


Abstract
Background: Overexpression of the human epidermal growth factor 2 (HER2) is associated with an aggressive metastatic phenotype in patients with breast cancer but its prognostic impact is not well-characterized in gastroesophageal adenocarcinoma. Patients and Methods: This is a retrospective series of three cases of HER2-positive gastroesophageal cancer. Results: In this case series, we describe three patients presenting with widespread metastatic disease prior to development of symptoms from the primary tumor. Two patients presented with brain metastases, while one demonstrated lymphangitic spread to lungs. Conclusion: Pooled analyses of outcomes among sub-populations of contemporary trials are needed to better understand the natural history and prognostic impact of HER2 over-expression in patients with gastroesophageal cancers.
- Esophagogastric adenocarcinoma
- gastroesophageal adenocarcinoma
- gastric adenocarcinoma
- esophageal adenocarcinoma
- HER2 over-expression
- HER2 amplification
- central nervous system metastasis
The human epidermal growth factor 2 (HER2) is over-expressed in approximately 6% to 35% of patients with gastroesophageal cancers (1-4). In breast cancer, HER2 over-expression is associated with poor prognosis in the absence of HER2 targeted-therapy, along with a predilection for metastatic disease to the central nervous system (CNS) (5, 6). In gastroesophageal cancers, the prognostic impact of HER2 over-expression is not well understood (7).
As in HER2-positive breast cancer, addition of the monoclonal antibody trastuzumab to chemotherapy improves outcomes in patients with metastatic HER2-positive gastroesophageal adenocarcinoma. In the phase III Trastuzumab for Gastric Cancer (ToGA) trial, patients with HER2-positive advanced gastric or gastroesophageal junction adenocarcinomas were randomized to first-line treatment with cisplatin plus a fluoropyrimidine with or without trastuzumab (4). The median overall survival and response rate were significantly improved in the trastuzumab arm compared to chemotherapy alone. Based upon ToGA, clinical practice guidelines now recommend HER2 testing by immunohistochemistry (IHC) and/or fluorescent in situ hybridization (FISH) in all patients with metastatic gastroesophageal adenocarcinomas (8).
We herein present a case series of three patients with HER2-positive, metastatic gastroesophageal adenocarcinomas. Each patient presented with symptoms of extensive metastatic disease at diagnosis, including synchronous CNS disease in two of the cases, rather than symptoms caused by the primary tumor itself. Our aim is to describe the aggressive course of these cases and consider the implications for clinical management and future research in this biomarker-defined population.
Case Report
Patients and methods. This retrospective case series was approved as an exempted category of research by the University of California, San Francisco Institutional Review Board. Cases were identified by the treating investigator.
Case 1. A 58-year-old male presented with headaches and gait instability. Computerized tomography (CT) of the brain showed multiple brain lesions consistent with metastases (Figure 1B). Whole-body imaging revealed a gastroesophageal junction mass along with synchronous metastases to liver (Figure 1A) and lymph nodes. Biopsy of the gastroesophageal junction mass was consistent with a diagnosis of primary metastatic gastroesophageal junction adenocarcinoma. He received palliative whole-brain radiation therapy and then started standard first-line chemotherapy with epirubicin, oxaliplatin and capecitabine (EOX) (9). After six cycles of therapy, repeat CT imaging showed a dramatic decrease in size of hepatic and nodal metastases.
