


Abstract
Background: Only scanty data are available to evaluate the impact of sequential TKIs on overall survival (OS) in patients with metastatic renal cell carcinoma (mRCC). This retrospective study investigated the efficacy of the sequence sorafenib–sunitinib (SO-SU) and vice versa (SU-SO) in a real-life scenario. Patients and Methods: Median progression free-survival (PFS) and OS were evaluated. The correlation between PFS and OS was also assessed. Results: In total, 104 patients received SO-SU and 21 (16.8%) SO-SU. No differences in PFS or OS were observed (PFS for SO-SU=26.1 months, and for SU-SO=20.0 months; OS=35.3 and 27.0 months, respectively). For both sequences, only a weakly-positive correlation between PFS and OS was observed. Conclusion: Our data support the use of the sequence of the two TKIs in a real-life setting. No strong evidence of a correlation between PFS and OS was observed.
The treatment of metastatic renal cell carcinoma (mRCC) has changed dramatically over the last few years, thanks to the introduction into the pharmaceutical armamentarium of seven novel targeted therapies. Indeed, the therapeutic scenario has shifted from cytokine-based therapy to the use of multi-targeted tyrosine kinase inhibitors (TKIs), such as sorafenib, sunitinib, pazopanib and axitinib, the monoclonal antibody to vascular endothelial growth factor (VEGF) bevacizumab, and the inhibitors of mammalian target of rapamycin (mTOR) everolimus and temsirolimus (1).
These targeted therapies have led to consistent improvements in treatment outcomes; however, complete cure of patients is seldom achieved (1, 2). In fact, in spite of considerable delays in tumor progression, complete and long-lasting responses are reported in fewer than 5% of patients (3). Therefore, these drugs mostly play the role of palliative treatment, with an efficacy that decreases over time (2).
Given the unfavourable results obtained with combination therapy, sequential therapy using targeted agents now represents the current standard strategy in the treatment of mRCC, with the aim of extending survival and maximizing the clinical benefits (2, 4).
After disease progression on frontline therapy, the switch to a second targeted agent allows disease control and, in addition, increases progression-free survival (PFS) and may even extend overall survival (OS) (4). Nevertheless, there is no clear consensus on the most appropriate sequencing of drugs after disease progression in mRCC (5-8).
The relationship between PFS and OS has been demonstrated in several solid tumor types treated with conventional chemotherapy; however, this correlation has not been clearly established in mRCC treated with targeted agents (9). In fact, even if PFS was found to be significantly superior for the experimental arm of pivotal phase III studies, a superiority in OS was not achieved in the same arm (9).
This retrospective study investigated the efficacy of two different sequential approaches based on the two strategies sorafenib followed by sunitinib (SO-SU) and vice versa (SU-SO) in patients with mRCC treated in a referral Center.
Patients and Methods
This retrospective study was conducted at the National Cancer Institute of Milan, Italy – a referral Centre for the treatment of oncological diseases in Northern Italy – between November 2007 and January 2012. Patients had given their informed consent to the use of their data for research purposes and the local Ethical Committee approved (INT 81/11) the study design.
The study was conducted on a population of 366 patients with mRCC who received at least one targeted agent. In more detail, patients aged ≥18 years with mRCC, a life expectancy of at least three months and an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0, 1 or 2 were required for inclusion. One hundred and eighty (49%) patients received only one targeted agent, while the remaining 186 (51%) received two or more targeted agents.
We only considered for our analysis patients who received either the SO-SU or the SU-SO treatment strategy. SO was admin¬istered orally, at a dose of 400 mg twice-daily; SU was given at a daily dose of 50 mg orally, with a ‘4 weeks on 2 weeks off’ schedule.
Patients' demographics and disease characteristics.
PFS and OS were evaluated by Kaplan–Meier analysis. The log-rank test was used to detect any statistical difference in PFS or OS. The correlation between PFS and OS was measured with the Kendall's Tau non-parametric index. A p-value <0.05 was considered statistically significant.
Results
Patient population. A total of 125 patients were included in the study. Tables I and II show patient and disease characteristics, respectively.
