


Abstract
Aim: The aim of the present study was to evaluate the feasibility of, and compliance with a regimen using split-dose cisplatin and vinorelbine (split-CV) as adjuvant chemotherapy in patients with completely resected non-small cell lung cancer (NSCLC). Patiets and Methods: The treatment schedule included cisplatin at 40 mg/m2 and vinorelbine at 25 mg/m2 administered intravenously on days 1 and 8, every three weeks for four cycles. Results: This study included 22 patients (male/female; 12/10) with a median age of 67 (range 50-76) years; 10 had clinical stage II and 12 stage III; 21 had ECOG 0 and 1 patient ECOG 1; 15 patients had adenocarcinoma, 5 squamous cell and 2 adenosquamous carcinoma; 18 patients had undergone lobectomy, 3 pneumonectomy and 1 segmentectomy. Seventeen out of 22 patients (77%) received the planned 4 cycles. The main adverse events were grade 3/4 neutropenia (76%) and anemia (12%). The average total doses of cisplatin and vinorelbine were 285 mg/m2 and 177 mg/m2, respectively. Conclusion: The split-CV regimen is well-tolerated as adjuvant chemotherapy for completely resected NSCLC.
Surgical resection is the only radical treatment for clinical stage IA-IIIA non-small cell lung cancer (NSCLC), except for a limited number of IIIA cases. However, even if a complete resection is performed, recurrence has been reported to occur in 40-60% of patients with NSCLC (1). The majority of recurrences occur at distant sites that usually lead to a fatal outcome. Therefore, effective adjuvant chemotherapy should be administered to reduce the risk of recurrence and to improve prognosis (2).
The Lung Adjuvant Cisplatin Evaluation (LACE) study was a meta-analysis based on individual patients from the five largest adjuvant trials (including the IALT, JBR-10 and ANITA) of cisplatin-based adjuvant chemotherapy published after 1995 (3-8). The LACE study showed a hazard ratio (HR) of 0.89 for death [95% confidence interval (CI): 0.82-0.96, p=0.004], corresponding to an absolute survival benefit of 5.4% at five years (9).
A prospectively planned analysis of the effects of chemotherapy according to regimen in the LACE study revealed a statistical tendency for superiority of cisplatin and vinorelbine (CV) compared with the other cisplatin-based doublets with vindesine, vinblastine, or etoposide. Therefore, CV-based regimens have been recommended as adjuvant chemotherapy for NSCLC (10).
In the JBR 10 trial, patients received four cycles of cisplatin at 50 mg/m2 on days 1 and 8 every four weeks and vinorelbine at 30 mg/m2 weekly (8), whereas in the ANITA trial, patients were treated with four cycles of cisplatin 100 mg/m2 on day 1 every four weeks in combination with vinorelbine at 30 mg/m2 weekly (4, 11). However, the compliance to treatment was almost the same for both trials, and only 45% of patients completed the four planned cycles of chemotherapy (4, 8). In the adjuvant setting, it is important to improve the compliance with treatment.
The split-dose administration of chemotherapy is becoming more accepted, since it makes it possible to maintain a similar dose intensity with a better toxicity profile, especially with regard to hematological and non-hematologic toxicities (nausea, vomiting and renal function) compared to conventional administration (12, 13). However, there have been no reports on the feasibility and compliance of adjuvant chemotherapy with a split-dose CV regimen administered to Japanese patients.
For this reason, we retrospectively evaluated the feasibility of a regimen including split-dose CV (cisplatin at 40 mg/m2 and vinorelbine at 25 mg/m2 on days 1 and 8 every three weeks) as adjuvant chemotherapy for Japanese patients with completely resected NSCLC.
