


Abstract
Aim: To describe the feasibility, safety, and oncological outcomes of a modified triple-incision total radical vulvectomy and inguino-femoral lymphadenectomy in patients with locally advanced squamous vulvar cancer. Patients and Methods: A modified triple-incision technique performed by two surgical teams operating simultaneously under regional anesthesia was performed on a consecutive series of 57 patients with Fédération Internationale de Gynécologie Ostétrique (FIGO) stages IB ≥4 cm to III squamous vulvar cancer. Adjuvant radiation therapy was delivered according to margin status and groin involvement. Surgical outcomes and follow-up data were retrospectively analyzed. Results: The mean age of patients was 75.5±10.7 years and 54 (94.7%) had at least one comorbidity. Fifteen (26.3%) had disease of clinical FIGO stage I ≥4 cm, 7 (12.3%) had stage II, and 35 (61.4%) had a stage III. All surgical procedures were completed as planned. The mean surgical duration was 108±37 min. Major intraoperative complications were observed in two cases (3.5%). Twenty-one (36.8%) patients received adjuvant radiation therapy. During a mean follow-up of 51.6±50.5 months, 29 (50.9%) patients developed local, regional or distant recurrence. The disease-free survival was 39.5±20.9 months. Nineteen (33.3%) patients died of primary disease. Overall survival for the entire cohort was 65.4%, with 3-year and 5-year overall survival of 60.5% and 48.6%, respectively. Conclusion: Our results seem to reveal that the procedure is safe, with surgical and oncological outcomes comparable to classic sequential triple-incision technique. The shortening of surgical duration along with the use of regional anesthesia can have significant advantages for perioperative care, reducing the global burden of treatment and increasing the number of patients eligible for therapeutic surgery.
Squamous vulvar cancer (SVC) is an uncommon gynecological malignancy that traditionally affects elderly women and constitutes 5% of all cancers of the female genital tract (1). The incidence of SVC in the general population is 1-2/100,000 women per year, while in women older than 75 years this rate is 10-fold higher (2, 3).
Tumor size, stage at diagnosis, and lymph node status are the most important prognostic variables for SVC (4). As well as for other cancer types, and more generally for all diseases, ageing represents an additional prognostic factor for SVC since increasing age confers high risk for a number of other health problems. Studies have shown that age and comorbidities strongly influence therapeutic decisions and are associated with less aggressive cancer therapy (3-5).
Complete surgical excision of the primary disease represents the cornerstone of the treatment of SVC. However, for elderly patients with locally advanced SVC suffering from other medical comorbidities, the standard surgical approach, consisting of total radical vulvectomy (TRV) and inguino-femoral lymphadenectomy (IFL) may be associated with significant perioperative morbidity and be potentially life-threatening.
In order to avoid the need for two subsequent surgical procedures (vulvectomy and lymphadenectomy), we developed a modified triple-incision technique for locally advanced SVC performed by two surgical teams operating simultaneously under regional anesthesia (RA).
The aim of this study was to describe this surgical technique, assess its feasibility, safety and its implications for morbidity and survival.
Patients and Methods
A review of the Departmental database was conducted to identify all patients with SVC treated at our Institution from January 1995 to December 2013. Among these, patients with locally advanced SVC [Fédération Internationale de Gynécologie Ostétrique (FIGO) stages IB ≥4 cm to III] and submitted to two-team simultaneous TRV and IFL via separate incisions were selected. Patients with non-squamous histology or with previous (within five years of the SVC diagnosis) or concomitant diagnosis of other malignancies were excluded from the analysis. Medical charts, operative records, pathology reports and follow-up data were reviewed and the following information was extracted for each patient: age, body mass index (BMI), comorbidities, American Society of Anesthesiology (ASA) score, stage according to FIGO classification, grading, surgical procedure, type of anesthesia, operative duration, estimated blood loss (EBL), intra- and postoperative complications, removal of inguinal drains, length of hospital stay, re-operations, adjuvant radiation therapy (ART), length of follow-up, recurrences, and survival.
