


Abstract
Aim: To evaluate the prognostic factors of ovarian granulosa cell tumors (GCTs) and treatment outcomes in recurrent GCT cases. Patients and Methods: We retrospectively reviewed 91 patients with GCT who were treated in two tertiary Centers between 1989 and 2011. Results: Eighty patients had stage I tumors, five had stage II, and six had stage III. There were 15 cases of recurrence with a median follow-up time of 58 (3-254) months. Multivariate analysis identified greater tumor size and postoperative residual tumor as independent risk factors for recurrence. Twelve patients underwent secondary surgery at first recurrence. At a median follow-up of 50 (4-185) months from first recurrence, the 5-year survival was 60% for patients with and 100% for those without residual tumor after secondary surgery, respectively (p=0.018, log-rank test). Conclusion: Complete cytoreduction is an important prognostic factor for recurrent cases as well as initial treatment of GCT.
Granulosa cell tumors (GCTs) of the ovary are rare sex-cord stromal lesions. GCTs account for about 5% of ovarian malignancies and are classified histologically as adult (95%) or juvenile (5%) types (1-3). Most GCTs occur in perimenopausal women who typically present with symptoms related to estrogen secretion, such as abnormal vaginal bleeding or precocious puberty (4). GCTs are usually diagnosed early and have a relatively favorable prognosis (1). However, late relapse often occurs due to an indolent disease course, and the prognosis of advanced disease is poor, with a 5-year survival rate of 0% to 20%, comparable to that for epithelial ovarian cancer (5, 6). In addition, more than 66% of recurrent GCT patients eventually die from the disease, indicating ineffective treatments and dissimilar tumor biology (1).
Prognostic factors for GCTs have been reported previously and include age, tumor size, tumor stage, tumor rupture, postoperative residual tumor, bilaterality, nuclear atypia, and high mitotic index (5-15). However, prognostic factors and clinical features of GCT recurrence remain unclear due the rarity and indolent course of the disease. Furthermore, there are few data that would facilitate optimal therapy development for recurrent GCT (16). We, thus, investigated the clinicopathological features of a large group of rare adult-type GCT in two tertiary referral Centers to further elucidate prognostic factors for recurrence and evaluate treatments.
Patients and Methods
Following approval from the Institutional Review Board at both Institutions (S2013-0588-0001, KUH1030028), all cases of adult-type GCT treated between 1989 and 2011 at the Asan Medical Center and Konkuk University Hospital in Korea were identified. Eligibility criteria included primary surgery at either Institution, as well as referral for a restaging operation from another hospital where GCT had been clearly described. Pathological diagnoses were confirmed by two pathologists specializing in gynecological oncology.
We retrospectively reviewed all available computerized and paper medical records at both institutions to obtain information on patient characteristics, clinical presentation, International Federation of Gynecology and Obstetrics (FIGO) stage, surgical procedures, tumor size, postoperative residual tumor, adjuvant treatments, recurrence patterns, management of recurrence, and last follow-up status. Tumor size was determined by preoperative ultrasonogram or computed tomography.
Exploration of the entire abdomen, including the diaphragm, liver, small bowel, rectosigmoid colon, pouch of Douglas, both paracolic gutters, and the abdominal wall, was performed in all patients. Complete surgical staging was defined when at least a unilateral salpingo-oophrectomy, pathological evaluation of the endometrium, peritoneal cytology, peritoneal biopsy, omentectomy, and pelvic and para-aortic lymphadenectomies were performed. No surgical staging was defined when only a unilateral salpingo-oophorectomy or ovarian cystectomy was performed. All other operations constituted partial surgical staging (15). To evaluate the postoperative residual tumor status in patients without complete surgical staging, we considered the patient clear of residual tumor if no gross residual tumor were found after exploration of the entire abdomen. Fertility-sparing surgery (FSS) was defined as the preservation of the uterus and at least one adnexa.
Continuous variables were assessed with Student's t-test or Mann–Whitney U-test. Categorical variables were assessed with the chi-squared or Fisher's exact tests. Disease-free survival (DFS) was calculated in months from the date of surgery to either the date of recurrence or to date of censorship. Patients were censored if they were alive at last contact or had died without disease recurrence. Survival curves were estimated with the Kaplan–Meier method and differences in survival were assessed by log-rank testing. Multivariate analyses were performed using the Cox proportional hazards regression. Receiver operating characteristic (ROC) curve analysis determined the continuous variable cutoff values for predicting recurrence using Youden's index (17). A two-sided p-value of less than 0.05 was considered to be significant. SPSS 19.0 (SPSS inc., Chicago, IL, USA) was used for statistical analysis.
