


Abstract
Background: Electrochemotherapy (ECT) is proposed as an innovative treatment for cutaneous and subcutaneous primary and secondary malignancies. Its actual application is limited to palliative treatment but recent experience predisposes for its utilization as neoadjuvant and first-line treatment. We explored the clinical application of ECT in a population of patients with head and neck cancer and we critically analyzed our results. Patients and Methods: Nine patients (four females; mean age=62.7 years) with recurrent or persistent squamous cell cancer in the head and neck area were treated with electrochemotherapy (ECT), with the aim of controlling local neoplastic growth and diminish local symptoms (pain, bleeding). Results: Our results in terms of local control and impact on quality of life were evaluated: among 14 lesions assessable for the study, 6/14 lesions exhibited a partial response, 4/14 a complete response, and in four cases we observed progression of the disease. Conclusion: Our personal experience in a heterogeneous, small group of patients with head and neck cancer gave controversial results, with disputable advantages in terms of quality of life improvement. We believe that the critical aspects of ECT in patients with head and neck cancer need to be further analyzed in order to better focus on the role of ECT for head and neck cancer.
Patients with head and neck cancer are currently treated with surgery, radiation therapy or systemic chemotherapy, or their combination. The success rate of multimodality treatment for patients with advanced recurrent disease is low, ranging between 10 and 20% (1). Given the poor response rates in patients with locally advanced disease and the side-effects associated with this standard form of treatment, alternative methods of treatment need to be developed.
Electrochemotherapy (ECT) is a recent therapeutic technique that relies on pulsed, high-intensity electrical currents (electroporation) that reversibly increases cell membrane permeability by creation of pores, through which small molecules, such as chemotherapeutic agents, can diffuse inside cells before they reseal. The two most commonly used drugs are bleomycin and cisplatin (2).
ECT is currently applied in many cancer types, including melanoma (3), basal cell and squamous cell carcinoma (4), Kaposi's sarcoma, and breast cancer, as a palliative treatment in cases of bleeding metastases, or to reduce mass-related symptoms (5). ECT can be proposed as a locoregional therapy for disseminated cutaneous and subcutaneous tumor lesions as an alternative treatment modality to conventional therapies, or as palliative care, in order to improve patients' quality of life (2). In a variable percentage of cases, ECT can achieve complete and durable remission of the disease (6). We report our personal experience in a small and heterogeneous group of patients with head and neck treated with bleomycin-based ECT with palliative intent, and we critically explore the contribution that ECT may make to such fragile patients.
Patients and Methods
Patients. This historical retrospective study was conducted at the First Otorhinolaryngology Unit, University of Pisa, Italy, from May 2010 to January 2013. We enrolled nine patients (4/5 females/males; mean age=62.7 years, range=46-84 years) diagnosed with locally recurrent or metastatic cancer in the head and neck area, after providing written informed consent for treatment with ECT.
The inclusion criteria, derived from European Standard Operating procedures of the Electrochemotherapy (ESOPE) (7), were the presence of a measurable tumor nodule suitable for electrode application and a Karfnoski's performance status of more than 60. Exclusion criteria included American Society of Anesthesiologists (ASA) class of more than 3, epilepsy, brain metastases, pulmonary, cardiac or liver impairment, short life expectancy (<3 months), active infection, previous treatment with bleomycin at maximal dosage, and different anticancer therapies administered within two weeks before ECT.
The histological characteristics of the different subtypes of tumor were assessed: there were eight squamous cell carcinomas and one infiltrating ductal carcinoma, all verified using biopsy. All tumors were recurrences after surgery, radiotherapy with/without chemotherapy; in all cases, the procedure was proposed as a palliative treatment in order to control the ongoing local growth of the lesion. More in detail, in two cases (patients 1 and 5), the tumoral nodules were ulcerated, painful, and bled easily: in particular, patient 5 could not lie on her back because of the huge dressing she had to wear in order to staunch the bleeding. In case 8, the tumoral ulcer was eroding the skin of the chin, possibly determining a wide fistula with the floor of the mouth, and similarly in case 9, the lesion was mainly ulcerative with a superficial wide erosion of the skin of the nose (Figure 1).