Single or multiple punch biopsies were used to obtain preoperative histology. Tumor size and contiguous organ involvement were established by low-power magnified examination. Cystoscopy and/or proctoscopy were performed in cases of urethral/anal involvement. Preoperative work-up consisted of general and pelvic examinations, chest and abdominal computed tomography (CT) and routine blood examinations. Written informed consent was obtained from all the patients.
Patients with involved surgical margins or with at least two involved groin nodes or extracapsular spread of groin nodal involvement received adjuvant radiation therapy (ART).
In cases of positive margins with negative groin nodes, the vulvar region was treated with an electron beam to a total dose of 50 Gy. In thecase of positive nodes, the treatment volume consisted of the pelvic and bilateral inguinal area to a total dose of 50 Gy, with a boost to the positive involved nodes up to 60 Gy.
Follow-up visits were scheduled every four months in the first two years and twice a year until the fifth year. At each visit, clinical examination was performed, and punch biopsies were carried out on any area of local abnormality. Abdominal and pelvic ultrasound scan (US) were performed every six months; chest X-ray and CT scan were performed once a year for five years.
Statistical analysis was performed using SPSS Version 15.0 statistical package (SPSS, Chicago, IL, USA). Results are expressed as the median (range) for discrete variables and mean±standard deviation (SD) for continuous ones. Disease-free survival (DFS) was defined as the time from surgery to local recurrence or metastasis. Overall survival (OS) was defined as the time from the date of surgery to the date of death from the disease or to the last follow-up visit. OS and DFS were estimated using the Kaplan–Meier method, and compared between subgroups using the log-rank test. All calculated p-values were considered statistically significant if less than 0.05.
Surgical technique. All patients received antibiotic [1 g cefazolin intravenous (i.v.), 30 min before surgery] and anti-thrombotic prophylaxis (4000 IU/day enoxaparin from the day before surgery and lower-extremity compression device).
The anesthetic technique was spinal anesthesia (1995-2003) or combined spinal-epidural anesthesia (2004-2013), both associated with minimal sedation. Spinal-epidural anesthesia was performed through lumbar puncture at L3-L4 using a midline approach. An 18-gauge needle was introduced using loss of resistance to saline technique, and the dura was punctured with a 27-gauge needle using the needle-through-needle technique. After confirming the subarachnoid space with aspiration of cerebrospinal fluid, 10 mg of 0.5% hyperbaric bupivacaine was administered. After withdrawal of the spinal needle, a 20-gauge epidural catheter was inserted through the epidural needle 3-4 cm into the epidural space. At the end of surgery, a bolus of 10 ml of 0.625 mg/ml levobupivacaine and 0.5 μg/ml sufentanil was given through the epidural catheter and repeated every hour during the first 24 hours. Patients in the spinal group received 10 mg of 0.5% hyperbaric bupivacaine mixed with 0.10-0.20 mg of morphine through a 27-gauge needle via a 20-gauge introducer, after free flow of cerebrospinal fluid was observed. Postoperatively, 4 g/24 h paracetamol i.v. and 30 mg/30 h morphine administered continuously via elastomeric pump were used for the control of postoperative pain. Ketoralac at 90 mg/24 h i.v. was used as rescue analgesia.
