


Abstract
Aim: To investigate the expression of platelet-derived growth factor (PDGF) receptor-A (PDGFRα), epidermal growth factor receptor (EGFR) and c-Met in spinal chordoma. To the authors' knowledge, little is known regarding the prognostic significance of receptor tyrosine kinase in spinal chordoma. Materials and Methods: Using immunohistochemical techniques, the authors investigated PDGFR-α, EGFR and c-MET expression in 52 primary and 104 recurrent lesions, and compared these data with clinicopathological parameters. Results: PDGFR-α, EGFR and c-MET were found to be expressed in 75.0%, 83% and 77% of primary, and in 97.0% of recurrent lesions in all investigated receptor tyrosine kinases. Higher PDGFR-α and c-MET expression was found to be correlated with younger patient age. Lesions with a higher expression of PDGFR-α demonstrated significantly higher EGFR scores in both primary and recurrent lesions compared to those with lower PDGFR-α expression. In recurrent lesions, higher c-MET expression was found to be associated with significantly better prognosis than those with lower c-MET expression (p=0.033). Lesions with a higher level of PDGFR-α expression were found to have significantly poorer prognosis than those with lower PDGFR-α expression (p=0.024). Those patients with lower EGFR expression were found to have significantly better prognosis than those with higher EGFR expression (p=0.005). Conclusion: In the current study, c-MET expression in patients with spinal chordoma was found to be correlated with a younger patient age and a favorable prognosis. Patients with a higher level of PDGFR-α and EGFR expression were found to have a significantly poorer prognosis than those with lower PDGFR-α and EGFR expression.
Chordomas are rare, slow-growing neoplasms of the axial skeleton that occur along the spine and comprise 1%-4% of all bone tumors (1). They are thought to originate from notochordal remnants. Chordomas can occur at any age, but especially between 40 and 60 years of age. They arise from the sacrococcygeal region in approximately 50%, from the sphenooccipital area in 35% and from the spine in 15% of cases (2). Locally, these tumors are highly aggressive and frequently demonstrate local recurrence even after wide resection (3). Due to the rarity of these tumors, current understanding of molecular marker expression in chordomas is limited. One important cell-signaling pathway in cancer progression involves a class of molecules known as receptor tyrosine kinases (RTKs).
A small amount of information is available on RTK activation, but their RTK expression could offer useful alternative therapeutic targets, as no effective chemotherapeutic regimens are available for the treatment of chordomas, surgery remains the mainstay of chordoma management (4). Differential expressions of c-Met and EGFR in a wide variety of other tumors have been shown previously (5). As only investigated in a small cohort of 12 chordomas, it appears important to investigate the expression of these receptors in a higher number of chordomas for meaningful conclusions. Therefore, in the present study, we decided to focus our investigations on the expression of RTK (EGFR, c-Met and PDGFR-α) in a cohort of 52 spinal chordoma patients.
Materials and Methods
Chordomas. A series of 52 chordoma patients with a total of 156 lesions (including 104 recurrent lesions), who underwent surgery between 1986 and 2007 at the neurosurgical Departments of the Nordstadt Hospital and of Hannover Medical School, Germany, were considered for the present analysis. Twelve out of 52 patients underwent surgery from 2008 to 2011 at the Mashhad University Medical Center in Mashhad, Iran. Tumor recurrence was defined as a return of symptoms and signs, with radiological verification of tumor re-growth (Table I). All patients were included in the study and there were no exclusion criteria other than lack of available material for immunohistochemical analysis. Clinical data were extracted from the two institutional surgical databases. The data obtained at presentation included: sex, age at diagnosis, tumor site, tumor size, primary versus recurrent chordoma, chordoma subtype, c-Met, EGFR and PDGFR-α expression, margin status, adjuvant radiotherapy has been administrated (yes/no, dose in Gray). Before surgery, all patients underwent staging based on computed tomography (CT) scan (Table II).
Cohort demographics. The patients (20 women and 32 men) ranged in age from 17 to 87 years (median=57 years). All patients experienced recurrence and subsequent resection. Locations of chordomas were sacral (n=36), lumbar spine (n=13) and cervical/thoracic spine (n=3).
Multi-tumor tissue microarray construction. A multi-tumor tissue microarray was assembled and used for comparison of molecular marker expression of chordomas. Following Institutional review board approval, we constructed the tissue microarrays, as previously described (6). The tissue microarrays (TMA) were constructed using a tissue arraying instrument (Beecher Instruments, Hackensack, NJ, USA). Three tissue core cylinders with a diameter of 0.6 mm were punched from each donor paraffin block in targeted areas corresponding to previously-demarcated neoplastic areas on the parallel slide. These tissue cores were then deposited into a recipient “master” paraffin block. The punches were placed 1 mm apart on the x-axis and 1.5 mm apart on the y-axis.
Two microarray blocks contained 76 and 80 punches, respectively. Sections 5-μm thick were cut from the master block, stained with H&E, and reviewed to ensure the presence of morphologically-pure cores of chordoma for each case. Morphological features of each core were confirmed by reviewing the corresponding whole-tissue sections stained with H&E. We obtained tissue cores from paraffin-embedded formalin-fixed tissue blocks from the archives at the Department of Pathology, Nordstadt Medical Center, Klinikum Hannover, Germany. A pathologist (H.O.) reviewed slides from all blocks to select representative areas of invasive tumor or normal tissue to be scored. The chordoma subtype (conventional, chondroid, dedifferentiated) was indicated.