The majority of patients (104, 83.2%) were treated with the sequence SO-SU and were followed for a period of 66.6 (range=6.0-84.1) months. On the other hand, 21 patients (16.8%) received the sequence SU-SO, with a median follow-up of 37.1 (range=4.0-60.1) months. Patients' characteristics are shown in Table I.
In both treatment groups, 38 patients also received a third or further line of targeted therapy. In the SO-SU group, 25 (24%) patients received a third-line, nine (8.7%) a fourth-line, and one (1%) patient a fifth-line of treatment. In the SU-SO group, four (19%) patients received a third-line and a fourth-line therapy.
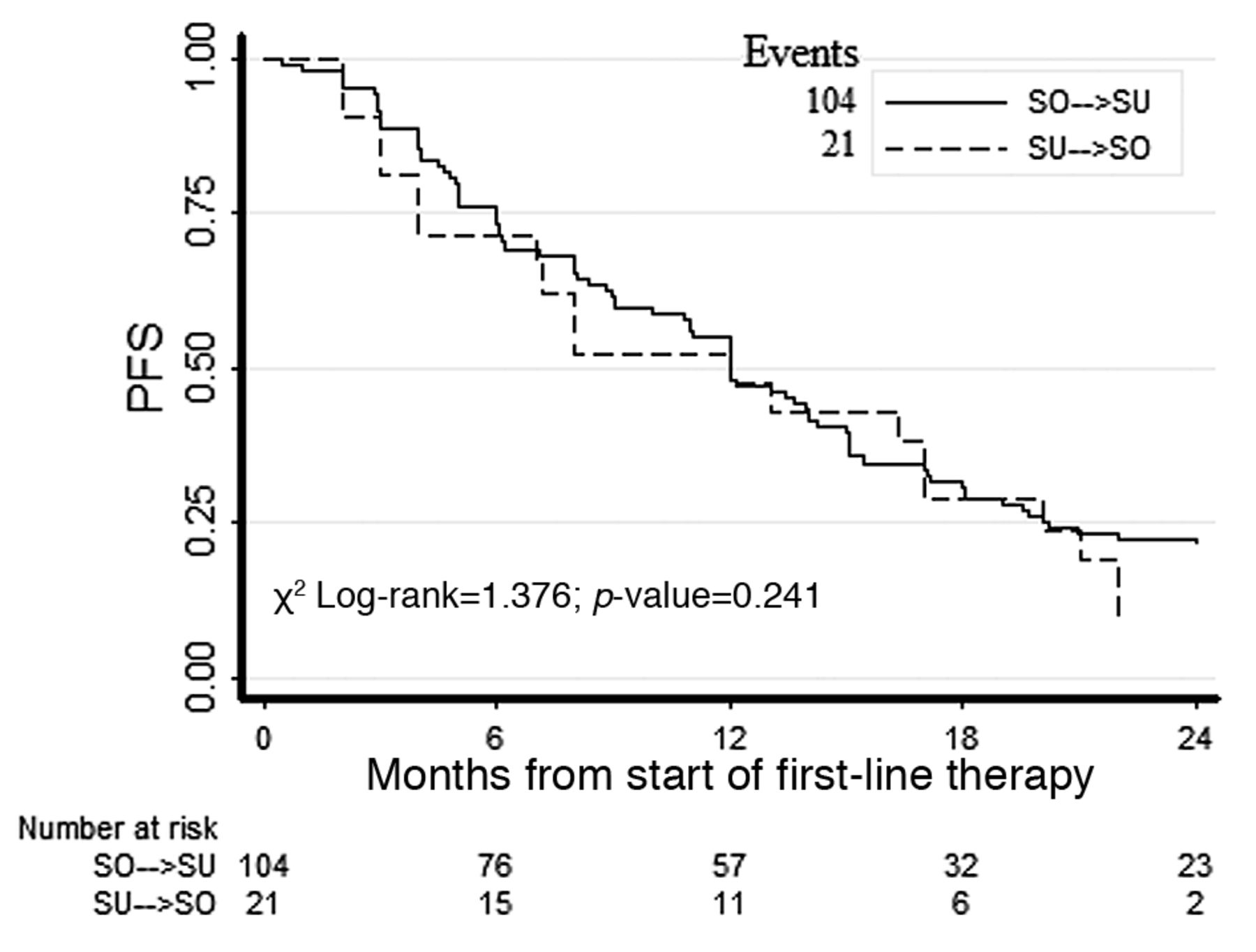
Survival. At the time of analysis, 37/125 (30%) patients were still alive and 27/125 (22%) were progression-free. No statistical difference in PFS was observed between the two treatment groups: the median PFS for SO-SU was 26.1 months (12 months in first-line plus 14.1 months in secondline; 95% CI=21.8-34.0 months), while that for SU-SO was 20 months (12 plus 8 months; 95% CI=10.0-33.0 months) (Figure 1). The median PFS after first-line treatment with either SO or SU was 12 months.