Computed tomographic (CT) scans or magnetic resonance (MR) imaging were performed for correct pre-treatment setting. For each patient, target lesions were measured in their largest diameter with a millimeter-scale ruler and registered; patients were asked for acquisition of images of their disease. The clinical features are shown in Table I.
Treatment. All patients were treated under general anesthesia with muscle relaxation, using mivacurium chloride to reduce muscle contractions (8). The electric pulse generator used was the CE-certified medical device Cliniporator™ (IGEA S.p.a., Carpi, Italy). The technical details have been described elsewhere (2, 7): in all cases except one, we utilized type III (exagonal) electrodes, which we considered the most suitable to reach the lesions. In case 2, where the lesion was located in the tongue base, electrode type IV (finger electrode) was utilized. Pulse configuration set was set up in a standard fashion, with an electric field of 1000 V/cm, 100 μs pulse duration and eight pulses for each pulse delivering.
In all cases, we administered intravenous bleomycin at a dose of 15000 IU/m2, in bolus, in a time interval of about one minute. Eight minutes after the infusion, the tumor was treated in overlapping sequences beginning at the margin, including a 1-cm safety margin, and ending in the center of the tumor (Figure 1). The pulses were completed within 30 minutes from the end of bleomycin infusion. In patients 2 and 3, a tracheotomy was performed in order to prevent acute respiratory difficulty because of tissue swelling of the oral cavity or the tongue base (Figure 2). In all cases, we applied a 24-hour elastomeric pump with morphine and ketorolac.
All patients were treated with electroporation once only, except for case 1 where a second application was performed two months later. This study was approved by the Ethical Committee of the University of Pisa (N. 3112).
Results
No intraoperative or immediate postoperative major complications occurred; no serious adverse events were reported. The already known acceptable toxicity profile of bleomycin was confirmed (9).
The immediate postoperative period was uneventful in the majority of cases: patients 1, 4, 5, 6, 8 and 9 were discharged on post-treatment day one. Locally, the treated areas were swollen and painful, but some of them, especially patient 1, reported an immediate sense of relief of the neck constriction he had previously. The healing process was different depending on the treated area: on lesions that were not in contact with saliva, a black eschar formed instead of gray-white necrotic material (Figure 1C). In areas in contact with saliva, a whitish fibrinous material covered the anatomical structures and then a slow mucosal resurfacing, with granulation tissue, was visible.
Patient 2 succeeded in having the tracheotomy removed 10 days after the treatment; she experienced a temporary worsening of pre-existing dysphagia, but recovered completely two months later. The patient was from a foreign country (Poland), and was lost at the third month post-treatment. Preliminary and unconfirmed impression was that she had had a complete response, but information on long-term result is unfortunately not available.
Patient 3 had a wide neoplastic lesion located in the floor of the mouth that eroded the mandible and reached the chin skin (Figure 2). The areas to treat were multiple, a post-radiotherapy trismus was present and consequently, before ECT, a tracheotomy was performed. The patient's wound became infected both on the floor of the mouth and on the skin of the chin. Ulceration of the floor of the mouth became evident five days' post-treatment and worsened day by day. Because of the major ulceration of the floor of the mouth and the swelling of the tissues, the tracheotomy tube was never removed. His general conditions worsened day by day: local edema and suprainfection further complicated the local and general condition, with great increase of pain. The patient died 45 days' post-treatment due to septicemia and cachexia.
Patient 7 showed a partial response of the treated areas (skin and lymph nodes of the neck and of the submandibular region): unfortunately, she rapidly developed additional metastases in the surrounding non-treated areas. We succeeded in discharging the patient only two weeks later because, in the immediate postoperative period, the treated areas were all swollen and covered by a thick eschar. Rapidly, new easily bleeding metastasis appeared in the nuchal area and needed major dressing which the patient's family could not handle by themselves. The patient died of cachexia two months later.