Immunohistochemistry. All slides were processed simultaneously under identical conditions using standard methods. Immunohistochemistry was performed on the 156 lesions for the following antibodies: EGFR (1:20, Rabbit Polyclonal Antibody, Dunn, Asbach, Germany), PDGFR-α (1:100, Rabbit Polyclonal Antibody, Lab Vision, Suffolk, UK), c-Met (1:500, Rabbit Polyclonal Antibody, Santa Cruz Biotechnology, Heidelberg, Germany) and CD-34 (1:30, Mouse Monoclonal Antibody, Abcam PlC, Cambridge, UK). The sections were treated with antigen retrieval. Then they were treated with a primary antibody, followed by staining with an avidin-biotin-peroxidase complex (Immunotech, Marseille, France) or an alkaline phosphatase detection kit (Vector, Burlingame, CA), according to standard immunohistochemical techniques (7). All slides were run simultaneously under identical conditions and negative control slides were included. Positive and negative control sections were included for each antibody and slide pre-treatment, respectively. TMA slides in which incubation with primary antibody was omitted served as the negative controls for each antigen retrieval regimen.
Sixty-seven lesions were documented as first; 25 as second and 12 as third recurrences.
Immunohistochemical scoring for EGFR, PDGFR-α, c-Met and CD-34. Immunoreactivity was evaluated independently by two pathologists who had no prior knowledge of the clinical data or other histological findings. Immunoreactivity was scored as described elswhere (7, 8). Every tumor was given a score according to the intensity of the nuclear or cytoplasmic staining (no staining=0, weak staining=1, moderate staining=2, strong staining=3) and the extent of stained cells (0=none; 1=less than 25%; 2=25-50%; and 3=more than 50%). We determined the sum of these 2 parameters to evaluate the expression of antibodies used in this study, on a scale from 0 to 6. The cells were graded as negative when they showed a complete absence of staining (score 0), weak staining (score 1), moderate staining (score 2), originating from baseline expression. The scores 3-6 were regarded as strongly-positive. Structures were only counted as microvessels if they stained positively with the vascular marker and appeared vascular morphologically. Expression of CD34 was used to detect microvessels.
Light microscopy. Nuclear pleomorphism, intra-tumoral necrosis, and intra-tumoral bleeding were evaluated as positive or negative. As reported, mitosis (9-14) and apoptosis (12-14) were scarce. Therefore, we also assessed them as positive or negative instead of calculating mitotic or apoptotic indices.
Statistical analysis. We evaluated correlation of marker expression by the Spearman rank correlation test. All calculations and analyses were performed with SPSS 18.0 for Windows. Significance was set at p<0.05.
Results
Histopathology and immunohistochemistry. The histological hallmark of chordoma are large tumor cells with abundant vacuolated cytoplasm, referred to as physaliphorous cells. All chordomas in our cohort were reviewed and classified as conventional (n=47) (90.3%), chondroid (n=3) (5.7%) and de-differentiated (n=2) (3.8%) chordomas by means of morphology and immunohistochemistry. They show prominent lobules separated by fibrous septa. The tumor cells are arranged in cords or sheets or may be floating singly in the often present abundant myxoid matrix.
Patients' characteristics at first observation with clinical and histopathological features (n=52).
EGFR. Chordomas displayed predominantly strong expression of EGFR with intense and diffuse cytoplasm membrane positivity. Immunoreactivity tended to concentrate at the tumor periphery but in several cases also appeared homogeneous over a certain tumor area. The EGFR immunopositivity in primary chordoma was found in all cases, showing different levels of reactivity. There were 10 tumor lesions with moderate (score 2) (19.2%) and 42 with strong expression (score3-6) (80.7%) (Figure 1).
CD34. Primary chordomas displayed predominately mild expression of CD34. Mild expression (score 1) was detected in 26 primary lesions (50%), moderate expression (score 2) in 17 (32.6%) lesions. A strong expression (score 3-6) could not be detected among primary chordomas. CD34 immunoreactivity was confined to endothelial cells and scattered single-positive cells in 40% of the tumor stroma. Over 11% of recurrent lesions had a high immunoreactivity for CD34 (Figure 2). There was a slight increase in expression of CD34 among the first to the third recurrences.