Results
Clinicopathological characteristics. Ninety-one patients with adult-type GCT were identified, constituting 4.2% of all ovarian cancer cases during the study period. The clinical characteristics of these GCT patients are summarized in Table I. The median age was 42 (range=7-85) years and GCTs occurred most frequently in the fifth decade of life. The median tumor diameter was 91 (range=25-300) mm and the tumors were bilateral in five (5.5%) patients. The preoperative cancer antigen 125 (CA-125) level was >35 IU/ml in 22 (31.4%) patients. Pathologic evaluation of the endometrium was performed in 66 (72.5%) patients, revealing 16 (17.6%) cases of endometrial hyperplasia and one (1.1%) case of endometrial cancer. Twenty-one (23.1%) patients underwent laparoscopic surgery. Twenty-three (25.3%) patients had no surgical staging, 27 (29.7%) had complete staging, and 41 (45.1%) had partial staging. Ovarian cystectomy was performed in only one patient, who was pregnant. Nine patients had the initial operation at an outside hospital and were referred to either of the tertiary Centers for re-staging surgery. Only one of these patients was subsequently up-staged because of omental involvement. Twenty-seven patients underwent an initial systemic pelvic or para-aortic lymphadenectomy, and the median number of harvested nodes was 29 (range=3-71). No nodal metastases were detected in these patients.
Eighty patients had stage I disease, five stage II, and six stage III. Three stage II cases had gross extraovarian disease with cul-de-sac nodule involvement. The remaining two patients with stage II disease had rectal and sigmoid colon serosal adhesions microscopically diagnosed with tumor involvement. Four patients with stage III disease without nodal dissection had grossly-advanced abdominal disease and two with node dissection had grossly advanced omental disease without nodal involvement. Postoperative adjuvant chemotherapy was administered in 22 cases, with the majority of patients (n=18) receiving bleomycin, etoposide, and cisplatin (BEP), as described previously (18). All patients with stage III GCT received adjuvant chemotherapy. As this was a retrospective study, the precise indications for adjuvant chemotherapy in patients with stage I-II GCT are unclear. Attending physicians made a decision to administer adjuvant chemotherapy to patients with stage I–II GCT after discussion with the patients.
Clinicopathological characteristics of patients with granulosa cell tumor in the present study.
Univariate and multivariate Cox proportional hazard regression analyses of prognostic factors for granulosa cell tumor recurrence.
Survival analysis. Disease in 15 patients recurred with a median follow-up time of 58 (range =3-254) months, with five subsequent deaths. The 5-year DFS rate of stage I vs. II-III was 85% and 58%, respectively (p=0.039, log-rank test) (Figure 1A). By univariate analysis, International Federation of Gynecology and Obstetrics (FIGO) stage (p=0.05), postoperative residual tumor (p<0.001), and tumor size (p=0.006) were significantly associated with DFS (Table II) but not with age, preoperative CA-125 level, surgical approach, surgical staging, pelvic/para-aortic lymphadenectomy, FSS, cytology, and intraoperative tumor rupture. By multivariate analysis, postoperative residual tumor (p<0.001) and tumor size (p<0.05) remained significant prognostic predictors of recurrence (Table II).

Kaplan–Meier plots of disease-free survival outcomes for the 91 patients with granulosa cell tumor in the study series who were classified according to stage (A), tumor size (B), and the presence of a postoperative residual tumor (C). There were statistically significant survival differences between the three groups (p=0.039, p=0.001, and p<0.001, respectively, log-rank test). D: Kaplan–Meier plots of the overall survival outcomes from the date of first relapse in patients with recurrence stratified by the presence or absence of a postoperative residual tumor after secondary surgery. A statistically significant improvement in survival for patients with no residual tumor after secondary surgery was evident (p=0.018, log-rank test).
ROC analysis was used to determine the cut-off values for the tumor size that predicted recurrence. The area under the ROC plot for discriminating recurrence using a cut-off value of 120 mm was 0.674 (sensitivity=60.0%, specificity=74.3%). Kaplan–Meier curves for the DFS of patients according to tumor size and postoperative residual tumor are presented in Figures 1B and C, respectively. There were statistically significant survival differences between groups categorized by tumor size and postoperative residual tumor (p=0.001, and p<0.001, respectively, by log-rank test).
