


Abstract
Background: Single tumors may show heterogeneity, and it is unclear whether biomarker expression in surgical and diagnostic biopsy samples correlates. Materials and Methods: We retrospectively identified lung cancer patients who were diagnosed by biopsy and underwent surgery between January 2007 and October 2010 at the Shimane University Hospital, Shimane, Japan. Thirty-two patients were identified. The expression of four predictive biomarkers was assessed, namely excision repair cross-complementing gene 1 (ERCC1), ribonucleotide diphosphate reductase M1 (RRM1), thymidylate synthase (TS), and class III beta-tubulin (BT). We also compared immunohistochemical staining in diagnostic biopsy and corresponding resected surgical samples. Results: Moderate correlation was seen between the expression of ERCC1, RRM1, TS, and BT in the biopsy and surgical specimens, with r values of 0.512 (p=0.003), 0.411 (p=0.020), 0.475 (p=0.006), and 0.404 (p=0.027), respectively. Conclusion: Assessment of biopsy samples with immunohistochemical staining is a feasible and reliable method for use in clinical decision making.
Lung cancer is the leading cause of cancer-related death worldwide, and the incidence has continued to increase over the last few decades (1). The standard chemotherapy for non-small-cell lung cancer (NSCLC) is the combination of a platinum-based and a third-generation anticancer drug. Recent advances in the etiology, pathogenesis, and tolerance mechanisms of NSCLC have lead to the development of molecularly-targeted therapy, such as epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors. Targeted-therapies have shown a promising survival benefit in NSCLC patients with EGFR mutations, but only 40% of NSCLC patients have these mutations (2), and cytotoxic anticancer drugs accordingly still play an important role.
Although researchers have identified a number of predictive and prognostic biomarkers of NSCLC, most were identified using resected tumors. Resected tumor samples cannot be obtained from patients with advanced lung cancer, however, and assessment in these cases is performed using small biopsy samples. While several reports have suggested that the assessment of biomarker expression in biopsy samples is useful, it is unclear whether biomarker expression correlates both with resected samples and diagnostic biopsy samples, and only a few reports have confirmed correlations in expression between surgical and biopsy samples (3-5).
Several biomarkers of drug sensitivity are used in the treatment of NSCLC. Excision repair cross-complementing gene 1 (ERCC1) expression is associated with platinum drug sensitivity and prognosis (6-8). Ribonucleotide diphosphate reductase M1 (RRM1) is useful in predicting sensitivity to gemcitabine (9-12). Thymidylate synthase (TS) expression is reported to be a predictive biomarker of sensitivity to pemetrexed (13-15). Class III beta-tubulin (BT) is known as a predictive biomarker of sensitivity to taxans (16-18). Platinum drugs, gemcitabine, pemetrexed, and taxans are key drugs in the treatment of NSCLC, and these four biomarkers are key molecules in predicting sensitivity to treatment. Thus, assessment of these biomarkers may facilitate the development of individualized therapy.
Through comparison of biopsy and surgical specimens, Taillade et al. reported a high correlation for ERCC1 (r=0.83) but low correlation for EGFR and pAkt (r=0.24 and 0.29, respectively), indicating that not all biomarkers can be evaluated by immunohistochemistry (IHC) (3). Chang et al. reported no correlation between TS expression and pemetrexed efficacy (19), whereas Chen et al. reported that these were in fact correlated (14). When findings for predictive biomarkers are negative, it is unclear whether the null result is due to the assessment method or the properties of the molecule itself, and it is therefore necessary to confirm the validity of the assessment method. Nevertheless, correlation of the expression of these four biomarkers between resected and diagnostic biopsy samples has not been reported.
In the present study, to confirm the reliability of assessment of ERCC1, RRM1, TS, and BT biomarkers by IHC, we retrospectively reviewed lung cancer patients who were diagnosed by diagnostic biopsy and underwent surgery and evaluated these four biomarkers in resected tissue and diagnostic biopsy samples with IHC.