Patients and Methods
Patients. A total of 22 consecutive patients with completely resected NSCLC were treated using adjuvant chemotherapy with split-dose CV at the National Kyushu Cancer Center between August 2008 and September 2011. The inclusion criteria were: age <75 years, pathological stage II-III, Eastern Cooperative Oncology Group (ECOG) performance status (PS) <2, no previous chemotherapy or postoperative radiation therapy, adequate bone marrow reserve (leukocyte count >4.0×109/l, hemoglobin >9.0 mg/dl, platelet count >100×109/l), hepatic function (bilirubin level <1.5 mg/dl), and renal function (creatinine level <1.5 mg/dl), and the exclusion criteria were: a concomitant malignancy, serious complications, such as active infectious disease, and serious heart disease.
Treatment. Patients received four cycles of adjuvant chemotherapy with cisplatin and vinorelbine every three weeks. Cisplatin was administered intravenously at a split dose of 40 mg/m2 over the course of 120 min on days 1 and 8. Vinorelbine was administered intravenously at a split dose of 25 mg/m2 over the course of 5 min on the same days as cisplatin. A total of 1,500 ml of normal saline solution were given intravenously on days 1 and 8. In addition, 1,000 ml of normal saline solution were given intravenously on days 2, 3, 9 and 10. Patients were pre-medicated with dexamethasone and 5-hydroxytryptamine-3 receptor antagonists for anti-emetic prophylaxis, according to the American Society of Clinical Oncology guidelines (14). The prophylactic use of granulocyte colony-stimulating factor (G-CSF) was not permitted. However, G-CSF was used when patients with febrile neutropenia or grade 4 neutropenia were observed. Dose reduction of cisplatin and/or vinorelbine in subsequent cycles were based on observed toxicities. When grade 3 or higher non-hematological toxicity or grade 4 hematological toxicity appeared, the first dose reduction of cisplatin and vinorelbine in the subsequent course was to cisplatin at 30 mg/m2 and vinorelbine at 20 mg/m2, and the second dose reduction was to cisplatin at 30 mg/m2 and vinorelbine at 15 mg/m2. If further dose reduction was required, the treatment was discontinued.
Evaluation criteria. The patients were evaluated based on their medical history, physical examination, assessment of PS, adverse events, treatment compliance and relapse-free survival. Hematological and non-hematological toxicities were assessed using the National Cancer Institute, Common Terminology Criteria for Adverse Events, version 4.0 (NCI-CTCAE version 4.0) (15).
Statistical analysis. The overall survival (OS) was measured from the day of surgery to the day of death or last follow-up. Progression-free survival (PFS) was defined as the time between the day of surgery and the diagnosis of recurrence or the last follow-up. The survival curves were made using the Kaplan–Meier method.
Results
Patients. A total of 22 consecutive patients received adjuvant chemotherapy with split-dose CV at the Kyushu Cancer Center between August 2008 and September 2011. Twelve patients (55%) were males and 10 (45%) were females. The median patient age was 67 (range 50-76) years. Twenty-one patients (95%) had an ECOG PS of 0, and one patient had a PS of 1 (5%). Most patients had undergone a lobectomy, and 12 out of 22 patients had pathological stage IIIA disease. The patients' characteristics are summarized in Table I.
Patients' characteristics.
Toxicity. All patients were evaluated for toxicity (Table II). All observed toxicities were mild. The grade 3 or 4 adverse events observed in the patients were: neutropenia in 17 patients (68%), anemia in two patients (9%), febrile neutropenia in two patients (9%) and elevation of alanine aminotranferase in one patient (5%). No severe non-hematological toxicities were observed. There were no treatment-related deaths.
Dose administration. All four planned cycles were completed in 17 out of the 22 patients (77%). The treatment was discontinued in 5 out of the 22 patients (23%); it was discontinued after one course of chemotherapy due to grade 2 creatinine decrease in one patient, and discontinued because two dose reductions were needed in three patients, and due to progression of cervical spondylosis owing to chemotherapy in one patient after three cycles (Table III). A dose reduction was required because of the development of adverse events in 11 patients. The reasons for dose reduction were grade 4 neutropenia in nine patients and grade 3 febrile neutropenia in two patients. The delivered dose intensity and relative dose intensity were 285 mg/m2 for cisplatin and 177 mg/m2 for vinorelbine. The relative dose intensity was 89% for both cisplatin and vinorelbine (Table IV).