Baseline characteristics by treatment sequence.
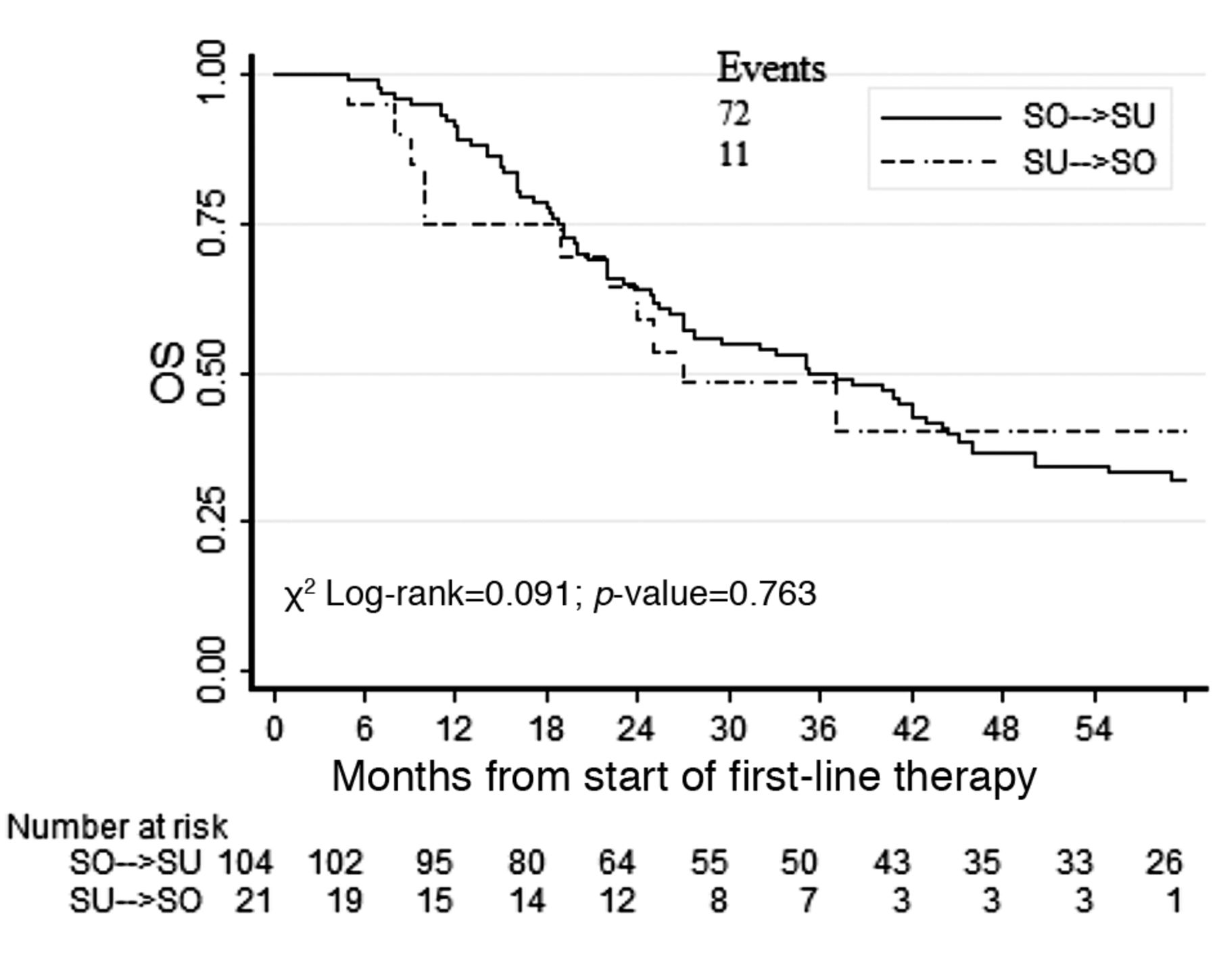
Similarly, no statistical difference in OS was observed between the two treatment groups: the median OS for SO-SU was 35.3 (95% CI=26-44.4) months, while that for SU-SO was 27 (95% CI=10.0-ND) months (Figure 2).