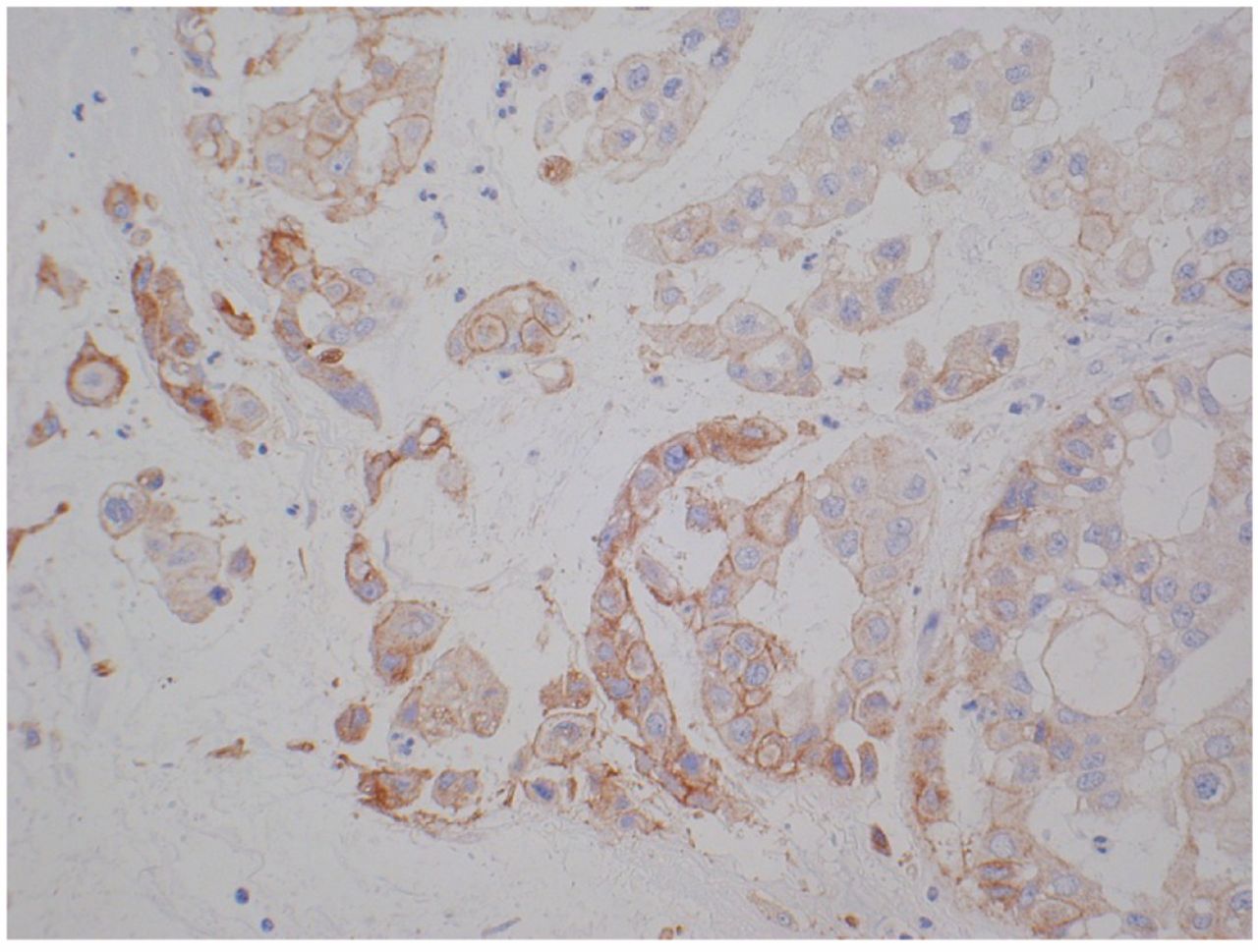
PDGFR-α and c-Met. All cases of primary chordoma were positive for PDGFR-α and all showed moderate (score 2) (n=6, 11.5%)-to-strong (score 3-6) (n=46, 88.4%) staining (Figure 3). C-Met were also positive in all primary chordomas and showed moderate (score 2) (n=15, 28.8%)-to-strong (score 3-6) (n=29, 55.7%) staining (Figure 4). Chordoma cells were presented with intense and diffuse cytoplasm membrane positivity.
Relationship between expression of EGFR, PDGFR-α, c-Met and clinicopathological factors. A relationship between EGFR expression, PDGFR-α and c-Met was detected. There was a significant correlation between EGFR and PDGFR-α expression levels (p=0.0265, Spearman ρ=0.2573). The expression pattern of primary and recurrent spinal chordomas are summarized in (Figure 5, Figure 6). EGFR and C-Met expression was significantly higher in the older than in the younger patient group. Men showed higher expression of EGFR and PDGFR-α than women; the difference for EGFR was statistically significant. A significant correlation between EGFR, PDGFR-α and CD-34 expression and clinical symptoms could not be observed (Table II).
Clear EGFR, PDGFR-α, c-Met and CD-34 expression differences have been noted between primary and recurrent spinal chordoma. No correlations were seen between site of primary tumor, age and sex.

Chordoma and overexpression of EGFR (score 6). Immunohistochemistry with anti-EGFR antibody showing strong membranous and cytoplasmic staining of tumor cells (original magnification, ×200; positivity appears in brown).
