


Abstract
Background: The prognostic value of lymph node (LN) status in patients who underwent resection for pancreatic cancer (PC) was examined in the present study. Patients and Methods: Fifty-six patients who underwent macroscopic curative resection for PC were analyzed. Twelve factors, including the number of LN metastases, LN ratio, and N category according to the Japanese Pancreatic Society classification, were analyzed using univariate and multivariate analysis. Results: The optimal cut-off value was 0.2 for the LN ratio. Positive surgical margins (p=0.022) and LN ratio ≥0.2 (p=0.017) were identified as independent prognostic factors. Among the 33 patients with regional LN metastasis, patients with LN ratio ≥0.2 had significantly worse prognosis than those with LN ratio <0.2 (median survival time 14 vs. 26 months, p=0.048), however, the differences in survival between those with N1 and those with N2 by Japanese Pancreatic Society classification were not statistically significant (p=0.85). Conclusion: The LN ratio might be more useful than other parameters as a predictor for survival after resection of PC.
Patients with pancreatic carcinoma have a poor prognosis, with a 5-year survival rate of approximately 10-20%, even after curative tumor resection (1-6). Lymph node involvement in particular, which develops in 60-70% patients with pancreatic cancer (2, 5, 6), has been described as one of the most important prognostic factors (5-10). Despite recent advances in surgical techniques, chemotherapy, and radiotherapy for pancreatic cancer, the prognosis of patients with lymph node (LN) metastasis of pancreatic cancer remains unsatisfactory.
In patients with other types of gastrointestinal cancer, the number of LNs harvested, the number of metastatic LNs and the ratio of metastatic-to-examined LNs (LN ratio) have been demonstrated to be important prognostic factors, rather than nodal disease alone (11-15). Recently, the gastric cancer nodal staging was changed in the Japanese Gastric Cancer Association 14th edition staging system, so that the staging now depends solely on the number of metastatic nodes found instead of their distance from the primary lesion (16). Regarding pancreatic cancer, the Union for International Cancer Control (UICC) (17) staging system classifies the N category into only two groups with respect to the presence or absence of nodal disease. On the other hand, in the Japanese Pancreatic Society (JPS) classification (18), LN metastasis is classified into four groups according to the distance from the primary site, while the regional LNs of the pancreas are classified into two groups. Similar to other types of gastrointestinal cancer, the number of LNs harvested, the number of metastatic LNs and the LN ratio may be superior to the staging used by the UICC or JPS classifications for pancreatic cancer. However, there are only limited data available on the prognostic value of these nodal factors following pancreatectomy (19-21).
The aim of the present study was to evaluate predictors of survival in patients who undergo resection for pancreatic cancer, focusing specifically on the prognostic value of the LN ratio, the number of LN metastases, the number of resected nodes, and the N category used in the JPS classification.

Lymph node groups for tumor of the pancreas by the Japan Pancreas Society classification system. The tumor is located in the head (A) or body and tail (B). Names of lymph nodes are described elsewhere (18).
Patients and Methods
Study population. The clinical records of 81 patients who underwent macroscopic curative pancreatectomy for pancreatic cancer between January 2001 and December 2009 were reviewed retrospectively. Macroscopic curative resection was defined as the absence of apparent tumor residue in the operative field without liver metastasis or macroscopic peritoneal dissemination. Out of these, 11 cases of pancreatic cancer derived from intraductal papillary mucinous neoplasms (IPMN), nine of pancreatic cancer cases with IPMN, five of pancreatic cancer cases with other cancer were excluded, and a total of 56 patients with pancreatic cancer were analyzed in the present study. All 56 patients had invasive ductal carcinoma of the pancreas.