Materials and Methods
Study population. The study population consisted of patients with operable and resectable NSCLC who underwent diagnostic lung biopsy and surgical resection between January 2007 and October 2010 at Shimane University Hospital, Shimane, Japan. Patients who had received chemotherapy or radiotherapy before surgery were excluded. We retrospectively identified 32 patients. Diagnostic procedures consisted of transbronchial lung biopsy (n=16) and percutaneous computed tomography (CT)-guided lung biopsy (n=16). Biopsy specimens were fixed in formalin-acetic acid-alcohol (FAA) for 24 h and then embedded in paraffin. Surgical procedures included lobectomy (n=25) and partial lobectomy (n=7). Surgical specimens were fixed in 10% buffered formaldehyde for 48 h and then embedded in paraffin. By histological type, there were 22 adenocarcinomas, 7 squamous cell carcinomas, 1 large cell carcinoma, and 1 pleomorphic carcinoma. According to the TNM staging system, 16 cases were stage Ia disease, 6 were stage Ib, 2 were stage IIa, 4 were stage IIb, 2 were stage IIIa, and 2 were stage IV; and by T factor, 11 samples were T1a, 6 were T1b, 9 were T2a, 1 was T2b, and 5 were T3. The protocol for the study was approved by the Institutional Review Board of Shimane University.
Immunohistochemical procedures. The immunohistochemical procedures used for biopsy and surgical specimens were similar. Formalin-fixed, paraffin-embedded tumor specimens were immunostained using an AutoStainer i6000® (BioGenex, San Ramon, CA, USA) for ERCC1, RRM1 and TS, and a BenchMark GX® (Roche, Tucson, AZ USA) autostainer for class III BT. Paraffin-embedded tumor material was cut into 4-μm-thick sections and placed onto glass slides. For IHC staining for ERCC1, RRM1, and TS, the slides were de-paraffinized in xylene and a graded series of ethanol. Slides for ERCC1 and TS antigen retrieval were exposed to Tris-EDTA buffer (10 mM Tris and 1 mM EDTA, pH 9.0) and those for RRM1 antigen retrieval were exposed to citrate buffer (10 mM, pH 6.0). They were then heated in a water bath at 95°C for 30 min and allowed to cool at room temperature for 20 min. Endogenous peroxidase activity was blocked by incubation with 3.0% H2O2 for 10 min. H2O2 was then washed-out with PBS, and slides were incubated with primary antibodies, namely a mouse monoclonal anti-ERCC1 antibody (1:200, 60 min) (clone 8F1; GeneTex, Irvine, CA, USA);, a rabbit polyclonal anti-RRM1 antibody (1:200, 60 min) (ProteinTech; Chicago, IL, USA);, and a mouse monoclonal anti-TS antibody (1:2, 20 min) (clone TS106; Dako, Glostrup, Denmark);. Antibody binding was detected with an Envision detection kit (Dako) using Mayer's hematoxylin as counterstain. For BT staining, the slides were de-paraffinized automatically according to the manufacturer's instructions. Antigen was retrieved by pouring high pH retrieval solution (CC1) (Roche, Tucson, AZ, USA) onto sections that were subsequently placed on a slide heater at 100°C for 30 min. Endogenous peroxidase activity was blocked by incubation with 3.0% H2O2 for 4 min. The samples were then incubated with a mouse monoclonal anti-BT antibody (clone TU20, 1:100, 50 min) (Serotec, Oxford, UK); at 37°C using polymer methods according to the manufacturer's instructions. Then they were counterstained with Mayer's hematoxylin and color was developed with bluing reagent (Roche).
The presence of tumor cells and histotypes was evaluated in the pathology department of our Hospital. Biopsy samples were considered eligible for analysis if there were more than 20 malignant cells on the slide and tumor morphology was well-preserved. Immunohistochemical staining in both biopsy and surgical specimens was evaluated independently by four physicians who were blind to clinical data (TO, YT, AS, and TI). Discordant cases were reviewed by all four physicians, and appropriate scores were obtained by consensus. For ERCC1, RRM1, and TS evaluation, staining intensity was graded on a scale of 0 to 3, with higher numbers indicating higher intensity. Endothelial cells in tonsil control tissue were used as a positive control for ERCC1 and placenta cells as a positive control for RRM1, with both assigned an intensity of 2 (20). A proportion score was assigned in four categories (0 if 0%, 0.1 if 1% to 9%, 0.5 if 10% to 49%, and 1.0 if 50% or more). This proportion score was multiplied by the staining intensity score to obtain a final semiquantitative H score (7, 20, 21). For BT evaluation, cytoplasmic expression was classified into five categories: score 0, no staining at all; score 1+, faint/barely perceptible partial cytoplasmic expression in <10% of tumor cells; score 2+, weak-to-moderate staining of the entire cytoplasm in >10% of tumor cells; score 3+, moderate staining of the entire cytoplasm in >10% of tumor cells; and score 4+, strong staining of the entire cytoplasm in >10% of tumor cells (16). Expression scores which were equal to or less than median values were classified as negative while those which were higher were classified as positive.