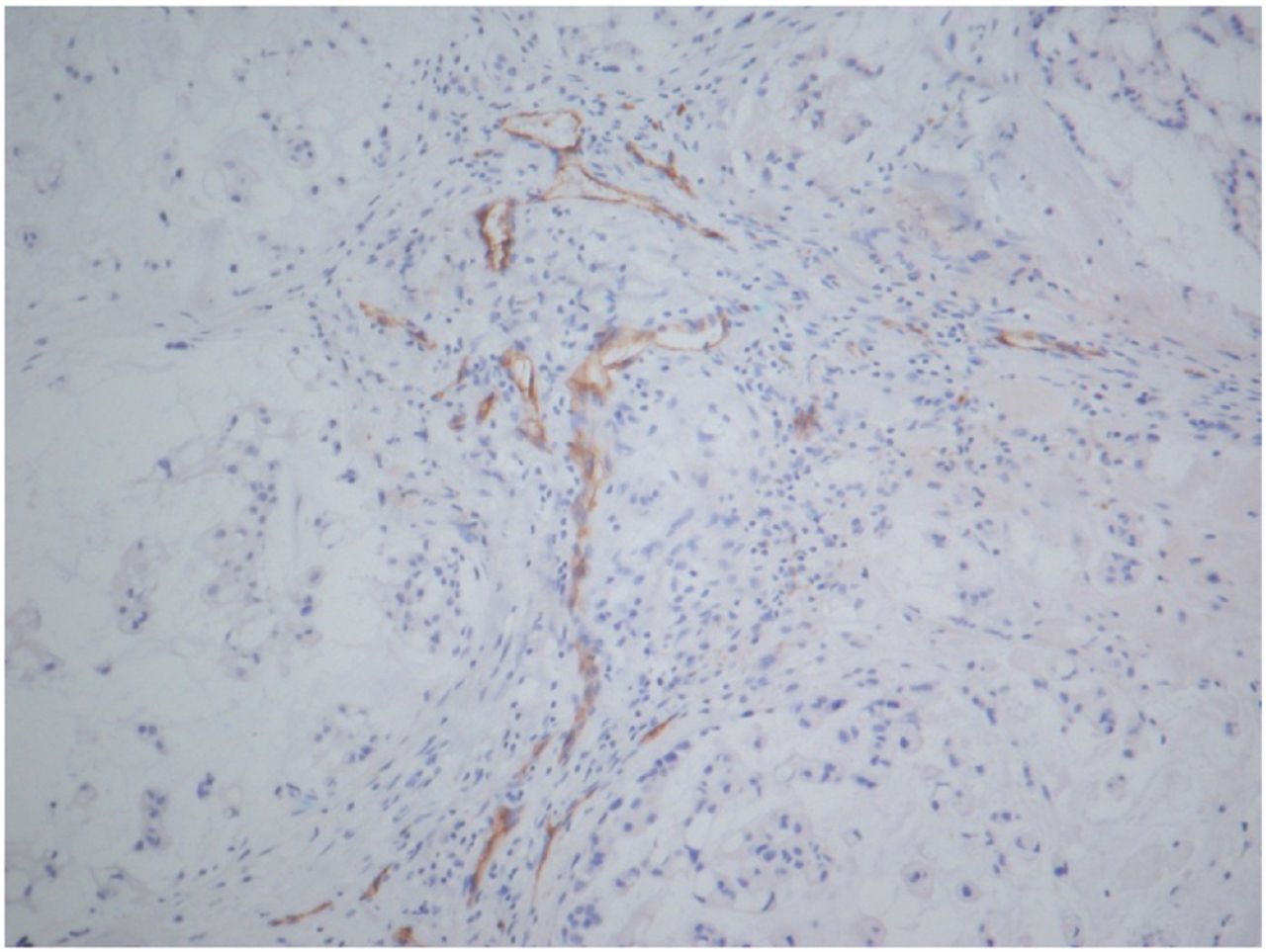
Immunohistochemical staining of spinal chordoma tissues with CD34 antibodies. The endothelial cells of vessels are stained positively (brown). CD34 mild staining (score 1) (original magnification, ×200).
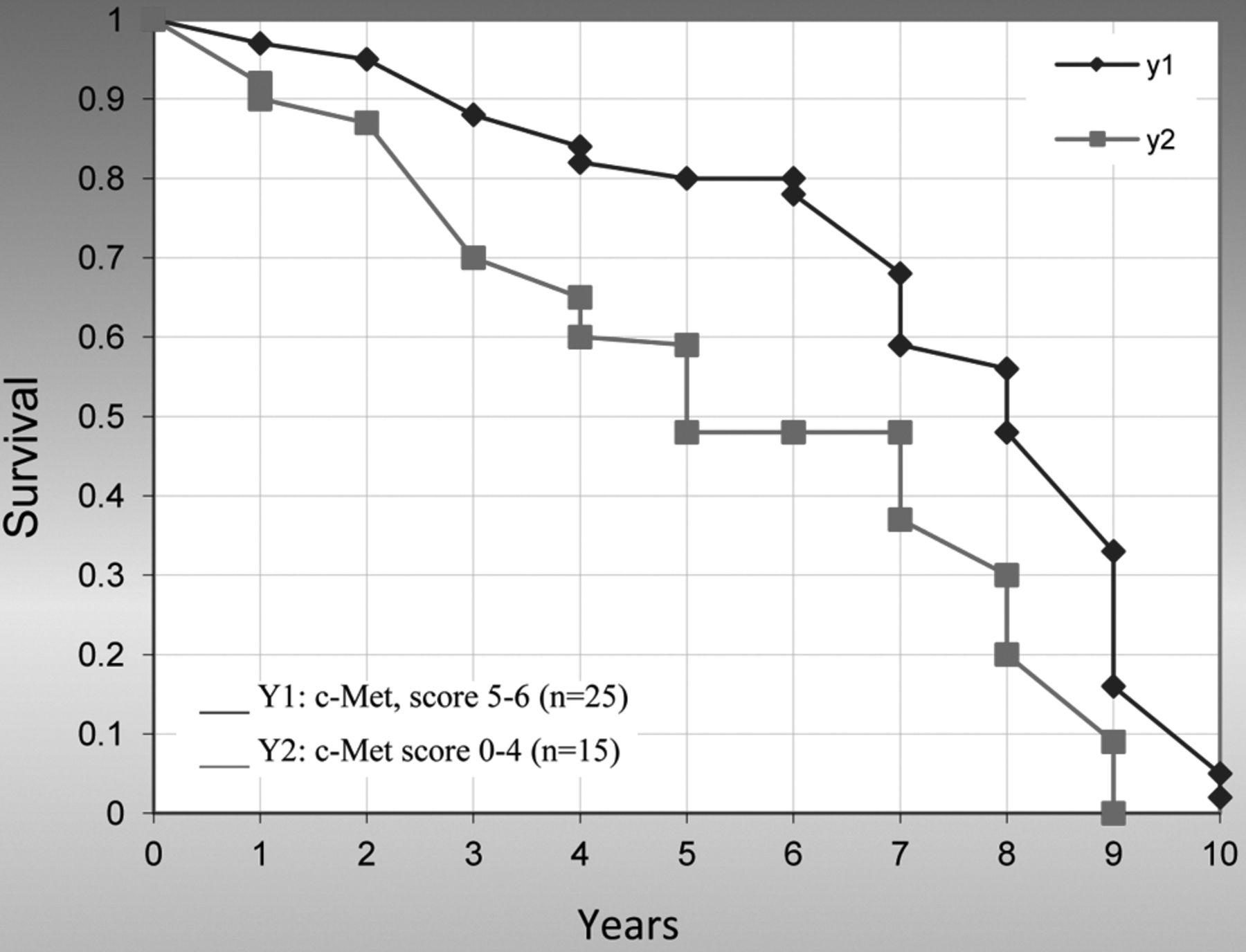
Prognosis. Follow-up ranged from 3 to 10 years after initial surgery. Detailed follow-up data were available for 40 patients, the Kaplan-Meier survival curve was used for calculating survival rates. Patients with higher levels of c-Met expression (score 5 or 6) were found to have a significantly better prognosis than those with lower c-Met expression (score 0-4) (p=0.033) (Figure 7).