Our principal criteria for performing pancreatectomy included the absence of: hepatic metastases, macroscopic peritoneal seeding, bulky lymph node involvement, cancer invasion to the superior mesenteric artery (SMA) or common hepatic artery (CHA) and occlusion of the portal vein. Tumors abutting the entire circumference of the SMA/CHA or the encasement of the SMA/CHA were contraindicated for pancreatectomy. Thirty-seven patients underwent pancreaticoduodenectomy, 16 patients underwent distal pancreatectomy and three patients underwent total pancreatectomy. In the present study, all patients underwent D2 lymphadenectomy according to the JPS classification, which was defined as complete removal of group 1 and group 2 lymph nodes (Figure 1). Twenty-three patients received adjuvant chemotherapy: 13 patients received gemcitabine alone, two patients received S-1 alone, six patients received gemcitabine plus S-1, and two patients received uracil–tegafur as adjuvant chemotherapy. No patients received adjuvant radiotherapy or chemoradiotherapy. All patients were examined in the outpatient clinic where abdominal ultrasound, computed tomography (CT) and measurement of the levels of carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9) were performed every three to six months after surgery.
The tumors were staged according to the UICC (17) and JPS classifications (18). Figure 1 shows the lymph node groups for tumors of the pancreas in the JPS classification system. The extent of metastasis according to the JPS classification is as follows: pN0, no LN metastasis; N1, metastasis to group 1 LNs without metastasis to group 2 or 3 LNs; N2, metastasis to group 2 LNs without metastasis to group 3 LNs; N3, metastasis to group 3 LNs. Group 1 and 2 l LNs are treated as regional LNs. Metastasis to the group 3 nodes is considered to be equivalent to distant metastasis. The LN ratio was defined as the number of positive LNs divided by the total number of LNs examined. Twelve clinicopathological factors, including the number of LNs metastases, the number of dissected LNs, the N category according to the JPS classification and the LN ratio, were analyzed using univariate and multivariate analyses.
The cut-off value for the lymph node ratio, the number of lymph node metastases, and the number of resected lymph nodes.
Statistical analysis. The ‘optimal’ cut-off values for the number of positive LNs, the LN ratio and the number of LNs examined were determined using p-values that were calculated using the log-rank test. The minimum p-value indicated the ‘optimal’ cut-off value. Survival was calculated using the Kaplan–Meier method and compared between groups using the log-rank test. A multivariate analysis using a Cox hazard model was performed to identify independent predictors of survival. All statistical analyses were performed using the Software Package for Social Sciences, version 11.5J for Windows 1 (SPSS, Chicago, IL, USA). A value of p<0.05 was considered to be significant.
The results of the univariate and multivariate analyses of prognostic factors associated with overall survival in the 56 patients with invasive ductal carcinoma of the pancreas.
Results
The overall 5-year survival rate was 29.5% and the median survival time was 25.1 months. The number of LNs evaluated was 27.3±15.3 (mean±SD), with a median of 25. The number of LN metastases was 2.8±3.3, with a median of 2. The LN ratio was 0.1±0.1, with a median of 0.07. Based on the minimum p-values, the optimal cut-off values were 0.2 for the LN ratio, 2 nodes for the number of positive LN and 10 nodes for the number of resected LNs (Table I).
