


Abstract
Background: This study was the first multicenter phase II study of cetuximab plus folinic acid/5-fluorouracil/irinotecan (FOLFIRI) in KRAS wild-type mCRC as a second-line treatment in Japan including BRAF and PIK3CA genotyping. Patients and Methods: Tumors of 112 pre-registered patients were genotyped for KRAS, BRAF, and PIK3CA. The primary study end-point was response rate, and secondary end-points were progression-free survival (PFS), overall survival (OS), and safety. Results: Sixty-seven patients (59.8%) were EGFR-positive and KRAS wild-type. The mean age of the enrolled patients (n=60) was 62.6 years (range=37-82 years). The response rate was 31.7% and stable disease was observed in 53.3%. No objective response was observed in patients with BRAF or PIK3CA mutations. The median PFS and OS were 7.4 and 18.2 months, respectively. Grade-3/4 adverse events were leucopenia (26.7%), neutropenia (43.3%), paronychia (10.0%), fissure (10.0%) and acne-like rash (5.0%). Conclusion: Second-line cetuximab plus FOLFIRI was effective and well-tolerated.
Colorectal cancer is the fourth most common cancer worldwide, and the number of patients affected by this disease continues to steadily grow (1-3). It is estimated that approximately 92,000 new cases of colorectal cancer are diagnosed each year in Japan (4). Infusion of folinic acid, 5-fluorouracil (5-FU) and irinotecan is known as the FOLFIRI regimen and is one of the standard first- and second-line chemotherapeutic regimens for patients with metastatic colorectal cancer (mCRC). The FOLFIRI regimen has been shown to be more effective than infusion of 5-FU with folinic acid-only (LV5FU2 or AIO regimen) in terms of response rate (FOLFIRI: 41% vs. LV5FU2/AIO: 23%), time-to-progression (TTP) (FOLFIRI: 6.7 vs. LV5FU2/AIO: 4.4 months), and median survival time (MST) (FOLFIRI: 17.4 vs. LV5FU2/AIO: 14.1 months) as first-line treatment (5). Cetuximab is a human/mouse chimeric monoclonal antibody of the immunoglobulin G1 (IgG1) subclass that targets the epidermal growth factor receptor (EGFR), inhibiting EGFR signaling and producing antitumour effects by competing with ligands at the EGFR (6-7). Cetuximab, administered alone or in combination with irinotecan, showed efficacy in the treatment of patients with EGFR-positive mCRC, who were refractory to irinotecan (8). Subsequent studies confirmed the efficacy and safety of cetuximab alone or in combination with chemotherapy (9, 10). Based on the results of these studies and a Japanese phase II clinical study (14), in which cetuximab was administered in combination with irinotecan in 39 patients with EGFR-positive mCRC refractory to irinotecan, in July 2008, cetuximab was approved for second-line and later treatment for EGFR-positive mCRC in Japan.
Genetic features of the V-Ki-ras2 Kirsten rat sarcoma viral oncogene homologue (KRAS) have been reported to predict patient response to cetuximab (11,13). The CRYSTAL (cetuximab combined with irinotecan in first-line therapy for mCRC) study reported the impact of KRAS mutation on outcome in patients receiving FOLFIRI, with or without cetuximab (12). This study evaluated a total of 1,063 patients from the original intention-to-treat (ITT) population of 1,198 patients. The KRAS-evaluable population had similar overall outcomes and characteristics to the ITT population. Patients with KRAS wild-type tumors benefited significantly from the addition of cetuximab to FOLFIRI. The response rate and median progression-free survival (PFS) in the cetuximab/FOLFIRI arm for patients with KRAS wild-type were 57.3% and 9.9 months, respectively. This rate was significantly better than the outcomes obtained with FOLFIRI alone, which was associated with a response rate of 39.7% and a median PFS of 8.4 months. Patients with KRAS mutations did not benefit from the addition of cetuximab, showing response rates of 31.3% and 36.1% and a median PFS of 7.7 months and 7.4 months in the FOLFIRI-alone and cetuximab/FOLFIRI arms, respectively. The overall survival (OS) also significantly improved with cetuximab/FOLFIRI in patients with wild-type KRAS (median OS of 23.5 months vs. 20.0 months for FOLFIRI alone). OS was reduced in patients with mutated KRAS, irrespective of cetuximab administration (16.2 months for FOLFIRI/cetuximab vs. 16.7 months for FOLFIRI-alone) (15). These studies demonstrated that cetuximab plus FOLFIRI as first-line therapy produced significant survival benefits for patients with mCRC. However, there are few reports on the efficacy and safety of cetuximab-plus-FOLFIRI as second-line therapy. In the National Comprehensive Cancer Network (NCCN) guideline (2014, version 2) (16), the recommended second-line chemotherapies for patients with wild-type KRAS initially treated with FOLFOX (folinic acid, 5-FU, and oxaliplatin) or capecitabine and oxaliplatin (CapeOx) regimens are FOLFIRI or irinotecan, with or without cetuximab or another EGF antibody, panitumumab.