Statistical analysis. Statistical analysis was carried out using the SPSS software system, version 20 (SPSS, Chicago, IL, USA). Correlations between biopsy specimens and surgical specimens in the expression of each biomarker were determined using Spearman correlation coefficients. Concordance rate among biopsy methods and tumor size were calculated using the chi square test and Fisher's exact test. p-Values <0.05 were considered statistically significant.
Results
Patients' characteristics. Patients' characteristics are shown in Table I. The 32 eligible patients consisted of 17 males and 15 females, with a median age of 75 (range=33-89) years. Biopsy and surgical specimens were available and assessable for all 32 patients with regard to ERCC1, RRM1, and TS, and for 30 patients with regard to BT. Two biopsy specimens could not be assessed due to insufficient tissue sample for immunostaining.
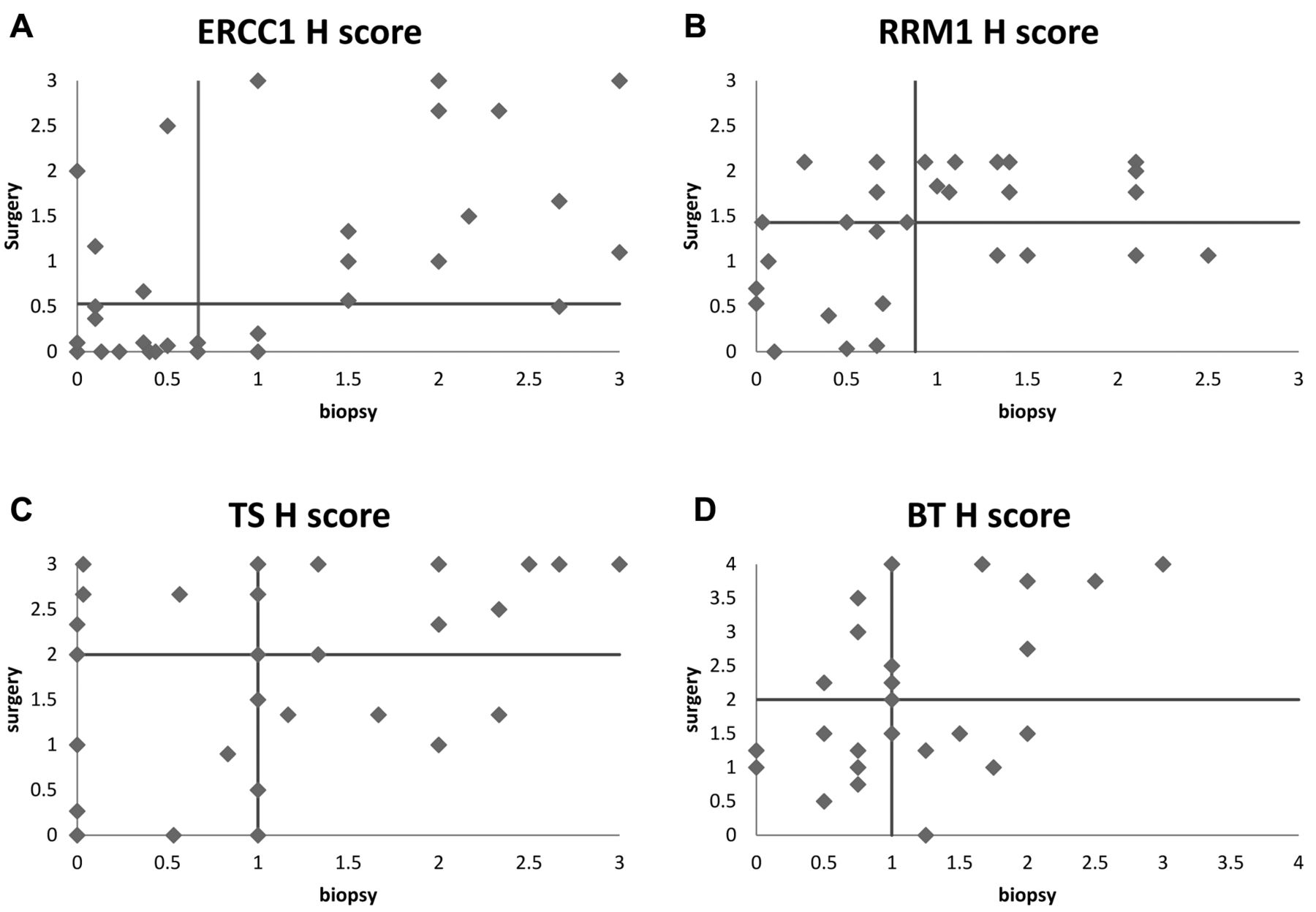
Immunohistochemical assessment. ERCC1. Correlation coefficient between the biopsy and surgical specimens was r=0.512 (p=0.003), and median H score was 0.67 and 0.53, respectively. Fifteen of 32 biopsy specimens and 16 of 32 surgical specimens were positive. Concordance rate was 78.1% (Figure 1A and E) (Figure 2A) (Table II).
RRM1. Correlation coefficient between biopsy and surgical specimens was r=0.411 (p=0.020), and median H score was 0.88 and 1.43, respectively. Sixteen out of 32 biopsy specimens and 14 out of 32 surgical specimens were positive. Concordance rate was 75% (Figure 1B and F) (Figure 2B) (Table II).
TS. Correlation coefficient between biopsy and surgical specimens was r=0.475 (p=0.006), and median H score was 1.00 and 2.00, respectively. Fifteen out of 32 biopsy specimens and 15 of 32 surgical specimens were positive. Concordance rate was 62.5% (Figure 1C and G) (Figure 2C) (Table II).
BT. Correlation coefficient between biopsy and surgical specimens was r=0.404 (p=0.027), and median H score was 1.00 and 2.00, respectively. Ten of 30 biopsy specimens and 14 of 30 surgical specimens were positive. Concordance rate was 53.3% (Figure 1D and H) (Figure 2D) (Table II).
Discussion