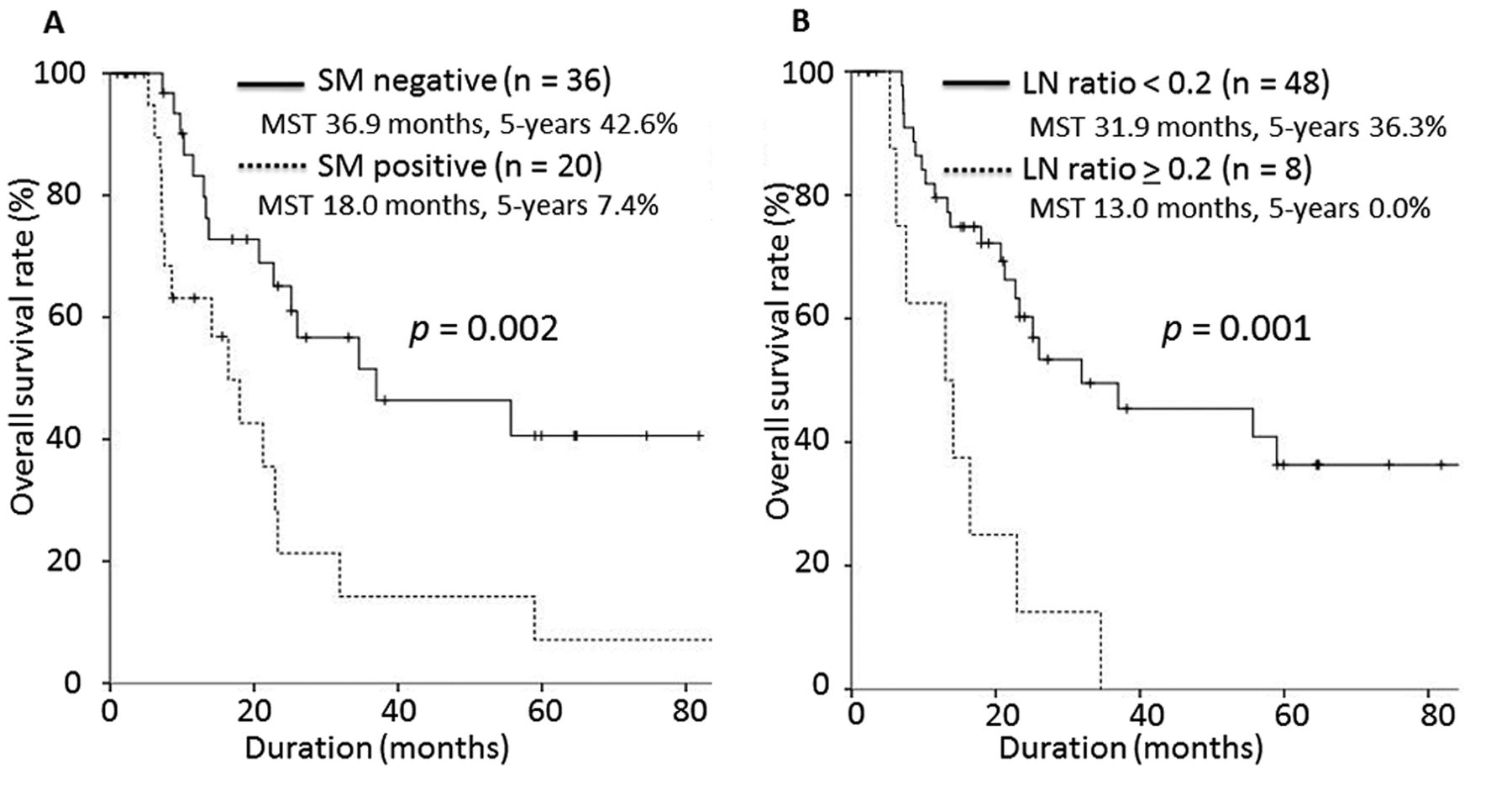
Table II summarizes the results of the univariate and multivariate analyses of the prognostic factors associated with overall survival. In the univariate survival analysis, retropancreatic invasion (p=0.027), a positive surgical margin (p=0.002), number of LN metastases ≥2 (p=0.010) and a LN ratio ≥0.2 (p=0.001) were significantly associated with a worse prognosis. The multivariate survival analysis showed that a positive surgical margin (p=0.022) and an LN ratio ≥0.2 (p=0.017) were independently associated with a poorer prognosis (Figure 2).

The overall survival curve according to the status of surgical margins (A) and lymph node ratio (B). Multivariate survival analysis showed that positive surgical margins and a lymph node ratio ≥0.2 were independently associated with a poorer prognosis.