The efficacy and safety of cetuximab in combination with FOLFIRI have not, therefore, been adequately reported. The objectives of the present study were to determine the efficacy of cetuximab-plus-FOLFIRI treatment as a second-line chemotherapy for mCRC in patients with wild-type KRAS, and to evaluate the safety profile of the specific treatment.
Patients and Methods
Patients. All patients included in this study provided written informed consent. Those included had histologically-proven, unresectable mCRC with at least one measurable lesion, according to the response evaluation criteria in solid tumors (RECIST) (17). They had an Eastern Cooperative Oncology Group performance status (ECOG PS) of 0 or 1 and adequate organ function for study treatment. All patients were 20 years old or more and had a life expectancy of at least three months. They had previously received at least one regimen of oxaliplatin-containing chemotherapy, at least 28 days prior to the first study treatment. For inclusion in the study, each patient's primary or metastatic tumor tissue needed to have immunohistochemically-confirmed EGFR expression and KRAS wild-type sequences at codons 12 and 13. Each of the patients included in the study had previously had surgery and tumour samples had been stored.
Analysis of tumor EGFR expression. The paraffin-embedded tissues fixed in 10% neutral buffered formalin were cut at 4 μm thickness. Immunostaining of sections was performed using the EGFR pharmDx™ kit (Dako, Glostrup, Denmark) according to the instructions of the manufacturer. EGFR expression was defined as membranous immunohistological brown staining of tumour cells. Positivity for EGFR expression was taken as any membranous staining above background level, whether this was complete or incomplete circumferential staining. The primary tumor was considered positive when 1% of tumor cells had membranous staining.
Tumor KRAS, BRAF and PIK3CA genotype analyses. DNA extraction was performed using a QIAamp DNA FFPE Tissue kit (QIAGEN, Tokyo, Japan) according to the manufacturer's instructions. Mutation of KRAS at codons 12 and 13, BRAF at codon 600, PIK3CA at exons 9 and 20 were determined by direct sequencing as previously described (18). Briefly, each region was amplified by PCR using: KRAS primer set (forward, F: ACCTTATGTGT GACATGTTCTAATATAG, reverse, R: GAATGGTCCTGCACCA GTAA); BRAF primer set (F: TCAT AATGCTTGCTCTGA TAGGA, R: GGCCAAAAATTTAATCAGTG GA), PIK3CA primer sets (9F: GCTTTTTCTGTAAATCATCTGTG, 9R:CTGAGATCAGCCA AATTCAGT, 20F: ACATTCGAAAGACCC TAGCC, 20R: GCAA TTCCTATGCAATCGGTC) and Taq polymerase with 3’-exonuclease activity (Ex Taq; Takara, Tokyo, Japan). Purified PCR products were used as a template for cycle sequencing reactions using a BigDye terminator v3.1 cycle sequencing kit (AppliedBiosystems, Foster City, CA, USA), and the reaction products were applied to an ABI 3500 Genetic Analyser (Applied Biosystems).
Study design. This phase II, multicenter, open-label, single-arm study was conducted in Japan. The study protocol was approved by the Institutional Review Board at each study site. Patients received cetuximab in combination with a FOLFIRI regimen. The initial dose of cetuximab was administered as a single intravenous infusion over 2 h at 400 mg/m2, followed by weekly 1-h infusions at 250 mg/m2. Prior to cetuximab treatment, patients received an anti-histamine and a corticosteroid to reduce the risk of infusion reaction.
Study end-points and assessments. The primary end-point of this study was the response rate, determined using the RECIST criteria (version 1.0). The secondary end-points were disease control rate (DCR), PFS, and OS. PFS was determined from the day of study enrolment to the last study contact date when patients were alive and had not shown disease progression. OS was calculated from the day of study enrolment to death. Safety end-points included the incidence and severity of adverse events (AEs). AEs were graded based on the National Cancer Institute common terminology criteria for AEs (version 3.0) (19).
Patient demographics and characteristics at baseline.