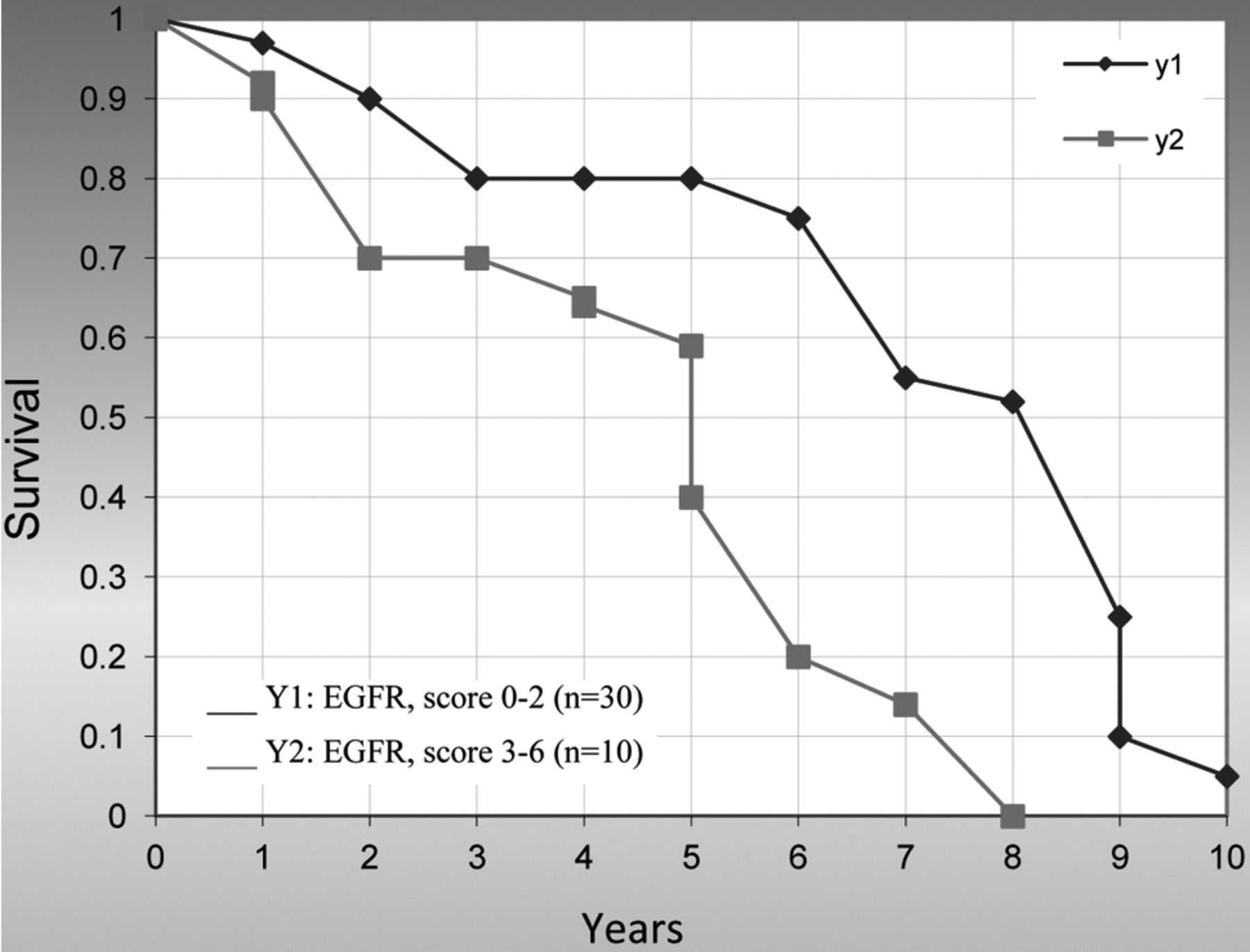
Overall survival in patients with a positive reaction (score 5-6) for PDGFR-α expression was significantly poorer at 10 years (p=0.024) (Figure 8), as well as patients with higher (score 4-6) EGFR expression (p=0.005) (Figure 9).

