstract
Prostaglandin D2 (PGD2) has been demonstrated to have antitumor effects on cancer cells. PGD2 acts through two major receptors of DP1 and DP2, as well as through the peroxisome proliferator-activated receptor γ (PPARγ) via the PGD2 metabolite, 15-deoxy-Δ12-14-PGJ2. The expression levels of DP1, DP2, and PPARγ were analyzed by immunohistochemistry on 277 primary gastric carcinomas. Either DP1- or DP2-positive cases were regarded as DP-positive. DP-Positive tumour was significantly associated with lymph mode metastasis, lymphatic invasion, and venous invasion. PPARγ positivity was not associated with any clinicopathological factors of gastric cancer. DP-Negative and PPARγ-positive cases were significantly associated with T category, lymph metastasis, and lymphatic invasion. The prognosis of DP-negative and PPARγ-positive cases was better than that of the other cases. These findings suggest that DP and PPARγ signaling influence the invasiveness of cancer cells. DP and PPARγ can be used as a potential marker for gastric cancer progression.
Prostaglandins (PGs) are products from arachidonic acid that are synthesized by cyclooxygenases. Although PGE2 is closely associated with the proliferation of various types of cancers (1-3), PGD2 is also another major metabolite of arachidonic acid associated with the progression of cancer cells. Previous studies reported that PGD2 inhibited cancer cell proliferation (4-8), including of gastric cancer cells (9). However, there are few reports on the clinical significance of PGD2 receptors in cancer.
PGD2 signaling is mediated through two distinct receptor pathways; one is the type D prostanoid receptor 1 (DP1), the G protein-coupled receptor, or PGD2 receptor; and the other is the PGD2 receptor 2 (DP2), that via chemoattractant receptor-homologous molecule expressed on type 2 helper T (Th2) cells (CRTH2) (10-12). Recent studies have reported that the PGD2 metabolite, 15-deoxy-12,14-PGJ2 (15d-PGJ2), activates the peroxisome proliferator-activated receptor γ (PPARγ) which has antitumor effects on various types of cancer (6, 7, 13-18), including gastric cancer (19, 20). However, there is no report on the correlation between DP expression PPARγ and expression. It is uncertain which receptors, DP or PPARγ, are associated with PGD2 signaling for cancer suppression (21). In the present study, we examined DP and PPARγ expression, and evaluated the relationship between the expression of PGD2 receptors and clinicopathological factors in gastric cancer.
Materials and Methods
Clinical material. Human gastric cancer tissues were obtained from a total of 277 patients who had undergone resection of primary gastric cancer at our institution between 2000 and 2004. The pathological diagnoses and classifications were made according to the Japanese Gastric cancer Association (22). Table I shows the clinicopathological characteristics of 277 patients with gastric cancer. The median follow-up time for all 277 patients was 47.7 months (range=1 to 90 months). The median follow-up time for the patients who died of their disease was 20.5 months compared with 60.2 months for surviving patients. This study was approved by the Osaka City University Ethics Committee (approval number 924). Informed consent was obtained from all patients.
Immunohistochemical techniques. Immunohistochemical staining was performed on 4-μm sections of formalin-fixed paraffin-embedded tissue. The slides were de-paraffinized in xylene and hydrated in decreasing concentration of ethyl alcohol. The sections were heated for 10 min at 105°C by autoclave in Target Retrieval Solution (DAKO, Carpinteria, CA, USA). Then sections were incubated with 3% hydrogen peroxide to block endogenous peroxidase activity. Immunohistochemistry was then carried using the following antibodies to: DP1(GTX71571, 1:100; Gene Tex, Irvine, CA, USA), DP2 (sc-271898; 1:100; Santa Cruz Biotechnology, Dallas, TX, USA), and PPARγ (ab19481, 1:50; Abcam, Cambridge, UK). The specimens were incubated with the antibody at 4°C overnight. The sections were then incubated with an appropriate immunoglobulin G for 10 min, followed by three washes with phosphate-buffered saline (PBS). The slides were treated with streptavidin-peroxidase reagent, and were incubated in PBS with diaminobenzidine and 1% hydrogen peroxide (vol/vol), followed by counterstaining with Mayer's hematoxylin.