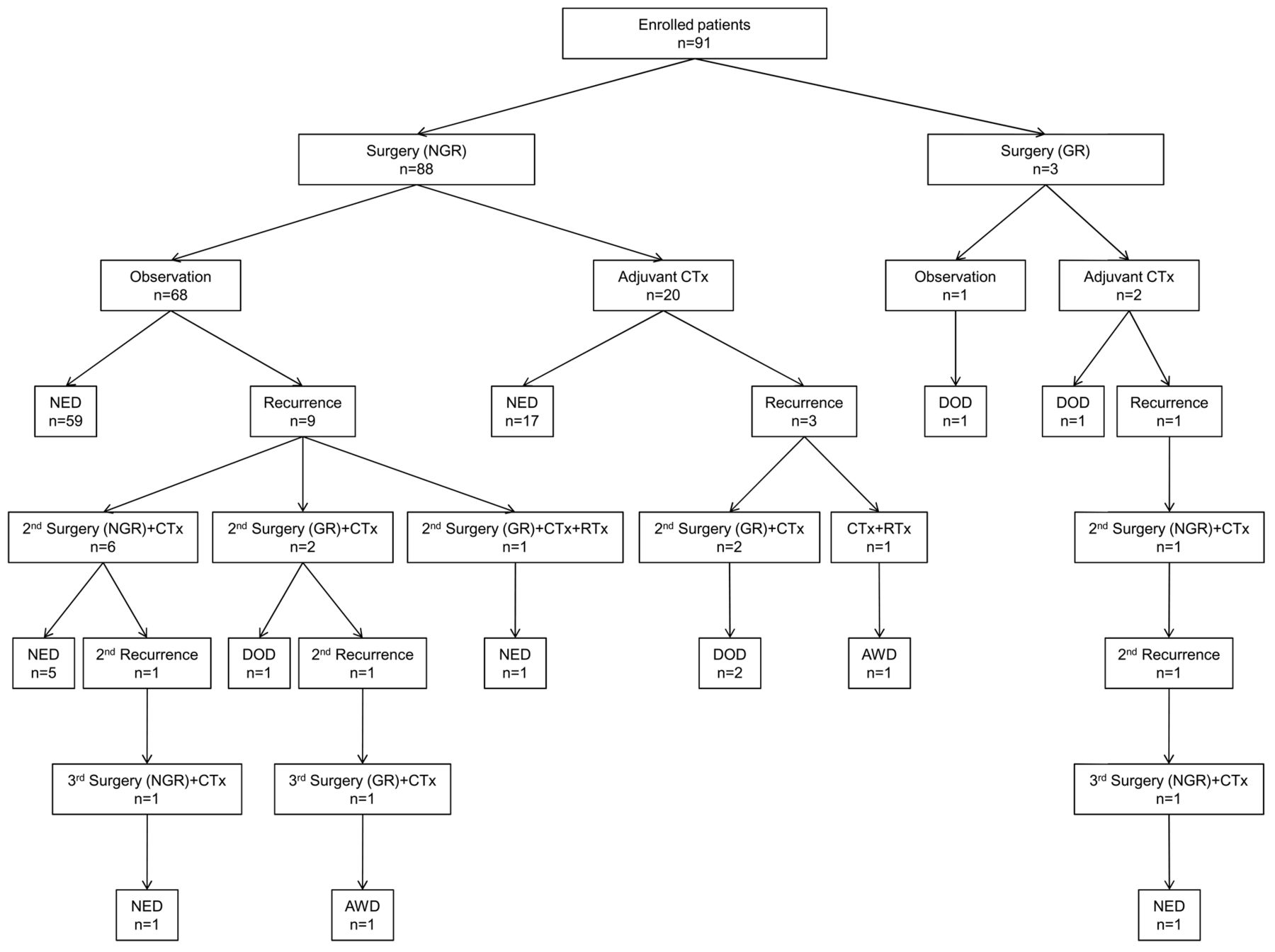
Flow chart illustrating patient management and outcomes. NGR, No gross residual disease; GR, gross residual disease; CTx, chemotherapy; RTx, radiotherapy; NED, no evidence of disease; DOD, dead of disease; AWD, alive with disease.
Among 30 cases with FSS, nine patients underwent laparoscopic surgery. Twenty-nine underwent unilateral salpingo-oophorectomy and only one underwent cystectomy. Twenty-two underwent endometrial evaluation. A total of five recurrences took place at 9, 12, 42, 74, and 97 months after initial surgery.