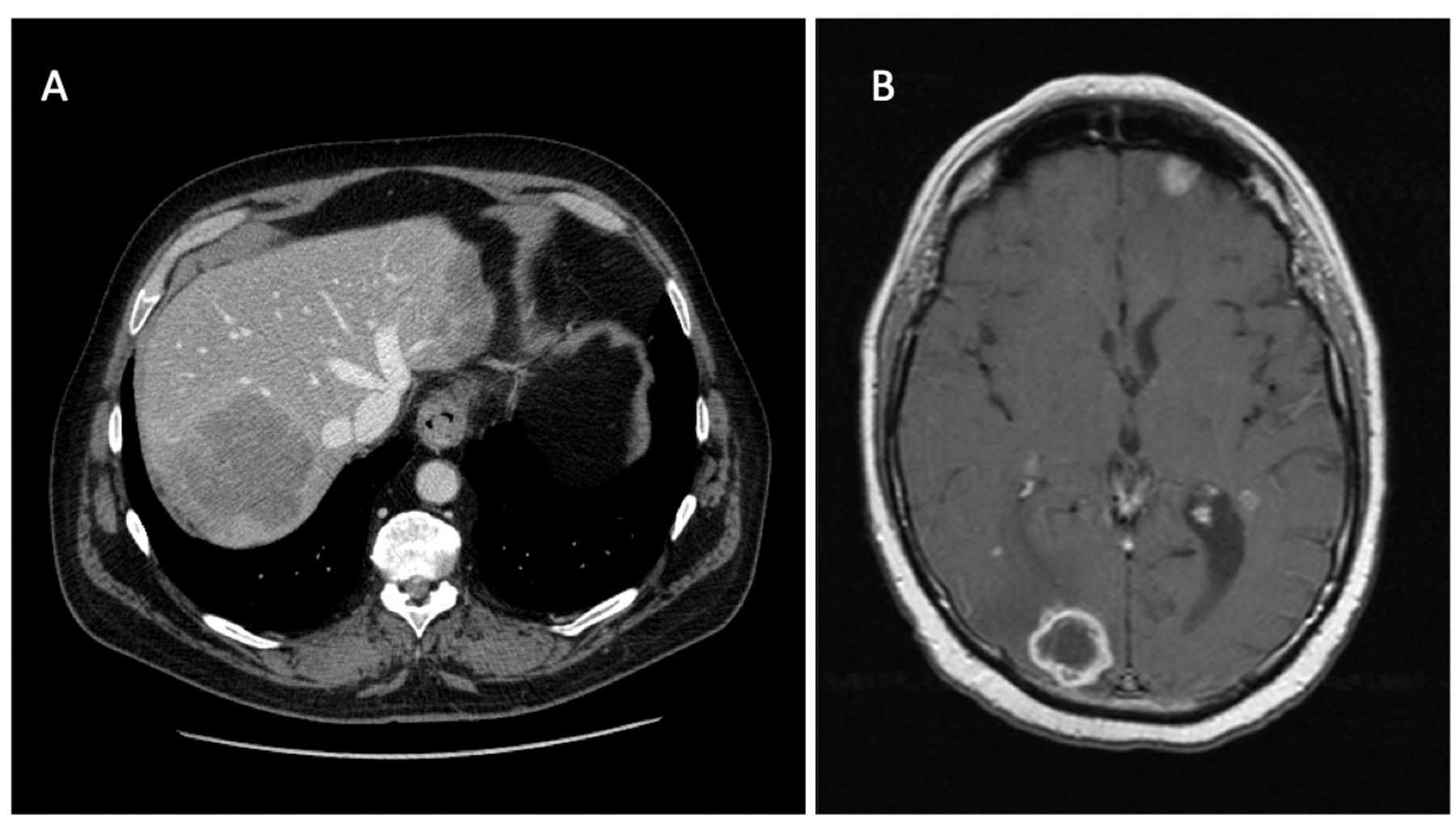
Case 1 imaging. A. CT Abdomen showing liver metastases. B. MRI brain with multiple metastatic brain lesions.
After a one-month chemotherapy holiday, a repeat brain magnetic resonance imaging (MRI) showed new brain metastases, which were treated with gammaknife. Subsequent imaging showed hepatic progression and peritoneal carcinomatosis. Meanwhile, HER2 testing demonstrated biphenotypic over-expression by IHC (Figure 2), whereas FISH was positive for amplification (ERB-B2 to centromere 17 ratio of 14.0). He was treated with a combination of irinotecan and trastuzumab. After one cycle, he succumbed to CNS progression, approximately 10 months after diagnosis.