Clinicopathological characteristics of 277 patients with gastric cancer.
Immunohistochemical scoring of DP1, DP2, and PPARγ. A numerical scoring system with two categories was used to assess the intensity and the extent of immunoreactivity. DP1 and DP2 staining were found to be cytoplasmic or membranous. For PPARγ, nucleus and cytoplasmic were both dyed. We used a proportion score as an estimate of the proportion of positive cells on the entire slide divided into five categories: 0, no immunoreactive cells; 1, immunoreactive cells <30%; 2, 30% ≤immunoreactive cells <50%; 3, 50% ≤immunoreactive cells <80%; 4, 80% ≤immunoreactive cells). The intensity score estimates the average staining intensity of positive tumor cells: 0, no staining; 1, weak staining; 2, moderate; and 3, strong membranous staining. The two scores were multiplied together to give a final numerical score ranging from 0 to 12. The cases were considered positive if the score was 6 or more. The slides were interpreted by two investigators without knowledge of corresponding clinicopathological data.
Statistical analysis. We used the χ2 test, and Fisher's exact test to determine the significance of the difference between the covariates. Survival curves were constructed using Kaplan–Meier method and compared using the log-rank test. The influence of each prognostic factor on patient survival was evaluated using Cox regression analysis. A p-value less than 0.05 was considered as the limit of statistical significance. All analyses were performed by SPSS software program (SPSS Japan, Tokyo, Japan)
Results
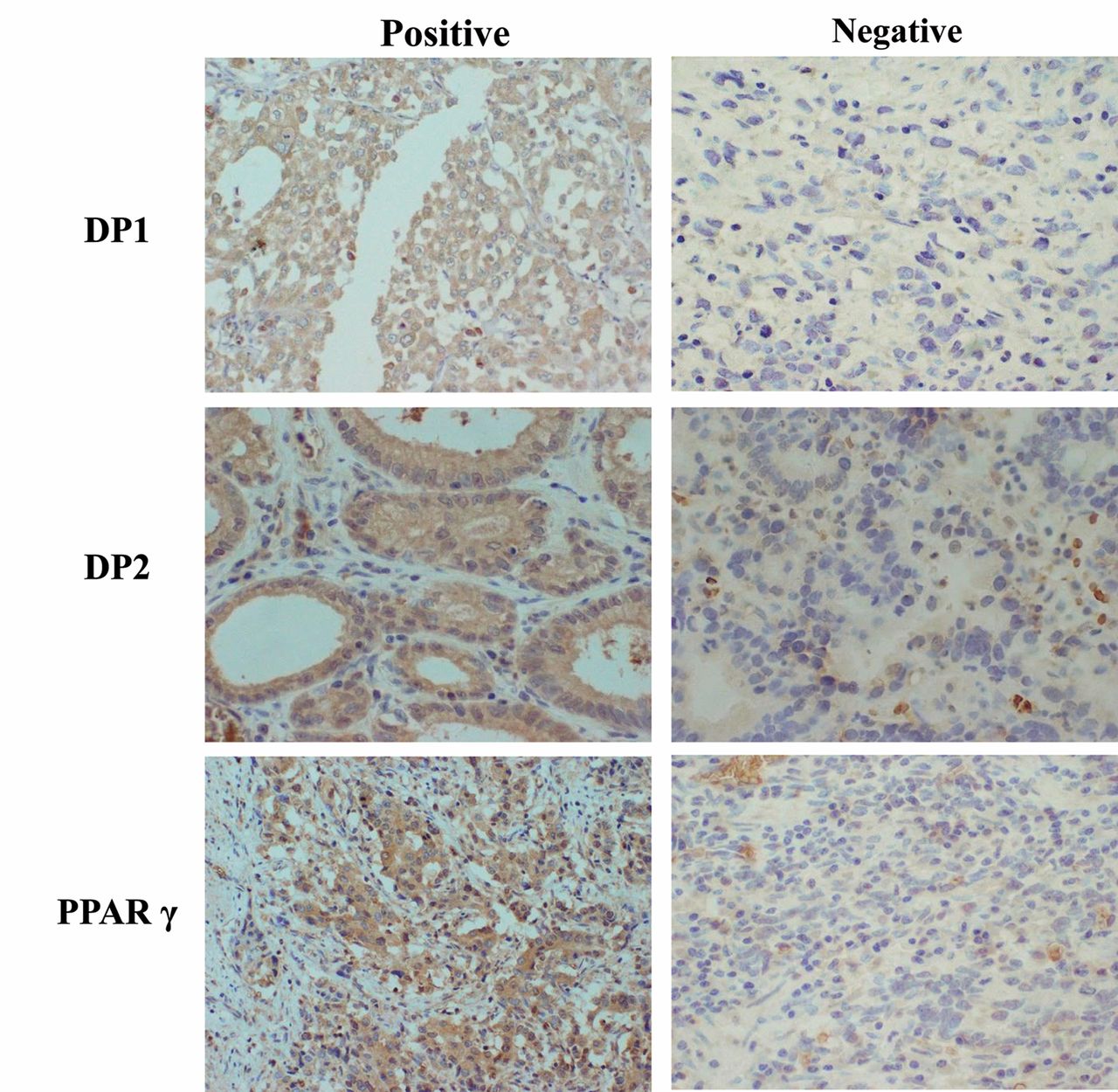