In the present study, we demonstrated the feasibility of simultaneous assessment of the expression of four key predictive biomarkers in the treatment of NSCLC in samples of small size. We also confirmed a moderate correlation among them, with correlation coefficients for ERCC1, RRM1, TS, and BT of 0.512, 0.411, 0.475, and 0.404, respectively. To our knowledge, this is the first study to identify these correlations. These findings suggest that expression of these biomarkers in biopsy samples can be reliably used in the development of individualized therapies.
Cobo et al. reported that 27 out of 228 TBLB samples in their study were too small of a number for polymerase chain reaction (PCR) evaluation of mRNA ERCC1 gene expression (22). In our study, we used immunohistochemical staining and found that almost all samples (94%) were adequate for analysis. If samples are large enough to be used to diagnose lung cancer, the addition of IHC assessment is not particularly difficult. IHC is not as expensive as PCR methods and can be easily implemented in routine use. Vilmar et al. evaluated the predictive efficiency of quantitative reverse transcriptase (qRT-)PCR and IHC for ERCC1, breast cancer susceptibility gene 1 (BRCA1), RRM1, and BT in surgically-resected tissue samples from NSCLC patients. Results showed a higher predictive value on assessment by IHC, and the authors concluded that IHC discriminated more effectively across these four biomarkers than qRT-PCR (23).
Patients' characteristics (n=32).
Several prospective trials have investigated the use of these biomarkers in treatment decision making. In a prospective phase II clinical trial in patients with advanced NSCLC, Simon et al. determined RRM1 and ERCC1 gene expression and selected chemotherapy regimens based on the results (24), while Cobo et al. conducted a phase III clinical trial which compared control (cisplatin/docetaxel) and genotypic arms (cisplatin/docetaxel or gemcitabine/ docetaxel) based on ERCC1 expression (22). Both trials showed higher response rates than previous studies, and suggested that evaluation of ERCC1 expression was a feasible and useful method of genotyping. Although many studies have suggested the usefulness of specific biomarkers in predicting the efficacy of chemotherapy, we are unaware of any that have evaluated the four present biomarkers together. Combined assessment of these biomarkers will likely facilitate the selection of promising drugs for not only first-but also second-line and later chemotherapy, which may lead to an improved quality of life for patients and prolonged survival.