Case 2. A 55-year-old male presented with dyspnea, right upper quadrant abdominal pain and weight loss. A CT scan of the abdomen and pelvis showed asymmetric wall thickening of the distal esophagus and proximal stomach, hepatic lesions, peritoneal implants and lymphadenopathy. Chest CT was notable for bibasilar pulmonary nodules and lymphangitic spread. Biopsy of an ulcerated distal esophageal mass with extension to the gastroesophageal junction revealed moderately differentiated adenocarcinoma with HER2 positivity (3+) by IHC, leading again to a diagnosis of primary metastatic gastroesophageal adenocarcinoma.
The patient initiated chemotherapy with the EOX regimen and demonstrated a marked response in lymphadenopathy and pulmonary nodules after four months, followed by progression soon thereafter. This prompted a transition to second-line chemotherapy with carboplatin, paclitaxel and trastuzumab based upon interval reporting of the ToGA trial results. Soon after, he passed away from complications of lymphangitic pulmonary progression, approximately 6 months after diagnosis.
Case 3. A 60-year-old male presented with worsening headaches and disequilibrium. The patient was found to have multiple brain lesions with vasogenic edema on CT, consistent with metastatic disease. Imaging revealed a mass extending from the mid-esophagus to the gastroesophageal junction. An endoscopy identified an endoluminal distal esophageal mass, with adenocarcinoma positive for HER2 by IHC (3+) on biopsy.
The patient was treated with palliative whole-brain radiotherapy followed by capecitabine, carboplatin and trastuzumab according to the ToGA regimen. After 6 cycles, he experienced complete radiographic response with no evidence of residual disease by esophagogastroduodenoscopy (EGD) with random biopsies. On maintenance trastuzumab, he developed CNS progression treated with gamma knife radiosurgery. He subsequently enrolled in a Phase I clinical trial investigating an AKT inhibitor in combination with paclitaxel and trastuzumab, completing five cycles with partial response. He eventually expired due to complications of CNS progression approximately 24 months after diagnosis.
Discussion
We have described the cases of three patients with primary metastatic gastroesophageal adenocarcinomas positive for HER2 over-expression. All three presented with synchronous metastatic disease, including multifocal brain metastases in two cases and lymphangitic spread to lungs in the third.
In most cases of gastroesophageal cancers, symptoms from the primary tumor, such as obstruction or bleeding, lead to diagnosis before metastatic disease is identified. In the three cases we presented, the observation that index symptoms arose from widely metastatic disease without symptomatic primary tumors suggests an aggressive, metastatic phenotype, as is well-described in HER2-positive breast cancer. Acknowledging the limitations of a small case series, these cases raise the hypothesis that HER2 over-expression may have similar prognostic impact in gastroesophageal cancers as in breast cancer, including a possible predilection for brain metastases, which are relatively uncommon in gastroesophageal cancers overall (10, 11). If an increased incidence of brain metastasis is confirmed in HER2-positive gastroesophageal cancers, it may be appropriate to implement guidelines similar to those in breast cancer, which support early interventions for CNS symptoms in patients with HER2-positive disease.