Histopathological features of primary spinal chordoma with strong PDGFR-α (score 6) staining. Physaliferous cells and round-to-oval nuclei can be detected.

Syncytial arrangements of tumor cells in the form of cords and expression of c-Met (score 6) in spinal chordomas.
Discussion
The aim of the present study was to explore the immunhistochemical expression of PDGFR-α, EGFR and c-Met as potential therapeutic targets; we performed this analysis in a series of 156 spinal chordoma lesions for which formalin-fixed surgical material was available.
Chordomas are rare, low-grade, primary malignant bone tumors arising from primitive notochordal remnants in the midline skeletal axis. Their incidence rate is less than 0.1 per 100,000 persons per year (15). Complete surgical removal still remains the cornerstone of chordoma treatment even though safe margins are often hard to achieve because of the anatomical location. Conventional radiotherapy with high-energy photons may offer some temporary disease control benefit in patients with incomplete surgery or, as exclusive treatment, in patients with unresectable/inoperable disease (16). Proton radiotherapy may succeed in offering better tumor control and produce fewer side-effects, even if it is still not as readily-available as external-beam radiotherapy (17).

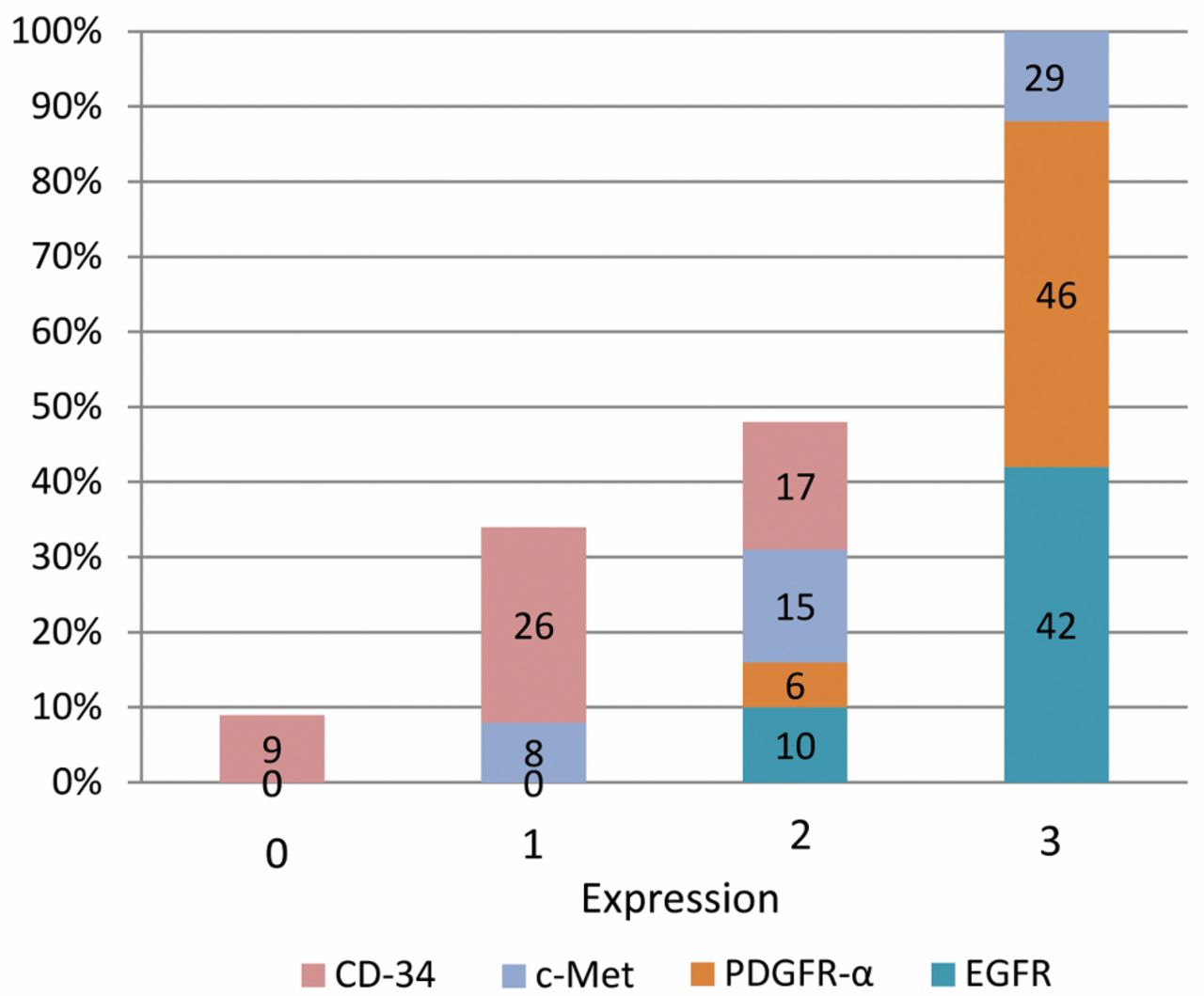
Expression of PDGFR-α, EGFR, c-Met and CD-34 in primary chordoma (n=52). PDGFR-α and EGFR expression are noted to be primarily strong. CD-34 expression showed predominantly slight-to-moderate expression. The c-Met expression in primary chordoma was variable from mild-to-strong expression.