Gene expression profiles dichotomized according to cut-off rates based on media H scores.
The concordance rate for ERCC1, RRM1, TS, and BT between biopsy and surgical samples was 78.1%, 75%, 62.5%, and 53.3%, respectively. Although the correlation coefficient of these biomarkers was not markedly different, discordant cases were nevertheless seen in TS and BT scores. We adopted the median H score as the cut-off value. For these two biomarkers, a relatively high number of tumors had the same score as the cut-off value (25% of TS scores and 17% of BT scores), which may have resulted in a lower concordance rate. This question might be resolved by determining the appropriate cut-off values in a larger study. If the H score of these biomarkers is in fact found to center around the median values, use of tri-chotomized evaluation (negative, positive, intermediate) based on chemotherapeutic efficacy might improve concordance.
Evaluation of biomarker expression on the basis of IHC requires for use of appropriate cut-off values. Many processes in IHC can affect dye affinity, and immunohisto-chemical assessment requires operator skill. Herein, results were assessed by four physicians and discordant cases were reviewed to assure accuracy. Adoption of IHC assessment into clinical practice requires that each Institution determine appropriate cut-off values, which in turn requires larger clinical trials. We are now evaluating patients with advanced NSCLC who were diagnosed by biopsy and underwent chemotherapy; results may provide the appropriate cut-off value of each biomarker according to chemotherapeutic efficacy and indicate the most appropriate treatment strategy for individual patients.
We also compared TBLB to CT-guided lung biopsies. Larger samples can be obtained with CT-guided core biopsy over TBLB. We used a 16 or 20 gauge semi-automatic needle for CT-guided biopsy. Concordance rates in the two groups were not significantly different. Because of heterogeneity in tumor morphology, we expected a higher concordance rate in CT-guided biopsy, which obtains bigger samples, but surprisingly found that the rate with TBLB was not inferior to that with CT-guided biopsy. With regard to ERCC1 assessment, concordance rates were 75% and 81.3% for TBLB and CT-guided biopsy, respectively (p=0.50). Rates for the other biomarkers were not significantly different (p-values for RRM1, TS, and BT were 0.34, 0.53, and 0.12, respectively). Because all eligible samples were from operable cases, most tumors were so small (median: 3 cm) that any heterogeneity in the tumor was likely also small. We also compared concordance rates between T1 and T2 or more advanced stage disease. Differences were again not statistically significant (p-values for ERCC1, RRM1, TS, and BT were 0.54, 0.58, 0.10, and 0.10, respectively). Thus, assessment of biomarker expression with biopsy samples appears to be reliable regardless of tumor size and biopsy method.