Patient 9 with squamous cell carcinoma of the skin of the nose had a very slow healing process that lasted for almost four months. As a result of ECT, she currently has no visible persistent neoplastic disease but at the same time has bone and cartilage exposure which is a source of moderate pain (with the need for daily paracetamol, 500 mg) and social discomfort due to her facial defect (Figure 3).
In all patients, a close follow-up was planned, with regular clinical examination once a week for the first month and monthly successively. As already stated, patient 2 was lost at follow-up after only three months post-treatment. Patients 1, 4, 5, 6, 8, and 9 attended their appointments regularly. In all cases, the healing process was evident but very slow and never achieved in less than eight weeks. Consequently, we decided to evaluate objective response at the eighth week post-treatment (Table I). Complete clinical response (CR) was found in patient 2 (at 12 weeks post-treatment), in patient 6 (in the upper parotid metastasis) and in patient 4, who after 12 months developed a small local recurrence amenable to minimal surgical excision; patient 4 had a CR again and died of stroke 32 months after the first ECT treatment. Partial response (PR), described as a non-healing wound after more than 8-12-weeks, or in cases of evident tumoral disease together with a volumetric reduction of between 25% and 75%, occurred in four patients, but case 9 was successively defined as a CR at five months post-treatment. In conclusion, of the 14 lesions assessable for the study, 6/14 lesions had a PR, 4/14 a CR, and in four cases we observed progression of the disease.

Case 9, female, 84 years old, squamous cell carcinoma of the skin of the nose. A: Pre-treatment image; B: surgical margins are drawn before starting electrochemotherapy; C: postoperative day 1.
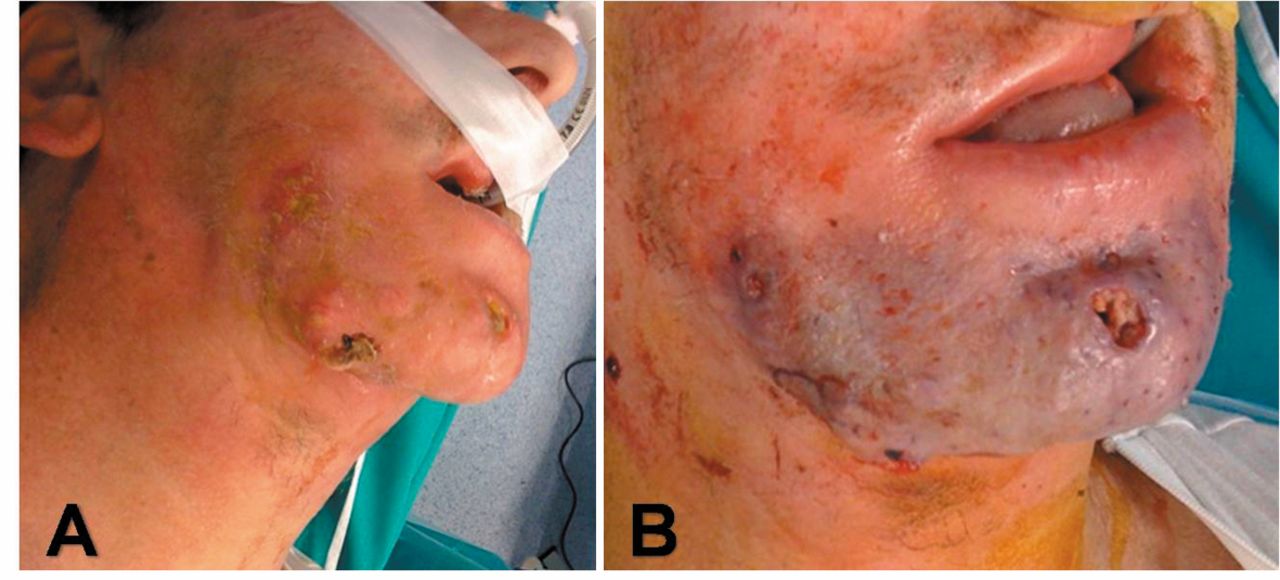
Case 3, male, 52 years old, squamous cell carcinoma of the floor of the mouth extended to the skin of the chin. A: Pre-treatment image; B: post-treatment image, with significant swelling and ecchimosis of the treated area.