Expression of DP1 and DP2 in gastric cancer. DP1 and DP2 were immunolocalized to the cell membrane and the cytoplasm (Figure 1). Table II shows the relationship between DP1, and DP2 expression and the clinicopathological features of gastric cancer. DP1 expression was positive in 105 (38%) out of 277 gastric tumors. DP1 expression was significantly positively correlated with T stage with respect to depth of tumor invasion (p=0.026), lymph node metastasis (p<0.001), lymphatic invasion (p=0.012), venous invasion (p=0.011), and Tumor infiltrative pattern (INF) type c (p=0.024). No statistically significant association between DP1 expression and patient gender, age, hepatic metastasis, or peritoneal metastasis was observed. DP2 expression was positive in 46 (17%) out of 277 gastric tumors. No significant association was observed between DP2 expression and any clinicopathological features. Furthermore, we defined either DP1-positive or DP2-positive cases as DP-positive cases, and both DP1-negative and DP2-negative cases were defined as DP-negative cases. A significantly positive correlation was observed between DP expression and T stage with respect to the depth of tumor invasion (p=0.029) lymph node metastasis (p<0.001), lymphatic invasion (p=0.028), and venous invasion (p=0.033).
Expression of PPARγ and DP in gastric cancer. PPARγ was immunolocalized in the cytoplasm and nuclei (Figure 1). PPARγ expression was positive in 152 (55%) out of 277 gastric tumors. Table III shows the relationship between PPARγ and the clinicopathological features of gastric cancer. PPARγ positivity was not associated with any of the clinicopathological factors. DP-negative and PPARγ-positive expression was observed in 70 (25%) out of 277 gastric tumors. A significantly negative correlation was observed of DP-negative and PPARγ-positive expression with T stage with respect to depth of tumor invasion (p=0.038), lymph node metastasis (p=0.012), and lymphatic invasion (p=0.050).