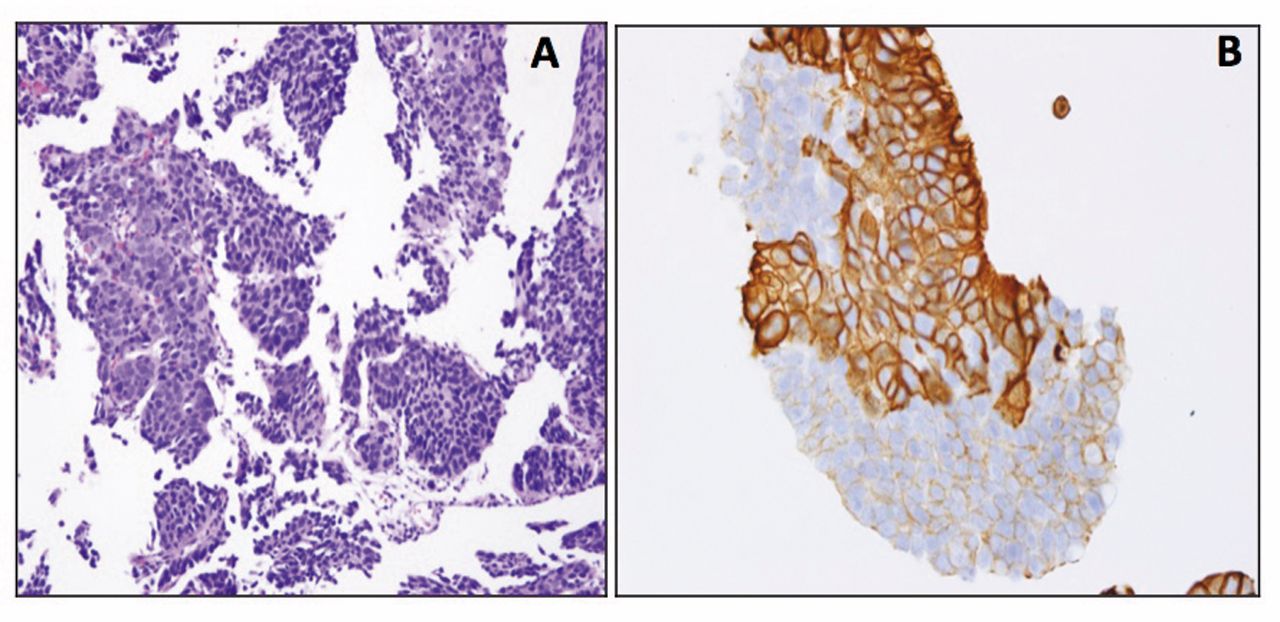
Case 1 histology. A. Adenocarcinoma (×20 magnification). B. Biphenotypic IHC staining of HER2 protein (×40 magnification).
The first two cases were diagnosed prior to reporting of the ToGA trial results. While impossible to draw any conclusions from such a small series, it is noteworthy that the patient in Case 3 who received first-line trastuzumab based on the ToGA results experienced significantly prolonged disease response and survival. This observation certainly supports the inclusion of trastuzumab in the first-line of chemotherapy for patients with HER2-positive metastatic gastroesophageal adenocarcinoma, as is now the standard of care for gastroesophageal cancers with HER2 over-expression or HER2 amplification based upon the results of ToGA (8).
The pathological findings in these patients also exemplify the evolving understanding of the differences between HER2 over-expression patterns by immunohistochemistry in gastroesophageal adenocarcinoma by comparison to breast cancer. Initially, breast cancer criteria were employed to define HER2 positivity in gastroesophageal cancers. Since ToGA, two major differences have emerged. First, although not seen in this series, it has been recognized that incomplete basolateral membrane staining is a common finding in gastroesophageal tumors. Secondly, higher degrees of intratumoral heterogeneity are present in gastroesophageal cases than in breast, such as the biphenotypic HER2 staining and HER2 amplification seen in Case 1 (Figure 2). These differences have warranted the development and validation of independent HER2 scoring criteria for gastroesophageal cancers (8, 12).
In summary, these three cases of HER2-positive gastroesophageal cancer demonstrated unusual presentations with symptoms of widespread metastatic disease, raising the hypothesis that HER2 positivity may be associated with a metastatic phenotype in gastroesophageal cancers, including a possible propensity for CNS metastases, which warrants further study in larger cohorts. Ongoing studies of next-generation HER2-targeted therapies, including trastuzumab emtansine (T-DM1) and pertuzumab, are underway, which promise to advance our understanding and management of this unique and important molecularly-defined subpopulation of gastroesophageal cancers.
Footnotes
-
Disclosures
None of the Authors disclose any potential conflicts that are relevant to the manuscript.
- Received August 13, 2014.
- Revision received August 18, 2014.
- Accepted August 25, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}