Case 9, female, 84 years old, squamous cell carcinoma of the skin of the nose. A: Post-electrochemotherapy (ECT) day 7; B: post-ECT day 30; c: post-ECT day 60.
Patient demographics, clinical features, staging (according to American Joint Committee on Cancer (AJCC) – TNM 7th Edition), treatment and outcomes.
As far as long-term results are concerned, two patients (4 and 9) were successful in obtaining a stable CR in the treated area, whereas all other patients developed local recurrence after a variable amount of time. In all cases with no response or PR, we proposed a second application of ECT in order to achieve better local control, but the remaining patients refused because of the postoperative pain and discomfort.
Discussion
Local recurrences in the head and neck area are challenging for the surgeon and extremely debilitating and disfiguring for the patient whose quality of life can be profoundly affected. Currently, there are no effective pharmacological or radiotherapeutic alternatives; salvage surgery, if feasible, can be rarely proposed without anticipating a severe loss of function. For these reasons, therapies that can control local growth and diminish local symptoms are of great interest and worthy of study.
In the past 10 years, ECT has emerged as a possible therapeutic tool for the control of cutaneous, subcutaneous and reachable mucosal neoplastic lesions. Potential advantages of ECT over conventional treatments are numerous. Drug concentrations are relatively low and administered as a single treatment; side-effects are generally negligible; cancer near critical organs where surgery or radiation therapy can lead to a permanent loss of function can be treated; it has a healing effect, a hemostatic effect, and mass-reducing effect; it is a valid treatment in patients where conventional chemotherapy, surgery, and radiation therapy have failed (10). Furthermore, this treatment modality has the potential of overcoming the multidrug resistance problem and it has also been reported to reduce the number of metastatic nodules when the primary tumor was treated (10). No less importantly, it is generally associated to brief hospitalization, it has a favorable cost–benefit ratio and is repeatable.
Small case series of electroporation and bleomycin therapy in head and neck cancer have been reported in the literature with very promising results (11), as in Gargiulo et al.'s (12) experience (80% CR; 20% PR; N=15). The recent Italian experience of Mevio et al. (13) and Gargiulo et al. (6) confirms the positive impression of the literature with an objective response rate of 94% (N=14) (13) and 100% (N=25) (6), respectively. Following the wave of enthusiasm for ECT, some authors proposed ECT in the preoperative phase as a neoadjuvant treatment, in order to obtain cancer size reduction and to allow easier and less invasive surgical treatment (6, 12).
Our experience differs from all others in terms of results, impact on patients' quality of life and conclusions. Critically analyzing our experience, we surely have two different kinds of bias: firstly, our group is small (N=9), but in line with previously published articles (N=15 (13); N=12 (14); N=1 (15), N=6 (4), and this implies that our considerations today could be completely different on a bigger sample group. Secondly, our patients were all treated for head and neck cancer but with very different subsite involvement (skin of the face, mucosa, neck) and with variable local response. In our opinion, this high variability is our study's point of strength because we are able to provide an all-embracing view of the topic.
Our small experience confirms some of the already known positive aspects of ECT: firstly, we appreciated the very low procedure-related toxicity and side-effects, especially from an anesthesiologic al point of view. The procedure was fast (under 30 minutes), well-tolerated, simple and with a low pain level. Very low technical expertise is required and even in initial cases, we were able to perform ECT without extensive training. We can confirm the good impression of others about the finger electrode (2, 3): it is very helpful in reaching lesions located in the oropharynx or the oral cavity due to the 90° angle between the electrodes and the rest of the device.