Treatment outcomes in relapsed patients. Disease in 11 out of the 80 stage I cases recurred with a median time of 42 (range=12-97) months. Four of the 11 patients with stage II-III disease relapsed with a median time of 21 (range=1-34) months. Peritoneal disease (n=12) was the most frequent type of recurrence. The specific sites of recurrence were as follows: two pelvic; eight pelvic-plus-abdominal; one bone; one pelvic-plus-lung; one pelvic-plus-abdominal-plus-bone and lung; one lymph-nodal; and one pelvic-plus-lymphnodal. The distribution of recurrence sites did not differ between patients with and those without a lymphadenectomy at initial surgery. Retroperitoneal lymph node recurrence was found in two cases, one with a lymphadenectomy during the primary surgery.
All patients with recurrence received chemotherapy. Treatment at the first relapse were as follows: elevan surgery-plus-chemotherapy, one surgery-plus-chemotherapy and radiotherapy; and one chemotherapy-plus-radiotherapy (Table III). For complete resection, four patients underwent extensive surgery, including right hemicoloectomy, low anterior resection, small bowel resection, and partial hepatectomy. At a median follow-up from the first relapse of 50 (range=4-185) months, the 5-year survival from the first relapse was 60% and 100% in patients with or without residual tumors after secondary surgery, respectively, revealing a statistically significant improvement in survival with no residual tumor after secondary surgery (p=0.018, log-rank test) (Figure 1D). All patients (n=11) who underwent secondary surgery received adjunctive platinum-based chemotherapy. All patients (n=7) without residual tumors after secondary surgery remain disease-free to date. Three patients developed a second relapse with a median time of 58 months from the first recurrence (range=42-70 months) and underwent tertiary surgery followed by chemotherapy. All of them had no residual disease after tertiary surgery and remain alive. At the last follow-up, eight patients were disease-free, two were alive with disease, and five had died (Figure 2).
Brief description of each patient in the study series with disease recurrence.
Discussion
The clinical characteristics, optimal therapeutic plans, and prognostic factors for GCTs remain elusive because of their relative rarity, indolent course, and long follow-up requirements. In the present study of 91 GCT cases treated over 20 years, we assessed clinical characteristics and prognostic factors for recurrence, and present a comprehensive summary of our experiences in the management of recurrent GCTs.
Stage, tumor size, and postoperative residual disease were revealed to have prognostic significance in our patients. Although several prognostic factors, including age, FIGO stage, postoperative residual tumor, tumor size, nuclear atypia, tumor rupture, and mitotic index have been reported for these lesions, some are not observed consistently (5-15). FIGO stage has been reported as a significant prognostic factor for GCT. The 5-year survival rate ranges from 75-95% for patients with stage I GCT and decreases to 22-50% for stage III/IV cases (1). Our current results also found that stage is significantly associated with recurrence in GCT. Although stage was not significant in multivariate analysis, this may be due to the small number of patients with advanced-stage disease in our series.
Univariate Cox proportional hazard regression analysis of prognostic factors for patients with granulosa cell tumor recurrence with stage I disease.
Several studies have suggested tumor size to be a prognostic factor for GCT, with a size of less than 10-15 cm being a predictor of recurrence (5, 8, 12-15). Our current study also indicated size to be of predictive value for recurrence because even after analysis of stage I disease only, tumor size was still found to be associated with recurrence (Table IV). Considering the indolent clinical behavior of GCT, a large tumor indicates that disease occurred long before diagnosis. This may be explained by our current findings that large tumors predict a poor prognosis.
Another significant GCT prognostic factor is the presence of a postoperative residual tumor. All patients with residual disease after initial surgery in our current series had tumor recurrence and two died. As is the case for epithelial ovarian cancer, postoperative residual tumors are proposed as important prognostic factors in GCT (2, 8, 9). Theoretically, postoperative residual tumors will progress over time, causing recurrence or persistent disease (8). Hence, surgeons should make every effort to detect and fully-excise metastatic tumors.
The prognostic value of complete surgical staging for GCT, including systemic lymphadenectomy, is debated (1, 5, 8). Surgical staging did not show an association with DFS in our study. Notably, however, no lymph node metastases occurred in the 27 patients with complete surgical staging. However, two of our patients had pelvic involvement detected microscopically and six cases had a gross extra-pelvic tumor mass including the omentum. These findings emphasize on the importance of continued staging procedures, such as multiple peritoneal biopsies and omentectomy, even if a lymphadenectomy is not required (15, 19, 20).
FSS should be considered for patients with early-stage GCT desiring to retain their fertility (7, 13). In the present study, 5 out of 30 patients treated with FSS had a recurrence, 4 of which remain disease-free. The efficacy of a wedge biopsy of the contralateral ovary is debated and should be performed cautiously because of the low incidence of bilaterality (2% to 8%) (1). The bilaterality rate in our current series was 5.5% and only two out of our 80 stage I cases had bilateral disease. Hence, FSS with a unilateral salpingo-oophorectomy seems to be a reasonable treatment option in the absence of extraovarian spread.