Chordomas respond poorly to chemotherapy, as generally reported in the small sub-group of patients with high-grade de-differentiated chordomas with agents active in high-grade sarcomas (18). There is no standard systemic therapy which could support surgical and radiotherapeutic protocols for treatment of advanced chordoma (19).
Recent studies have concentrated on molecular-targeted agents, giving rise to new therapeutic hopes, particularly since the antitumor activity of imatinib mesylate has been shown to act as an anti-PDGFR drug both in vitro and in patients with chordoma (20-22). Some patients with chordoma have been reported to benefit from a therapy with EGFR inhibitors (23, 24). Clinical benefits and objective tumor regression were observed in all patients using anti-EGFR treatment, even in those with a long delay between initial diagnosis and drugs administration. The largest series analyzed to date (173 clinical samples) (25) and our series with 156 samples confirmed frequent EGFR expression in 69% and 95% of the cases. Therefore, targeting EGFR might be an attractive alternative in the treatment of chordoma. Weinberger et al. (5) collected a cohort of 12 chordomas and examined the expression of hepatocyte growth factor/scatter factor receptor (c-Met), HER2/neu and EGFR and compared these with 17 other malignancies. The immunohistochemical analyses revealed predominantly strong expression of EGFR (strong 50%, moderate 33%, weak 17% EGFR expression), and c-Met (strong 58%, moderate 17%, weak 8% c-Met expression). The authors state that chordomas, like many other solid tumors, express EGFR and c-Met and show strong expression of both EGFR and c-Met (13, 14).
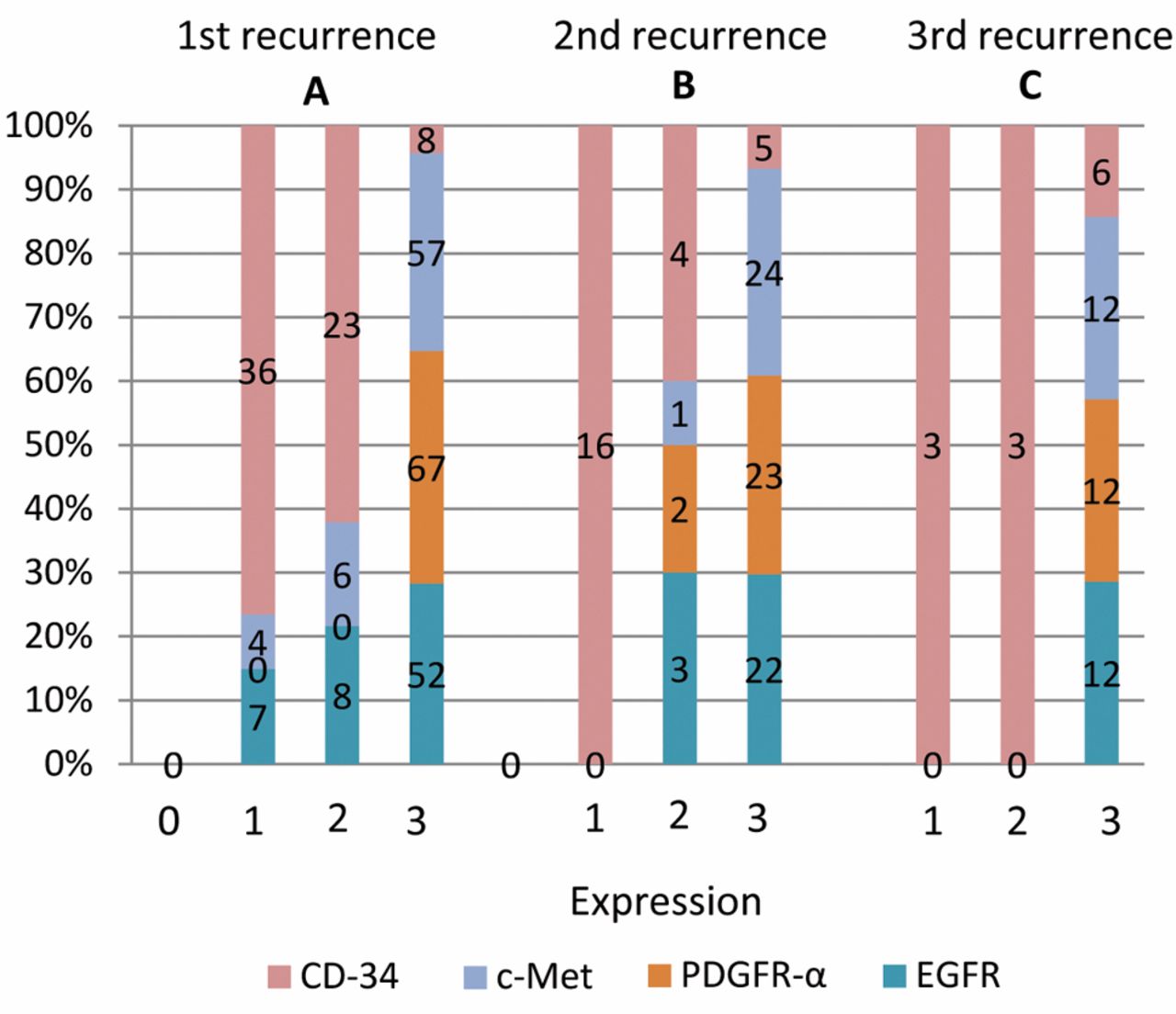
Expression pattern of first (n=67), second (n=25) and third (n=12) recurrence of spinal chordomas as summarized in Figure 5. There was a slight increase in expression of PDGFR-α, EGFR, c-Met and CD34 among the first to the fourth recurrences. A) 1st recurrence (n=67); B) 2nd recurrence (n=25); C) 3rd recurrence (n=12).