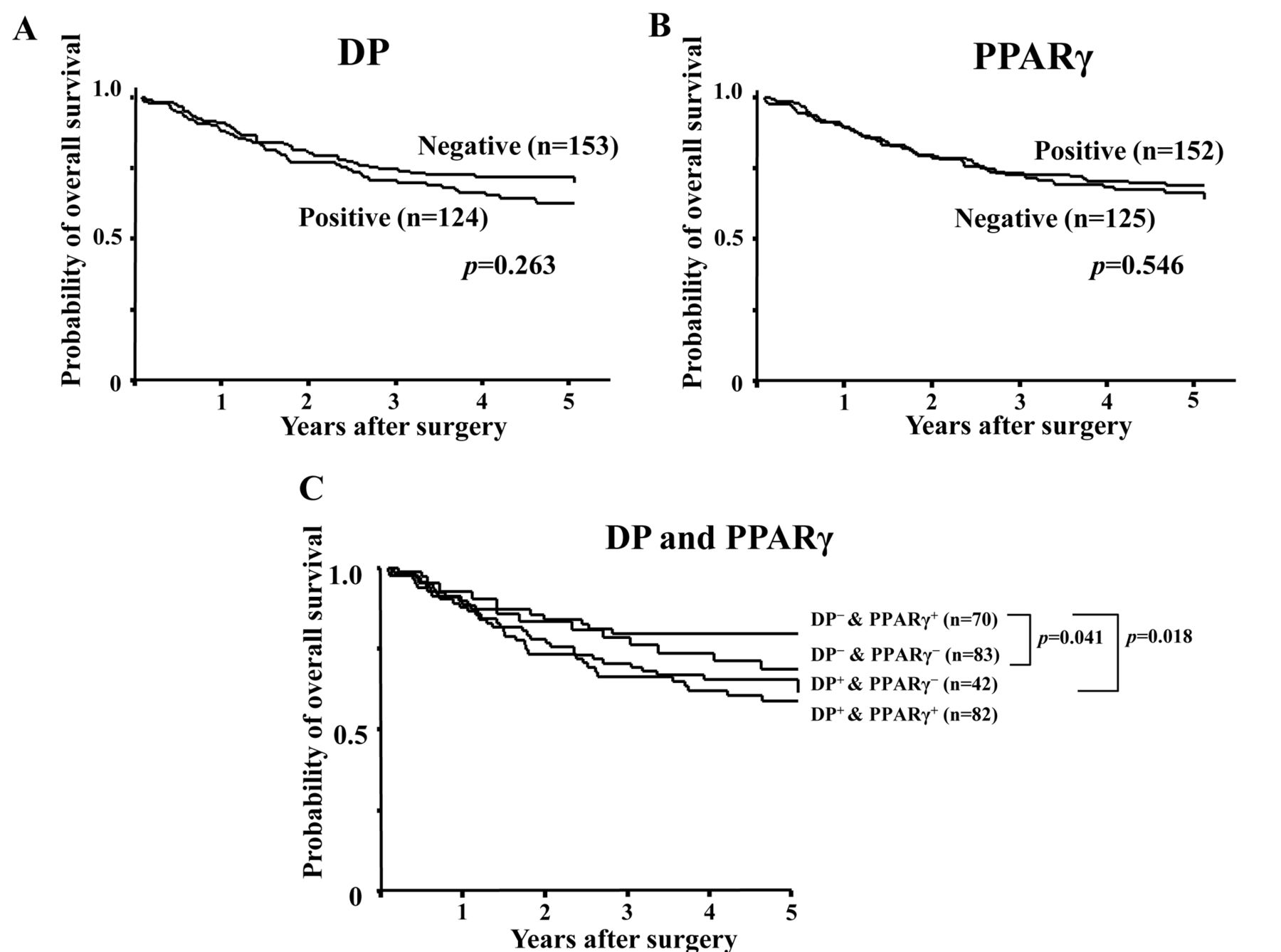
Patient survival. No significant correlations were observed between DP and PPARγ levels and patient survival (Figure 2A and B). In contrast, the prognosis of patients with DP-negative and PPARγ-positive tumors was better than that of those of the other groups (Figure 2C). In univariate analysis, DP-negativity and PPARγ-positivity (p=0.027), macroscopic type not type 4 (p<0.001), intestinal tumor histology (p=0.018), T stage I/II (p<0.001), no hepatic metastasis (p<0.001), no peritoneal metastasis (p<0.001), no lymph node metastasis (p<0.001), no lymphatic invasion (p<0.001), and no venous invasion (p<0.001) were significantly associated with better patient survival. In multivariate analysis, macroscopic type, not type 4 (p<0.001), and lack of hepatic (p=0.004), peritoneal (p=0.001), and lymph node (p=0.013) metastasis remained significantly associated with patient survival but DP-negativity with PPARγ-positivity lost significance (p=0.579) (Table IV).