In our opinion, intravenous administration allows a more uniform distribution of the drug inside the tumor, especially for large masses, overcoming the potential bias of local administration. An intravenous route is also obviously indicated in cases of multiple nodular lesions.
ECT clinical application in head and neck cutaneous malignancies has already been reported in literature, and our results can be considered superimposable. In some patients, we registered a significant reduction of neck stiffness, of pain, and especially in case 5, of bleeding. In such patients, the increase of the health related quality of life, together with the importance of “doing something” for terminal patients, justifies the risk related to general anesthesia and to the infusion of a chemotherapic drug.
New clinical elements that differ completely from others concern local healing processes, objective response to ECT, impact on quality of life, and possible loss of substance (and function) due to ECT.
As far as healing processes are concerned, none of our patients reached local healing in less than eight weeks: consequently, we postponed the 4/6-week evaluation (3, 6) of treatment to the eighth week, like others (4). We are still looking for a valid endpoint for determining if there is a CR or a PR, and if a second application could be proposed. Our experience shows that a very slow healing or a non-healing wound is not always a sign of non-response to ECT.
As far as local response is concerned, other experience shows that local recovery is generally followed by a second intention healing process (6, 13) that successfully substitutes the lost tissue and its function. Our experience differs from literature in three cases (cases 1, eight and 9) where the local response to treatment was so intense that a wide loss of substance with secondary fistula or abnormal communications were observed. We could not have anticipated such responses, but patients must be forewarned of this possible complication.
In terms of local control, our results are poor, with only 28% of CR, and 42% of PR. Furthermore, in case 3, ECT in fact complicated the clinical course of the patient and surely had a major role in his subsequent septicemia and death. Among the reasons for such a poor result, there is the consideration that all patients were all previously irradiated: previously irradiated fields can cause partial electrode needle penetration and suboptimal electrical current delivery in fibrotic tissue (3).
As far as quality of life is concerned, ECT is nowadays indicated as a palliative treatment, considered as an “approach that is aimed at improving the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spirituality” (16). It is well known that superficial metastases may have a detrimental impact on the patient's quality of life, especially if requiring intensive dressing, so their treatment could ensure the preservation of patient function and well-being (3). Our patients with cutaneous and subcutaneous lesions surely benefitted from ECT in terms of reduction of bleeding (case 5) and reduction of neck pain and stiffness (case 1), with improvement of their quality of life. Conversely, deterioration of quality of life was experienced in patients with a tracheotomy performed with ECT: in fact, the presence of a tracheotomy tube, even if temporary, is a known negative clinical predictor of quality of life, with subsequent depression and physical limitations (17). Our experience suggests that ECT should be carefully evaluated if need for a tracheotomy is anticipated.
Conclusion
Clinical application of ECT to the treatment of primary skin cancer and skin and mucosal metastases related to other malignancies has been consistently expanding in the past decade. ECT represents an effective, safe, and well-tolerated adjunct to the therapeutic options in difficult-to-treat cutaneous tumors, and it is worthy of being considered in selected cases where the extension of the lesion, the number of lesions, or the patient's conditions contraindicate traditional techniques. However, our experience suggests that its use must be seriously evaluated in cases of major head and neck mucosal involvement, in some anatomical sites where the possibility of a complete healing by secondary intention is impaired, and in all cases where a tracheotomy must be anticipated. In the aforementioned cases, the advantages of proposing ECT are not that obvious to the patient and an improvement in quality of life is difficult to demonstrate.
Footnotes
-
Conflicts of Interest
We state that all Authors have contributed to, read, and approved this manuscript.
We declare that this manuscript has not been previously published, nor is it under consideration elsewhere and that none of the authors has any conflict of interest, financial or otherwise. The authors have no commercial, proprietary, or financial interest in the products or companies described in this article.
- Received November 27, 2013.
- Revision received December 22, 2013.
- Accepted December 24, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.