In 2008, Fasig et al. (26) published results of their immunohistochemical analysis of RTK signal transduction activity in 21 cases of chordoma. PDGFR-α and EGFR were detected in 100% and 67% of cases, respectively. The authors did not observe statistically significant correlations between the expression of any of the markers studied and disease-free survival or tumor location. In our series, with a large number of 156 samples, 95.2% of cases were evaluated immunohistochemically as positive and 4.8% as negative for EGFR expression. We also found a significant and strong correlation between c-Met and EGFR expression. According to our data, the other RTKs which are highly expressed in spinal chordomas are PDGFR-α and c-Met.
C-Met expression and clinicopathological findings. C-Met is thought to play a role in the early stages of neoplastic promotion. C-Met expression was frequently noted in well-differentiated tumor types; in addition, c-Met expression was found to be inversely correlated with vascular or perineural (27) invasion and metastasis (27, 28) in these tumors. Furthermore, patients with c-Met-positive lesions were found to have a more favorable prognosis than those with c-Met-negative lesions in some cancers (28-31).

Kaplan-Meier curve for the overall survival of patients with expression of c-Met. The 10-year survival rate for patients with a higher level of c-MET expression was found to be significantly better than those with lower c-MET expression (p=0.033).
In the present study, we detected a high frequency of c-Met expression. All of spinal chordoma lesions examined were positive for c-Met expression.
Naka et al. (14, 31) have also demonstrated a high c-Met expression in skull base chordoma. Considering the finding that c-Met is mainly expressed in epithelial cells (32, 33), these results indicate that skull base chordomas with greater epithelial differentiation express c-Met more strongly - or suggest that those with less epithelial differentiation have decreased c-Met expression. This might be quite similar to spinal chordoma. In addition, there was no apparent correlation between c-Met expression and PDGFR-α expression in spinal base chordoma.
Furthermore, patients with higher c-Met expression were found to have a significantly longer survival than those with lower c-Met expression. These findings indicate that the accumulation of c-Met protein does not necessarily correlate with recurrence of spinal chordoma, and a subsequent lack or loss of c-Met expression is considered to result in a more aggressive clinical behavior, leading to poor survival.
PDGFR-α expression and possible therapeutic approaches. Increasing knowledge on genetic markers of chordomas has recently led to the use of molecular-targeted therapies. The finding that chordomas display overexpression of constitutively active phosphorylated forms of PDGFR and of KIT receptors (34) prompted the use of imatinib in chordoma patients, a tyrosine-kinase inhibitor (TKI) drug with specificity for the kinase domains of these receptors. Imatinib was used with some success in clinical trials (20) alone or in combination with the immunosuppressant sirolimus (a.k.a. rapamycin) (21). It seems likely that the effects of TKI drugs may extend to other phosphorylated receptors found altered in chordomas, such as PDGFR-α (22, 23, 28). In our present study, all cases of chordoma were positive for PDGFR- α.

Survival according to the expression of PDGFR-α in spinal chordomas. Lesions with a higher level of PDGFR-α expression were found to have a significantly poorer prognosis than those with lower PDGFR-α expression (p=0.024).

Survival curves for patients with lower EGFR expression (score 0-2) were found to have a significantly better prognosis than those with higher EGFR expression (score 3-6) (p=0.005).
Altogether, these observations suggest that a small-molecule tyrosine-kinase inhibitor could very likely be sufficient in the treatment of spinal chordoma. Our findings should be viewed with caution, but for patients with few other treatment alternatives, experimental use of one of these agents may be a viable option.
Conclusion
Our study demonstrates that PDGFR-α, EGFR and c-Met are frequently-activated RTKs in spinal chordomas and may play significant roles in the growth of chordomas. Given the natural course of chordomas, any possible new treatment options deserve exploration. In light of these findings, chordoma patients may benefit from treatment with multi-kinase inhibitors targeting both EGFR and PDGFR. In addition to the PDGFR family, which is inhibited by imatinib, the presence of activated receptors of the EGFR family may provide a rationale for treating these patients.
Acknowledgements
Special thanks go to Prof. Dr. med. Dr. h. c. mult. M. Samii from the International Neuroscience Institute Hannover/Germany, Department of Neurosurgery, for providing us with a large amount of data on chordoma patients thanks to his excellent experience in skull base surgery.
- Received January 7, 2014.
- Revision received January 14, 2014.
- Accepted January 15, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Design and evaluation of novel 4-anilinoquinolines and quinazolines EGFR inhibitors in lung cancer and chordoma
- Active receptor tyrosine kinases, but not Brachyury, are sufficient to trigger chordoma in zebrafish
- Active Receptor Tyrosine Kinases, but not Brachyury, are sufficient to trigger chordoma in zebrafish
- Design of a GAK/EGFR inhibitor set to interrogate the relationship of EGFR and GAK in chordoma
- Afatinib Is a New Therapeutic Approach in Chordoma with a Unique Ability to Target EGFR and Brachyury
- PARP1 is a novel independent prognostic factor for the poor prognosis of chordoma
- Predicting Survival of Patients with Metastatic Epidural Spinal Cord Compression from Cancer of the Head-and-Neck