Hematological and non-hematological toxicity in study of cisplatin plus vinorelbine as adjuvant chemotherapy.
Number of cycles and the treatment completion rate in study of cisplatin plus vinorelbine as adjuvant chemotherapy.
Dose administration of in study of cisplatin plus vinorelbine as adjuvant chemotherapy.
Efficacy. The Kaplan-Meier curves for OS and PFS are shown in Figure 1. The median PFS was 39.5 months (95% CI=32.9-46.1 months). The median OS had not been reached as at the writing of this artcle.
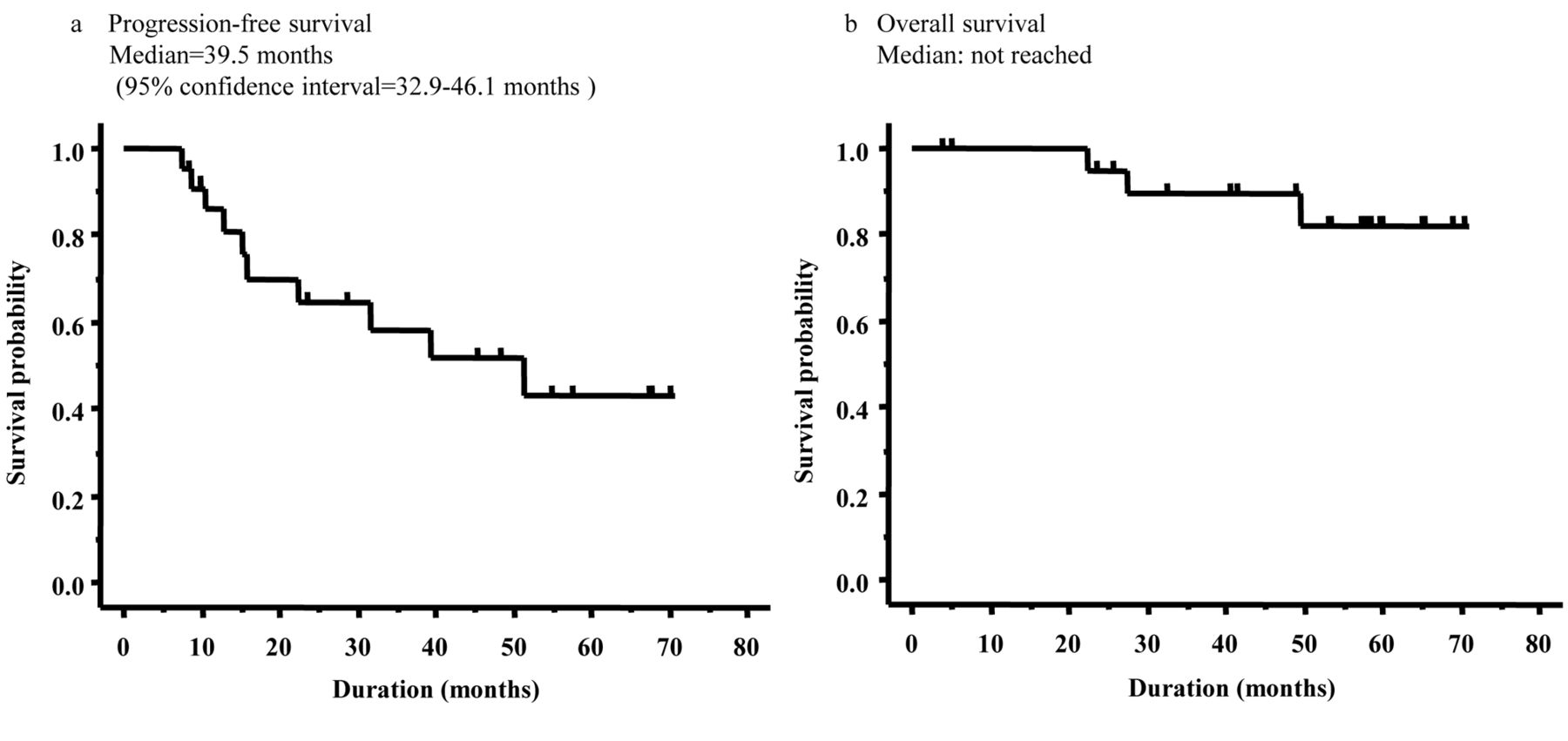
Kaplan-Meier curve showing (a) overall survival and (b) progression-free survival for patients who received adjuvant chemotherapy with split-dose of cisplatin and vinorelbine (n=22).