Twenty-one of our patients with GCT underwent laparoscopic surgery (complete staging=8, partial staging=8) and all were stage I. Laparoscopic approaches did not compromise survival outcomes compared with a laparotomy in our study cohort. Reports have emerged suggesting that a laparoscopy as either a primary surgery or surgical re-staging is feasible and safe for selected ovarian sex-cord stromal tumors (21, 22). Although further evidence is needed, a laparoscopy is feasible for early-stage GCT when adequate surgical techniques and strict guidelines are followed.
In our current dataset, the pelvis was the most frequent (86.6%) site of first relapse, with the retroperitoneum in second place (13.3%). Two-thirds of these recurrences were multi-focal. The reported pelvic and extrapelvic recurrence rates are 55.0% and 47.7%, respectively, and retroperitoneal involvement is reported in up to 15% of first relapse cases (8, 9, 20, 23). Tumor dissemination patterns in recurrent GCT cases are different from the initial diagnosis. GCTs are inclined to initially arise without retroperitoneal involvement. By contrast, and similar to recurrent epithelial ovarian cancer, the vast majority of recurrences in our series involved multiple abdomino-pelvic fields. Multivisceral surgical approaches will thus often be required to resect recurrent tumors completely. Nevertheless, a complete tumorectomy following GCT recurrence is more achievable (85-91%) compared with epithelial ovarian cancer (16, 23).
Given that standard guidelines for the treatment of recurrent GCTs are lacking, various approaches such as surgery, chemotherapy, radiotherapy, and hormonal and target therapies have been suggested (24-27). In our current series, the absence of residual tumor after secondary surgery conferred a statistically significant improvement in survival following a first relapse. Chua et al. demonstrated the feasibility of a repeated peritonectomy to achieve complete cytoreduction in five patients with recurrent GCT with prolonged DFS (28). Current evidence suggests that complete tumor resection is a prognostic factor not only at initial surgery but even at recurrence in GCT.
We could not evaluate whether chemotherapy improved the outcome at relapse because all our patients with recurrent GCT received chemotherapy. The role of salvage chemotherapy at relapse remains uncertain. One report suggested that chemotherapy did not appear to improve the outcome at relapse (16). However, chemotherapy can be used for inoperable disseminated disease or disease with suboptimal cytoreduction (18, 29). A Gynecology Oncology Group phase II study reported that the BEP regimen was an active combination with a tolerable toxicity profile in patients with both advanced primary and recurrent (18). In another study, taxanes demonstrated activity against GCT and may be less toxic than BEP (30). Further studies of GCT cases are required to confirm the role of chemotherapy in treating this rare disease.
Our present study has limitations that are inherent to a retrospective design. Due to lack of data, we could not evaluate several histological or molecular markers as possible prognostic factors, including the mitotic index, Ki-67, and p53 (6, 31). In addition, the current study spans over 20 years, and it is likely that temporal changes in practice patterns, including adjuvant chemotherapy regimens, increase the difficulty of evaluating outcomes related to the care provided. However, the majority (82%) of patients who underwent initial surgery followed by adjuvant chemotherapy received BEP. Finally, our identified recurrence rate of 16.5% is relatively low compared with other studies (12, 20). Because GCTs have a typically late relapse, the recurrence rate would be expected to increase over a longer follow-up period. Longer follow-ups for patients with GCT are needed to further characterize recurrent GCT. Nevertheless, the present report is one of only a few studies on a large GCT series that has assessed treatment outcomes for recurrent GCT.
In conclusion, we have identified initial disease stage, tumor size, and postoperative residual disease as prognostic factors in adult GCT. Moreover, in cases with no residual disease, FSS can be performed in selected patients to preserve fertility. It is also important to achieve a complete tumorectomy without macroscopic residual disease in the treatment of GCT recurrence. Although the GCT recurrence pattern is mainly multifocal, a high rate of complete tumor resection encourages clinicians to attempt a surgical approach in the management of recurrent GCT. However, future prospective, well-designed, multi-center trials are required to better-elucidate the findings for this rare cancer.
Acknowledgements
We thank Sun Ok Kim, M.S., Department of Clinical Epidemiology and Biostatistics, University of Ulsan College of Medicine, Asan Medical Center, for statistical consultation.
- Received December 10, 2013.
- Revision received January 3, 2014.
- Accepted January 7, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}