For both SO-SU and SU-SO treatment sequences, a weakly-positive correlation between PFS and OS was observed, τ=0.13 and τ=0.15 respectively (Figure 3).
Discussion
Our study has shown a favourable trend, in terms of PFS, for the sequence SO-SU: 26.1 (95% CI=21.8-34) months and 20 (95% CI=10-33) months for the reverse sequence. However, statistical significance has not been reached. This finding is in line with the results of a meta-analysis of 853 patients included in prospective and retrospective studies which documented a benefit, often significant, for the sequence SO-SU when compared to the opposite sequence (10).

Progression free survival in sunitinib (SU)-sorafenib (SO) and SO-SU treatment groups.

Overall survival in sunitinib (SU)-sorafenib (SO) and SO-SU treatment groups.
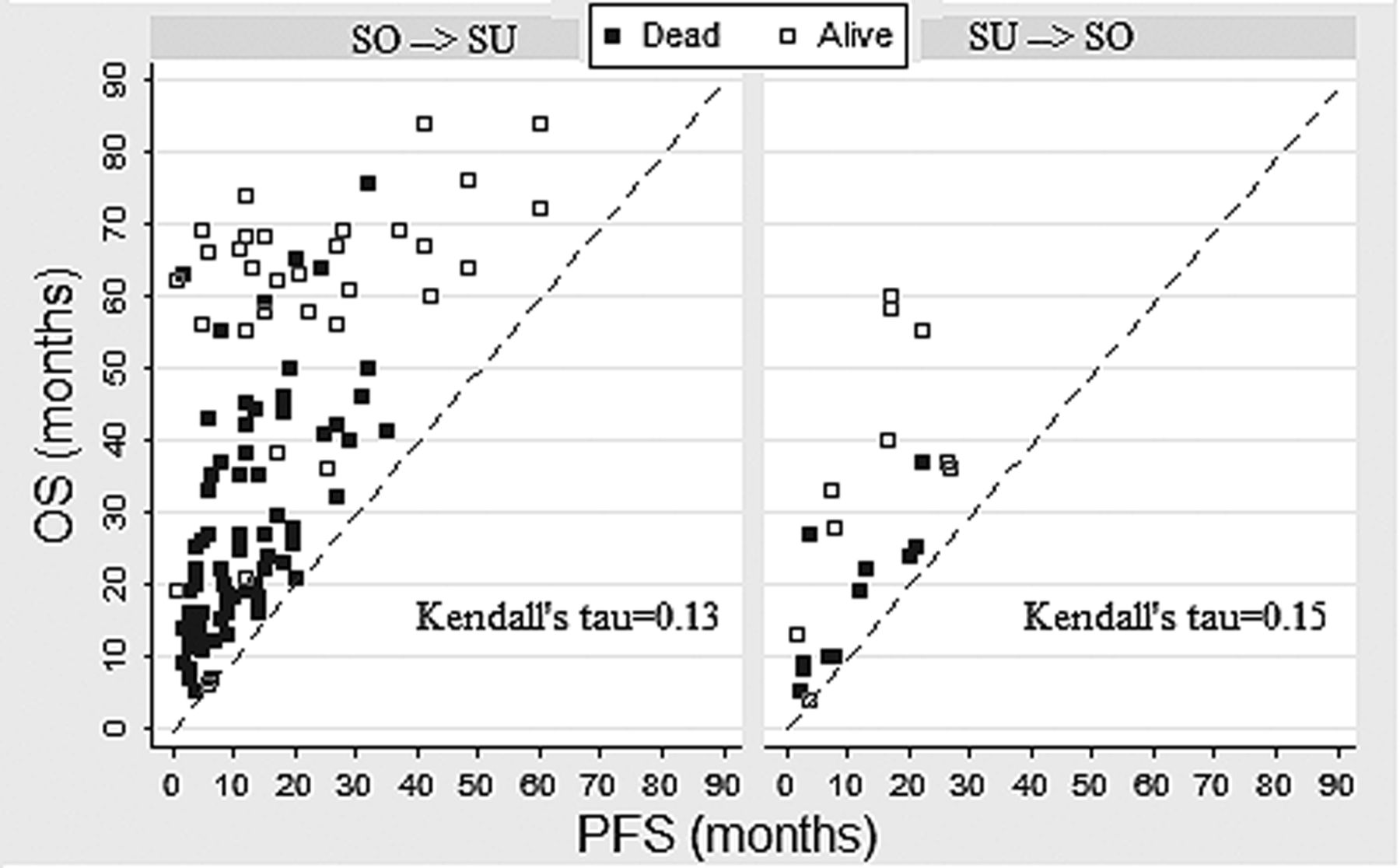
Correlation between progression-free survival (PFS) and overall survival (OS) according to Kendall's Tau index in the SO-SU and SU-SO treatment groups.