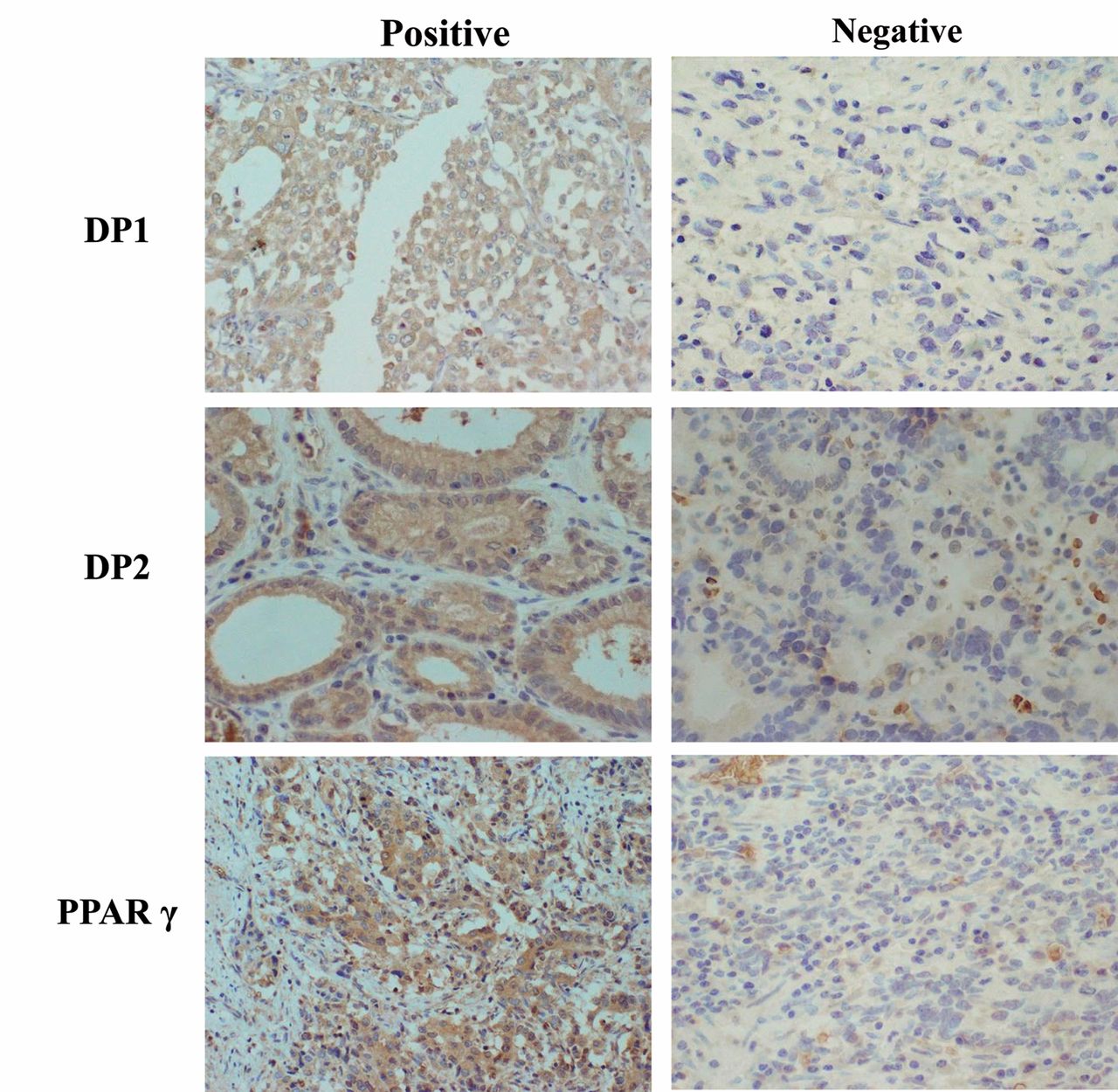
Immunohistochemical determination of type D prostanoid receptor (DP) and peroxisome proliferator-activated receptor γ (PPARγ). DP1 and DP2 were mainly expressed in the membrane and cytoplasm of gastric cancer cells. PPARγ was mainly expressed in the cytoplasm and nuclei of gastric cancer cells. The expression was evaluated by the intensity of staining and percentage of stained tumor cells.