Discussion
The LACE meta-analysis showed a 5-year survival benefit of 5.4% with cisplatin-based adjuvant chemotherapy (6). A sub-group analysis for the CV regimen indicated that it provided a superior survival benefit compared to other cisplatin-based regimens (5). In the ANITA trial, cisplatin at a dose of 100 mg/m2 was administered on day 1 and vinorelbine at 30 mg/m2 was administered on days 1, 8, 15 and 22 every four weeks, and each four-week treatment schedule was designated as one cycle. On the other hand, in the JBR-10 trial, cisplatin at 50 mg/m2 on days 1 and 8 and vinorelbine at 30 mg/m2 was administered on days 1, 8, 15 and 22 every four weeks, and each four-week treatment schedule was designated as one cycle. However, the completion rates of the planned full doses of adjuvant therapy with CV were low in these trials, only 48% in the JBR-10 and about 50% in the ANITA trial. Moreover, treatment-related deaths were observed in both trials, 2% in the ANITA trial and 0.8% in the JBR-10 trial. Therefore, we planned treatment using split-dose CV (split administration of cisplatin 40 mg/m2 and vinorelbine 25 mg/m2 on days 1 and 8, every three weeks) to reduce the appearance of adverse events and to increase the compliance for adjuvant chemotherapy in Japanese patients with NSCLC.
The hematological toxicity in the present study was similar to that in the ANITA and JBR-10 studies. Shukuya and others reported the safety and compliance of adjuvant chemotherapy with non-split cisplatin and vinorelbine in Japanese patients with NSCLC (16). The hematological toxicity was almost the same in the present study as was reported in that trial. On the other hand, the non-hematological toxicity tended to be lower than those reported in several previous trials. Therefore, split-dose CV might be more feasible for adjuvant chemotherapy in Japanese patients with NSCLC.
Although the recommended dose of cisplatin is controversial, the LACE trial reported a favorable prognosis in a subset analysis of patients who received 300 mg of cisplatin (5). The planned total cisplatin dose was 400 mg/m2 in both the ANITA trial and JBR-10 trials. The median dose that patients actually received was 304 mg/m2 in the ANITA trial and 302 mg/m2 in the JBR-10 trial. In the present study, the planned dose of cisplatin was 320 mg/m2 and the actual dose administered was 285 mg/m2. Although the treatment completion rate of 77% in this study was higher than those in previous trials (ANITA 49%, JBR-10 48%), the actual dose of cisplatin in this trial was less than in other trials [ANITA, JBR-10, and another Japanese trial (16)].
This treatment requires hospitalization because of the need for hydration before cisplatin administration on days 1-3 and 8-11. However, patients tend to prefer to be treated as out-patients. Therefore, this treatment may be improved by shortening the hydration.
In conclusion, the split-dose CV regimen was a feasible and well-tolerated treatment, especially concerning non-hematological toxicity, as adjuvant chemotherapy for Japanese patients with completely resected primary NSCLC. However, we recommend adjuvant chemotherapy with non-split cisplatin and vinorelbine in Japanese patients with NSCLC, because of the lower actual dose of cisplatin and the absence of need for hospitalization.
- Received December 8, 2013.
- Revision received December 24, 2013.
- Accepted December 27, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.