Statistical analysis. All analyses were performed using SAS (version 9.2; SAS Institute, Inc., Cary, NC, USA). Frequency counts and percentages are provided for categorical variables. Response rate and DCR were reported as a proportion of the study population, with 95% binomial confidence intervals (CI). Continuous variables were summarized using mean, median, standard deviation (SD), and range. Survival curves were drawn by the Kaplan–Meier method and a 95% CI for the median survival time was constructed using a Greenwood formula.
The target sample size of 50 patients to investigate treatment response effects was based on expected and threshold response rates of 16% and 4%, respectively, with α=0.05 (one-sided), β=0.1, and binomial distribution.
Results
Patients' characteristics. From December 2008 to November 2009, a total of 112 patients were pre-registered. Of these, 45 were excluded (40.2%) as they had KRAS mutations (37 in codon 12, 8 in codon 13). The most frequent KRAS mutation was GGT→GAT at codon 12.

Therapeutic effects: Progression-free survival (PFS) curve. CI: Confidence interval, MST: median survival time.

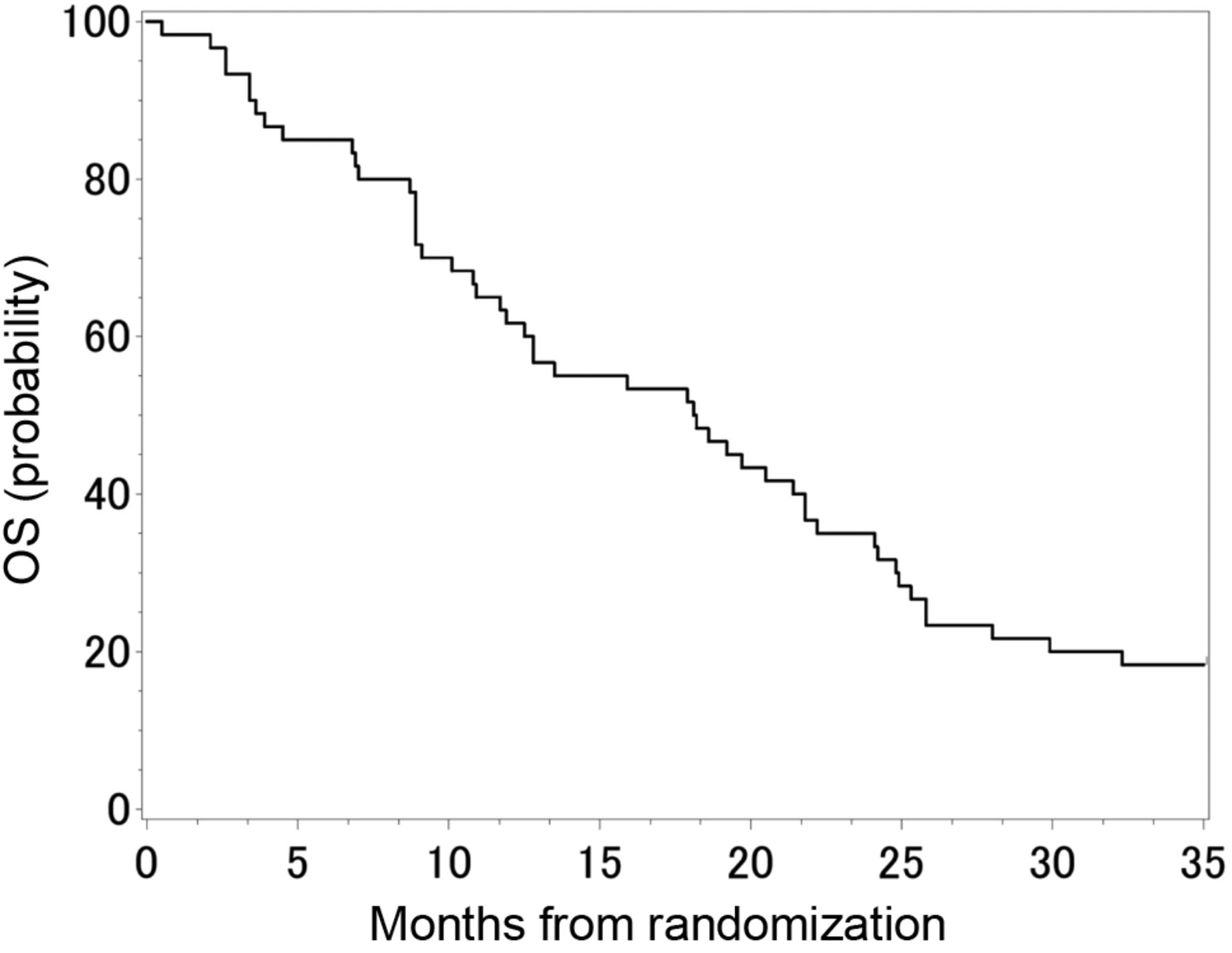
Therapeutic effects: Overall survival (OS) curve. CI: Confidence interval, MST: median survival time.