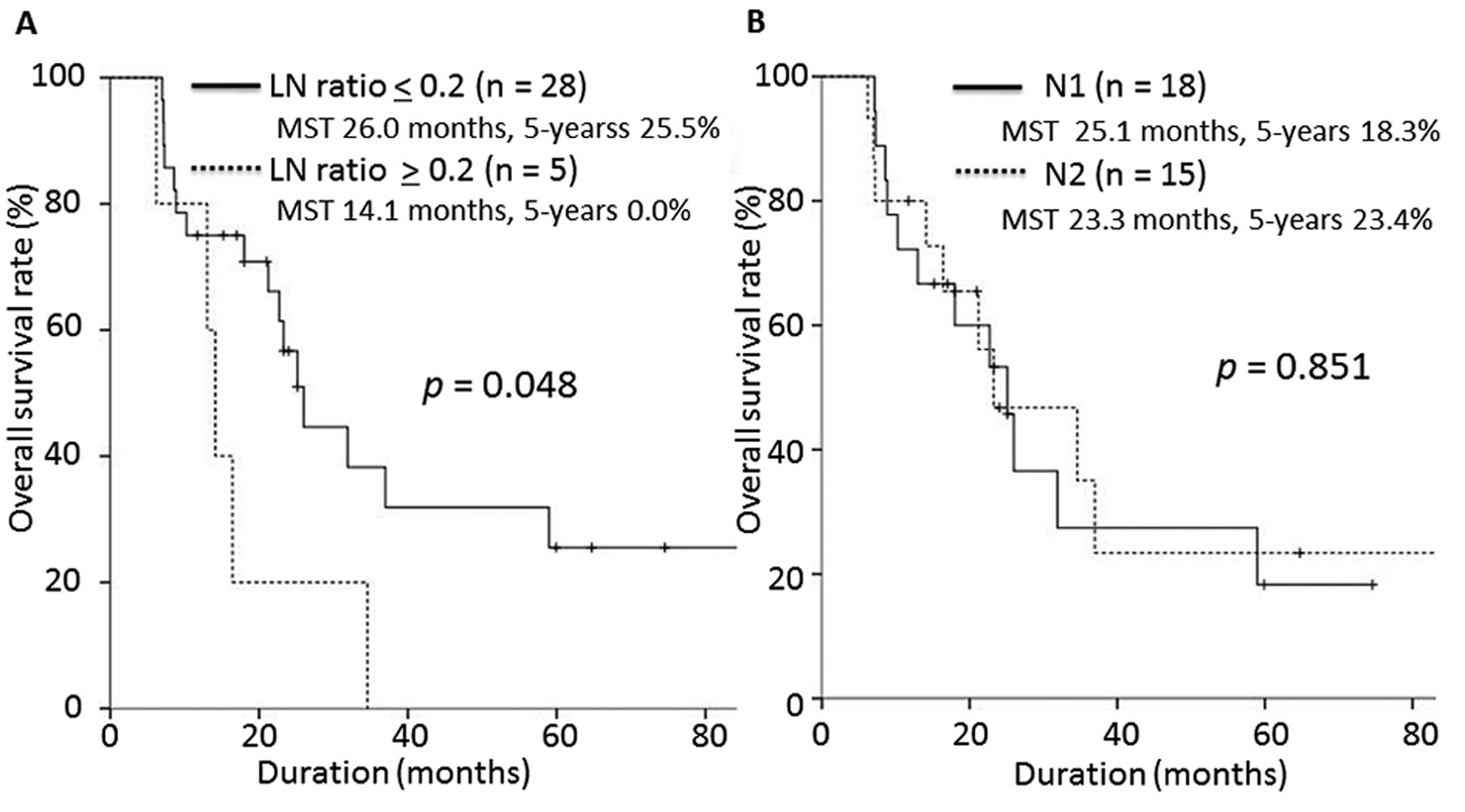
With regard to the sub-group analysis of the 33 patients with regional LN metastases (N1 or N2 in the JPS classification), there were significant differences in the survival rates between patients with an LN ratio ≥0.2 and those with an LN ratio <0.2 (median survival time (MST) 14.1 vs. 26.0 months, p=0.048; Figure 3A); however, the differences in survival between those with N1 and N2 in the JPS classification were not statistically significant (MST 25.1 vs. 23.3 months, p=0.851; Figure 3B).