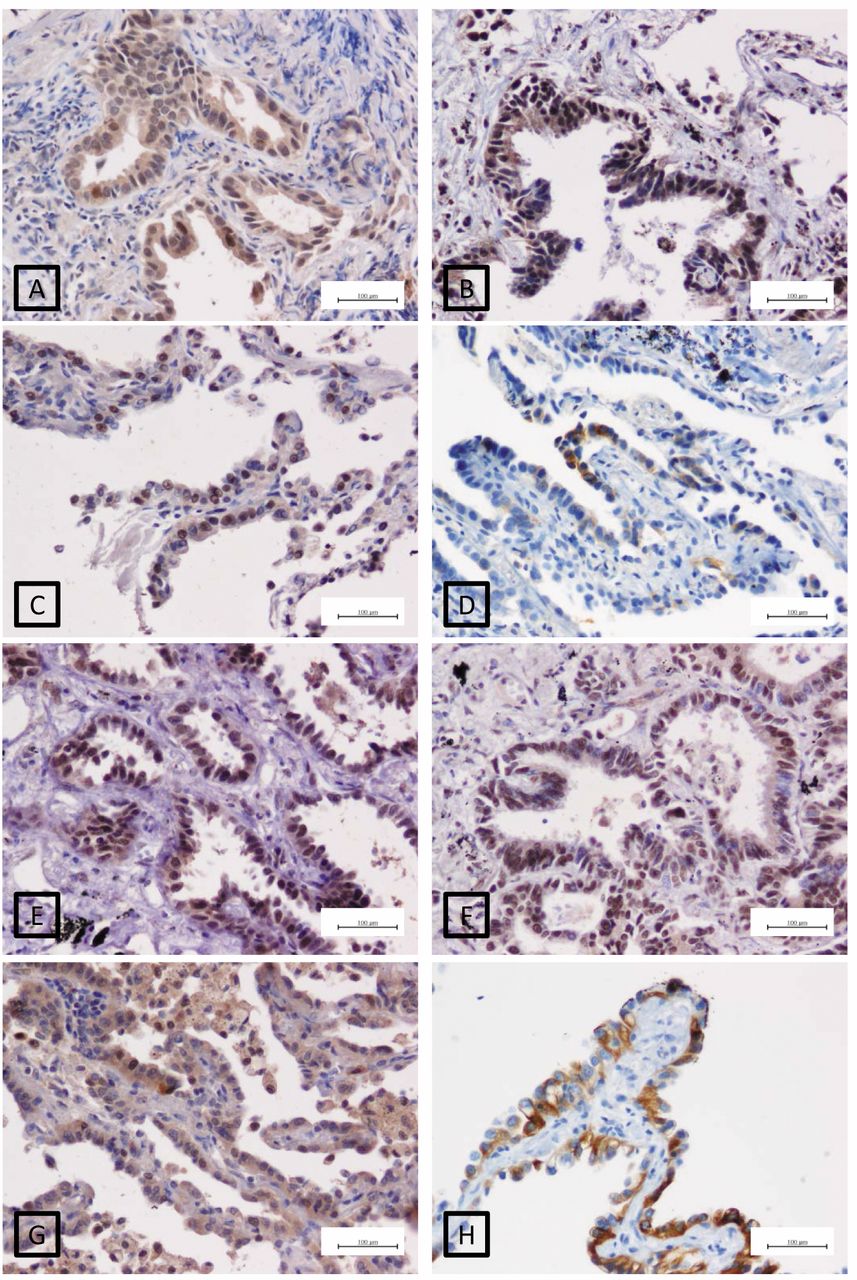
Immunohistochemical staining (original magnification, ×200). A-D: Biopsy samples of adenocarcinoma with positive staining for ERCC1, RRM1, TS, and BT, respectively. E-H: Surgical samples of adenocarcinoma with positive staining for ERCC1, RRM1, TS, and BT, respectively.

A: ERCC1 expression in biopsied versus paired resected tumors. B: RRM1 expression in biopsied versus paired resected tumors. C: TS in biopsied versus expression in paired resected tumors. D: BT in biopsied versus expression in paired resected tumors.
Several limitations of the study warrant mentioning. First, the number of the subjects was small, and all had operable tumors. Second, biopsy samples and corresponding surgical samples were not dyed together. Although we used an autostainer for IHC, antigen retrieval for ERCC1, RRM1, and TS was performed manually, which might have influenced dye affinity. Third, although ERCC1 is an intra-nuclear protein, both the nucleus and cytoplasm were positive in this study. We used the 8F1 clone for ERCC1 staining here, although a previous study reported that this clone is sometimes positive in cytoplasm and therefore has the possibility of non-specific staining (25). A prospective study enrolling a larger sample, concurrent staining of tissue samples, and use of a more specific stain for ERCC1 would address these limitations.
Conclusion
We showed that a correlation exists in the expression of ERCC1, RRM1, TS, and BT in biopsy and surgical specimens in patients who had undergone surgery for NSCLC. IHC assessment can be performed in small tumor samples and provides promising data for designing individualized therapy. Introduction into clinical practice awaits retrospective confirmation of the usefulness of this analysis and the establishment of appropriate cut-off values.
Acknowledgements
Financial support for this study was provided by the Japan Society for the Promotion of Science, Grants-in-Aids for Scientific Research. We thank Ms Yumi Nishio for her secretarial assistance.
Footnotes
-
This article is freely accessible online.
- Received February 11, 2014.
- Revision received April 29, 2014.
- Accepted April 30, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}