Sixty patients satisfied the inclusion criteria and were enrolled. The patient demographic characteristics are shown in Table I. The median patient age was 62 years (range=37-82 years), and 65% were male. The median follow-up period was 39.7 months. Fifty-four (90%) and six (10%) patients had an ECOG PS of 0 and 1, respectively. Thirty-two (53.3%) of the 60 patients had received bevacizumab-plus-FOLFOX therapy before registering in this study. Twenty-nine patients (63.3%) had liver metastasas. BRAF and PIK3CA mutations were present in three (5.0%) and two (3.3%) tumors, respectively.
Efficacy. Out of the 60 patients enrolled in the study, 19 (31.7%; 95% CI=20.3-45.0%) had a complete or partial response, and 51 (85.0%; 95% CI=73.4-92.9%) had a complete or partial response to therapy, or stable disease, as determined by the investigators. For the comparison with the threshold 4% response rate, the one-sided p-value was <0.0001. In addition, the response rate and DCR in individuals with wild-type BRAF and PIK3CA tumors was 34.5% (95% CI=22.2-48.6%) and 90.9% (95% CI=80.1-97.0%), respectively (Table II).
Patient genotype and response to therapy.
The median PFS and OS were 7.4 months (95% CI=5.3-10.1 months) and 18.2 months (95% CI=11.7-21.8 months), respectively (Figures 1 and 2). Patients with BRAF mutations (n=3) showed tumor enlargement of 85.6%, 50.9%, and 12%, and those with PIK3CA mutation (n=2) also showed tumor enlargement of 44.0% and 4.0% (Figure 3).
Safety. Thirty-nine patients (65.0%) withdrew from the cetuximab plus FOLFIRI therapy due to progression of disease, two (3.3%) withdrew due to AEs, and 17 (18.3%) withdrew for other reasons. No patient died within 28 days of the last dose of the study medication. All 60 patients experienced at least one AE during the study, most of which were mild to moderate in severity.
The most common grade 3/4 AEs with FOLFIRI-plus-cetuximab were neutropenia (43.3%), leukopenia (26.7%), and vomiting (5.0%). The only cetuximab-related grade 3/4 AEs were fissure (10.0%), paronychia (10.0%), and acne-like rash (5.0%) (Table III).
Discussion
The present FLIER study was the first to prospectively estimate the efficacy of cetuximab-plus-FOLFIRI as a second-line treatment for mCRC in Japanese patients with wild-type KRAS. FOLFIRI-plus-cetuximab was well-tolerated as a second-line treatment in this study and showed antitumour activity in patients with mCRC. KRAS mutation rates of 37.0% and 37.7% have been reported by large-scale studies (20,21). The KRAS mutation rates found in this study (40.2%) were therefore similar to those of these previous reports.
Adverse events of grade 3 or more in all patients.
In the present study, the response rate was 31.7%. Objective response rates ranging from 17-23% (22-24) have been reported in patients receiving FOLFIRI regimens, and rates of 4-8% (24, 25) have been reported in patients receiving other irinotecan-based therapies (including patients with both wild-type and mutant KRAS tumours). Our response rate was, therefore, higher than that in any previous study of FOLFIRI alone. In addition, all five patients with BRAF and PIK3CA mutations showed tumor enlargement, hence the response rate and DCR in individuals with wild-type BRAF and PIK3CA tumours was 34.5% and 90.9%, respectively. This result was concordant with the previous reports (26).
In the present study, the median PFS and OS were 7.6 and 19.5 months in patients with wild-type KRAS, which were also higher than those previously reported for patients receiving FOLFIRI regimens after failure of oxaliplatin-based therapies (PFS range=3.7-4.7 months; OS range=9.3-10.5 months) (22-24). Thus, addition of cetuximab to FOLFIRI as second-line therapy provided additional benefit to mCRC patients with wild-type KRAS tumours.

Waterfall plot of tumour shrinkage, grouped by BRAF, and PI3KCA mutation status. Each column shows the rate of shrinkage. Pts, Patients; dagger/columns, BRAF mutation; double dagger/columns, PI3KCA mutation.