Discussion
Metastatic disease to regional LNs is a well-known important prognostic factor in patients undergoing pancreatectomy for pancreatic cancer (22). Recently, the clinical importance of the LN count (20) and the LN ratio (19, 21) for survival following surgery for pancreatic cancer has been reported. Some studies have shown a correlation between a large number of LN metastases and survival rates (17). However, the number of LN metastases is associated with possible stage migration because this number is influenced by the number of LNs resected and examined. Regarding gastric cancer, stage migration of up to 15% can be observed when at least 15 nodes are dissected after gastrectomy (15). On the other hand, the LN ratio refers to the tumor characteristics of LN metastases and the therapeutic characteristics of the degree of dissection, and can be used to better identify subgroups of patients with various types of cancer, thereby minimizing the stage migration phenomenon (11-15).
D2 lymphadenectomy is widely-applied as the standard operation for treating pancreatic cancer in Japan. However, some randomized controlled studies of patients with pancreatic cancer have indicated that extended lymphadenectomy leads to a high rate of operative morbidity and does not increase the survival rates compared with D1 lymphadenectomy (24-28). If D1 lymphadenectomy were to become a common operative method for treating pancreatic cancer, many patients would obtain no information regarding LNs other than peri-pancreatic nodes. Therefore, correctly classifying LN involvement based on the sites of positive LNs according to the JPS classification may be difficult unless patients undergo D2 lymphadenectomy. At present, the utility of D2 dissection has not been confirmed, and it may not be useful to classify regional LNs based on the site and distance of metastatic LNs from the primary tumor. Therefore, a new classification should be established to more easily and appropriately estimate the prognosis. The present study showed that using the LN ratio might be more feasible, reproducible and accurate for assessing prognostic stratification without stage migration. However, Matsuno et al. reported that the N category in the JPS classification was significantly meaningful in a large series of 23,302 cases (2). Further investigations are required to confirm the applicability of stage definition.
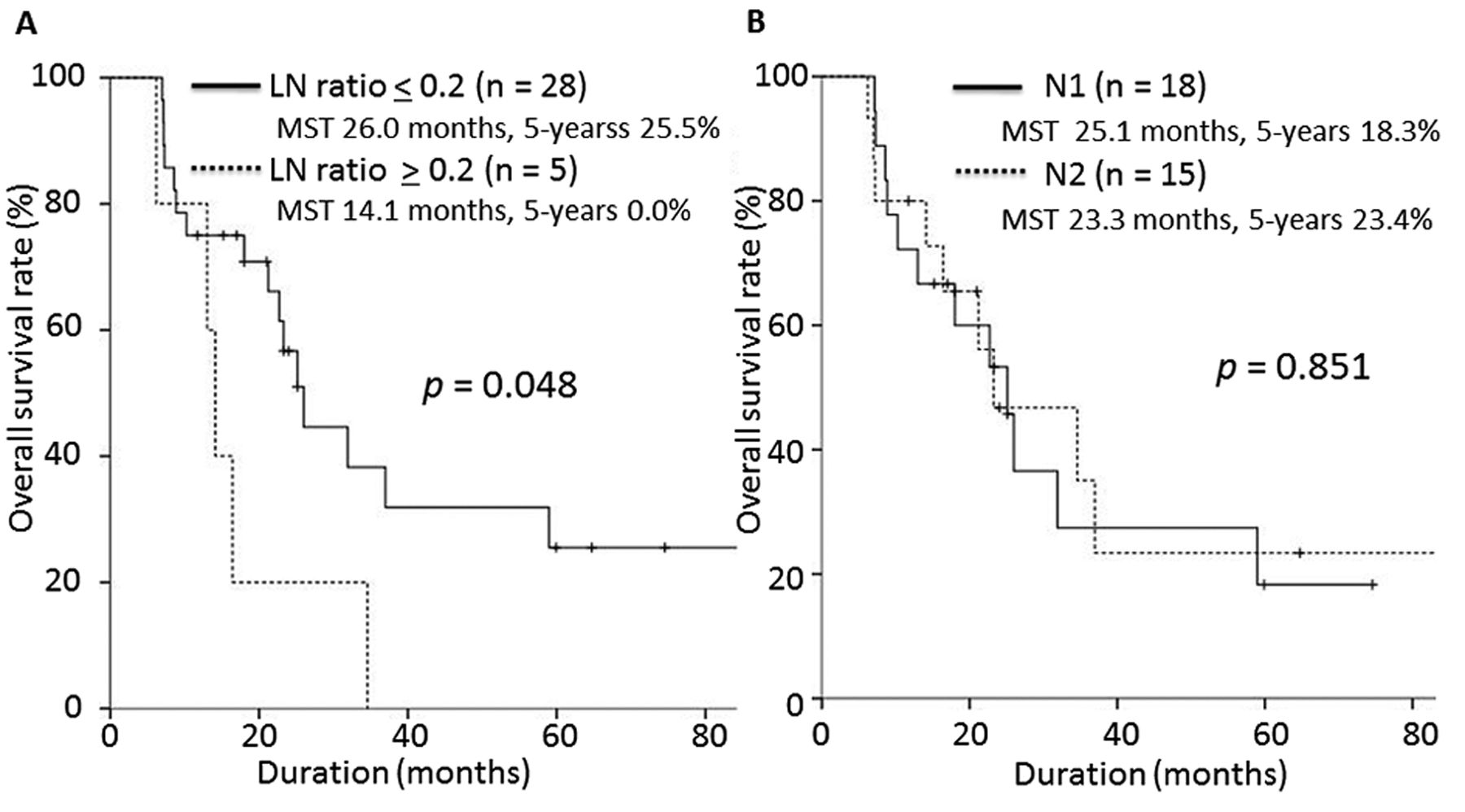