Many biases could have influenced our investigation. First of all, the two sub-groups of the study population were not well-balanced. The population undertaking the sequence of SO followed by SU was larger: 104 versus 21 patients for the opposite sequence. In addition, patients on SO-SU were followed-up for a longer time (66.6 months versus 37.1 months). Another bias lies in the imbalance of patients evaluated according to Motzer prognostic factors. Indeed, more poor-risk patients did receive the SU-SO sequence (23.8% versus 7.7%). In addition, the number of patients previously treated with cytokines was higher in the SO-SU group (42.3% versus 14.3%). Finally, we must acknowledge that similarly to what is repeated in other single-Center retrospective studies, the contribution of our study to the identification of the best therapeutic sequence is at best limited: it is likely that the best sequential strategy in RCC will be only identified following the results of the multicenter phase III trial currently ongoing (11).
With respect to OS, our study reported a median of 35.3 months for the sequence SO-SU, and 27 months for the opposite sequence. As seen for the PFS, this difference was not statistically significant. Noteworthyily, the median OS using the sequence SO-SU was quite high and may confirm the positive synergistic effect of this sequence of TKIs reported by some authors (4, 12).
In our study, the non-parametric index Kendall's Tau, which indicates the correlation between PFS and OS in both sequences, reported only a weakly-positive correlation (r=0.13 and r=0.15, for SO-SU and SU-SO, respectively). This result seems to be in line with currently available data which show that an increased PFS should not be considered as a fully valid surrogate for OS (4).
With the goal of establishing the correct sequence for targeted-therapy in RCC, prospective studies are ongoing and could confirm the findings in clinical practice. In particular, the results of the two SWITCH 1 and SWITCH 2 studies (the latter a phase III study evaluating the best sequence between sorafenib-pazopanib and pazopanib-sorafenib) are awaited (11, 13). We believe that due to the high number of targeted agents presently available, it will not be possible to definitively position any drug in a well-defined sequence. We speculate that sequence studies only provide general information, and not inflexible rules for allocating therapy to each patient. Therefore, in agreement with many others, it is our opinion that in the absence of unmistakable predictive factors, the choice of RCC therapy should take into consideration the evaluation of patient comorbidities, through a patient-focused approach, and the rate of invasion of disease (11, 14-16).
In conclusion, data from this retrospective, imbalanced, field-practice study support the sequence of the two TKIs in a real-life setting. Patients who received two TKIs had an OS benefit, potentially due to the synergistic effect of therapies. No strong evidence of a correlation between PFS and OS was observed.
Acknowledgements
Editorial assistance for this manuscript was provided by Dragonfly Editorial, funded by Bayer HealthCare.
Footnotes
-
Conflicts of Interest
Giuseppe Procopio is member of the advisory board of the pharmaceutical companies Astellas, Bayer, GSK, and Pfizer. For the remaining authors, no conflicts were declared. The Authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in this article apart from those disclosed.
- Received January 22, 2014.
- Revision received March 24, 2014.
- Accepted March 27, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}