A recent prospective analysis evaluated the effect of tumor KRAS genotype on the efficacy of second-line panitumumab-plus-FOLFIRI in a phase II, open-label, single-arm study of patients with mCRC (PRECEPT study) (27). That study showed a lower response rate (23%), shorter PFS (6.5 months, 95% CI=4.8-8.3 months) and OS (12.5 months, 95% CI=9.8-19.0 months) in patients with wild-type KRAS mCRC, compared to the findings obtained in our study. Patients in that study had received first-line treatment with bevacizumab-plus-oxaliplatin-based chemotherapy. In the present study, patients had received prior treatment with bevacizumab plus FOLFOX (n=32, 53.3%); FOLFOX-alone (n=14, 23.3%); FOLFOX-plus-cediranib or placebo (n=11, 18.3%), and others (n=3, 5.0%). Second-line irinotecan-based chemotherapy is commonly used in mCRC after first-line oxaliplatin-based chemotherapy. A recent randomised phase III study (TML; ML18147) reported the effects of second-line bevacizumab-plus-chemotherapy in mCRC patients who were previously treated with bevacizumab-plus-chemotherapy (28). This TML study showed a 5.4% response rate, PFS of 5.7 months, and OS of 11.2 months. Thus, cetuximab can be a highly effective second-line treatment, even in patients already treated with bevacizumab.
A phase II study of second-line bevacizumab-plus-FOLFIRI was also conducted in patients with mCRC (AVASIRI trial) (29). That study reported a similar response rate (32%), PFS (11.6 months, 95% CI=6.9-16.4 months), and OS (21.4 months, 95% CI=12.0-30.8 months) to those of the present study. This indicated that treatment with an antibody against either EGFR (cetuximab), or an antibody against vascular endothelial growth factor (VEGF, bevacizumab) warrants further validation in a large-scale study.
Recently, the results of an open-label randomised controlled trial comparing irinotecan plus oral S-1 (a combination of tegafur, 5-chloro-2,4-dihydroxypyridine, and potassium oxonate; IRIS) with FOLFIRI as second-line chemotherapy for mCRC were reported. This study showed that the IRIS treatment resulted in a PFS that was not inferior to that associated with FOLFIRI treatment in patients receiving second-line chemotherapy for mCRC (30).
In the present study, the major common haematological grade 3/4 AEs were neutropenia (43.3%) and leukopenia (26.7%). Grade 3/4 acne-like rash and diarrhea were observed in only 5.0% and 1.7% of the patients, respectively. No patients in the present study exhibited any levels of hypomagnesaemia. A previous study of second-line panitumumab plus FOLFIRI in patients with wild-type KRAS reported grade 3/4 AEs of neutropenia (23%), skin-related toxicities (28%), diarrhea (14%), and hypomagnesaemia (8%). Moreover, grade 3/4 AEs of neutropenia (64%), leukopenia (16%), and diarrhea (8%) were reported following second-line bevacizumab-plus-FOLFIRI. In both of these studies as well as in the present study, high rates of neutropenia were found, with moderate to severe neutropenia occurring in nearly in over one-third of all patients. These findings, taken together with the results of the present study, also emphasize the need to proactively manage skin toxicities (31) and hypomagnesaemia (32) in patients receiving antibody to EGFR.
In summary, the FLIER study was the first study to prospectively estimate the efficacy of cetuximab-plus-FOLFIRI treatment in patients with wild-type KRAS receiving second-line treatment for mCRC in Japan. FOLFIRI-plus-cetuximab was well-tolerated and had antitumour activity as second-line therapy in patients with mCRC.
Conclusion
The present study was the first multicentre prospective phase ll study of second-line cetuximab plus FOLFIRI for patients with wild-type KRAS mCRC in Japan. The KRAS mutation rate in the pre-registered study population was comparable to that reported by previous studies. Cetuximab plus FOLFIRI was well-tolerated and had antitumour activity as a second-line therapy in patients with wild-type KRAS mCRC, producing a treatment response rate of 31.7% and PFS of 7.4 months.
Acknowledgements
This study was supported, in part, by a non-profit organization, Epidemiological and Clinical Research Information Network (ECRIN). We thank Ms. Mai Hatta for her excellent clinical research coordination.
In addition to the Authors listed in the title page, the following investigators and Institutions contributed equally to this study. Hiroyoshi Takemoto: Kinki Cetral Hospital; Kenji Amagai: Ibaraki Prefectural Central Hospital; Yusuke Okuyama: Kyoto First Red Cross Hospital; Toyokawa Akihiro: Yodogawa Christian's Hospital; Nagata Naoki: Kitakyushu General Hospital; Kenji Kobayashi: Matsunami General Hospital; Michio Inukai: Kagawa University Hospital.
Footnotes
-
This article is freely accessible online.
- Received January 28, 2014.
- Revision received February 18, 2014.
- Accepted February 19, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}