The overall survival curve according to the lymph node ratio (A) and N category by the Japan Pancreas Society classification (B) in the subgroup analysis among the 33 patients with regional lymph node metastases.
Data exist regarding the importance of the number of LNs analyzed for survival following surgery for pancreatic cancer (23). The number of LNs examined differs in individual Institutions. Pawlik et al. reported that the median number of lymph nodes evaluated at Johns Hopkins Hospital was 17 (21), while Slidell et al. reported that the median number of LNs evaluated in the Surveilance Epidemiology, and Endo Results (SEER) dataset was only 7 (29). Schwarz et al. stated that both the LN ratio and the number of lymph nodes examined are important prognostic factors and that the attempt to examine at least 15 total LNs, or approximately 10 negative LNs for curative-intent pancreatectomy, is advisable to optimize operative benefits (23). It is true that the number of LNs analyzed may reflect the therapeutic measure of lymphadenectomy; however, there were no significant differences in the number of LNs examined in the present study.
Although some authors have indicated the superiority of the metastatic LN ratio in assessing pancreatic cancer, definitions of the significant prognostic cut-off point vary. Slidell et al. reported that an LN ratio ≥0.4 is a strong prognostic indicator with a hazard of death similar to the presence of distant metastasis (29). However, other authors have shown similar deteriorations in prognoses when the LN ratio is greater than 0.2, as demonstrated in the present study (30, 31). Further analyses involving a large number of cases regarding the significant prognostic cut-off point of the LN ratio in pancreatic cancer are necessary.
The use of retrospective analyses in a relatively small case series is a limitation of the present study because all cases originated from a single institution. To objectively evaluate the significance of the LN ratio, a prospective, multi-institutional, randomized trial is necessary.
In conclusion, our results suggest that the LN ratio may be more useful than the number of LN metastases, the number of dissected LNs, and the N category of the JPS classification as a predictor for survival after pancreatectomy in patients with pancreatic cancer.
- Received January 27, 2014.
- Revision received April 1, 2014.
- Accepted April 2, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}