Discussion
PGD2 acts through DP1 and DP2, as well as PPARγ. In the present study, DP1 expression was associated with invasiveness, including invasion depth and lymph node metastasis, whereas no significant association was observed between DP2 expression and clinicopathological features. These findings suggest that DP signaling, particularly PGD2/DP1 signaling, is associated with tumor invasion. In contrast, PPARγ alone was not associated with any clinicopathological factor.
Association between type D prostanoid receptor (DP) 1 and DP2 expression and clinicopathological factors.
Reports on the correlation between DP expression and PPARγ expression are limited. The mechanism of action of these receptors in relation to PGD2 signaling in cancer has remained elusive. A negative correlation between DP-negative PPARγ-positive tumors and invasion and lymph node metastasis was found here. It has been reported that PGD2/DP1 signaling plays an important role in the predisposition of postcolitis rats to colorectal cancer (23). On the other hand, an inverse correlation between PPARγ expression and tumor size, histological grade, axial lymph node metastasis, and breast cancer prognosis has been reported (24). The results of this study indicate that PGD2/DP1 signaling was associated with increased malignant potential, which includes invasion, and that PGD2/PPARγ signaling might act as growth inhibitors. In addition, the findings of the current study suggest that PGD2 signal imparts a wide range of effects on the proliferation of gastric cancer cells, particularly those involving DP and PPARγ signaling. To the best of our knowledge, this is the first report to demonstrate that the effect of PGD2 on the progression of cancer cells may depend on the expression of DP1, DP2, and PPARγ receptors.

Survival of patients. The Kaplan–Meier survival curve of 277 patients with gastric carcinoma. Neither the expression of type D prostanoid receptor (DP) nor of peroxisome proliferator-activated receptor γ (PPARγ) (A, B) correlated with patient survival. However, the overall survival of patients with DP-negative PPARγ-positive tumor was significantly (log-rank; p=0.041) better than that of these with DP-negative and PPARγ-negative tumor, and was significantly (log-rank; p=0.018) better than that of those with DP-positive and PPARγ-positive tumor.
The prognosis of patients with DP-negative PPARγ-positive cancer was found to be better compared with that of other phenotypes. DP and PPARγ can be used as potential predictors of cancer progression. However, multivariate analysis showed that DP-negative and PPARγ-positive expression are not independent prognostic factors.
In conclusion, the expression of DP and PPARγ may represent a clinically useful approach in monitoring the progression of gastric carcinoma.
Association between peroxisome proliferator-activated receptor γ (PPARγ) expression and clinicopathological factors in gastric cancer.
Univariate and multivariate analysis with respect to overall survival of patients with gastric cancer.
Acknowledgements
This study was partially founded by KAKENHI (Grant-in-Aid for Scientific Research, nos. 20591573, 22390262, and 23390329), by the National Cancer Center Research and Development Fund (23-A-9), and by the Foundation for Promotion of Cancer Research. We thank Mayumi Oda (Osaka City University Graduate School of Medicine) for technical advice.
Footnotes
-
Conflicts of Interest
There are no financial or other interests with regard to the submitted manuscript that might be construed as a conflict of interest.
- Received February 28, 2014.
- Revision received March 14, 2014.
- Accepted March 17, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.