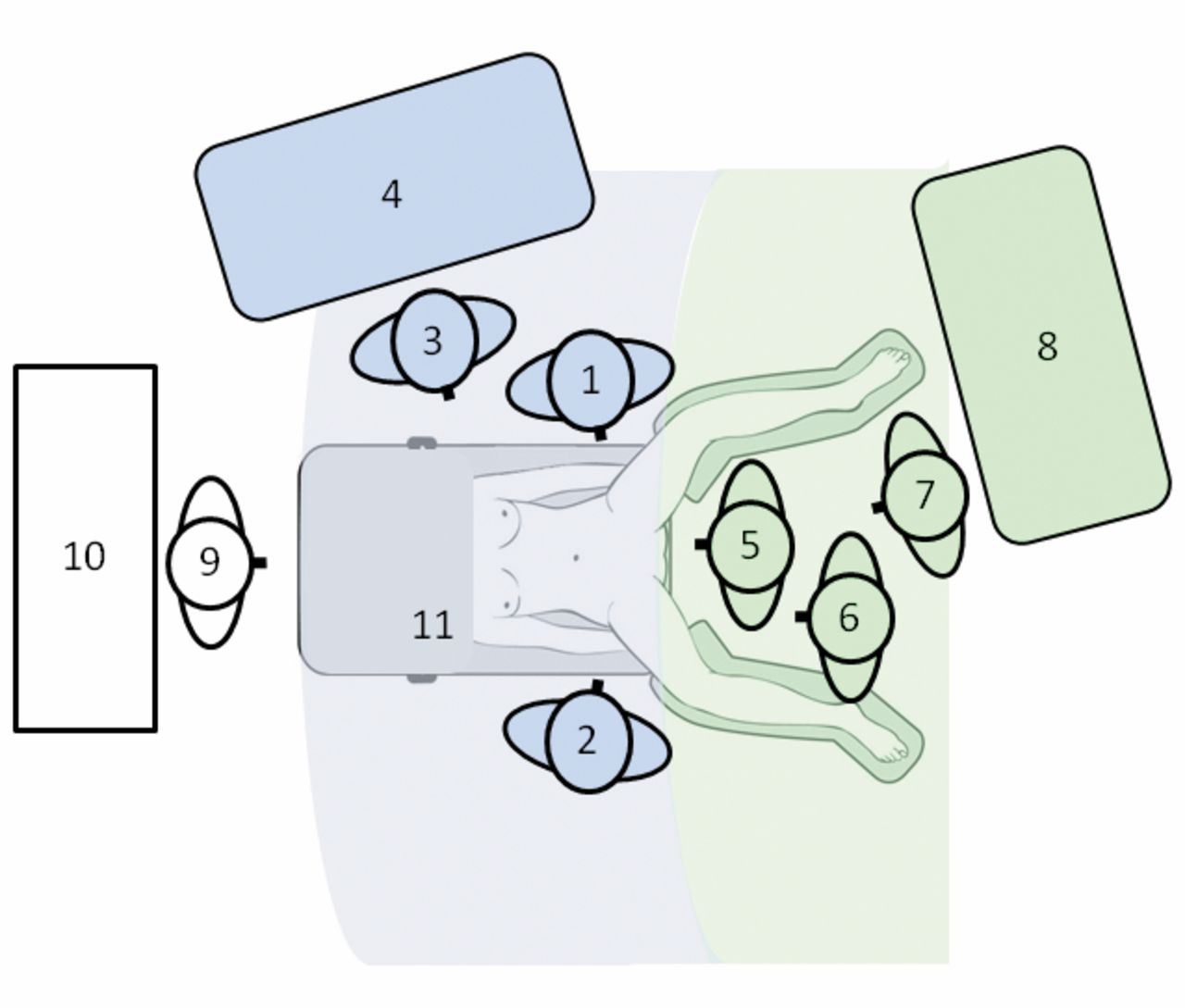
The patient was positioned lying supine with thighs in external rotation, placed at 30° angles to the surgical table and opened at approximately 60° to provide adequate exposure both to the inguinal region and perineum. In all cases, two teams performed the surgery: one for TRV and the other for IFL. Surgical procedures started at the same time. Each team consisted of an attending gynecological surgeon, an obstetrics and gynecology surgical resident, and a scrub nurse. The positions of the patient, surgeons, nurses and instrument tables an illustrated in Figure 1.
TRV and IFL were performed according to standard triple-incision technique.
Concerning vulvar operation, the outer and the inner incisions were first drawn with a 2 cm margin from the tumor. Anterior skin incision was basically elliptical entering through the fatty tissue of the mons pubis down to the periosteum, and removing the clitoris by the division of the suspensory ligament. Laterally, the dissection was developed down to the level of the deep fascia of the thigh, moving then medially to the inferior fascia of the urogenital diaphragm towards the lateral aspect of the vaginal wall. The vaginal incision was made circumferentially above the urethral meatus, ensuring that the required margin around the tumor was maintained. The outer incisions were then extended posteriorly and carried down to the level of the deep fascia enveloping the sphincter ani muscle. After removal of the specimen, primary closure was often possible. Anteriorly, the defect was closed side-to-side in two layers. The lateral skin was sewn to the vagina incorporating the levator ani muscles to give strength to the closure. Sometimes the posterior vaginal wall could be undermined to cover the perineal body. If closure of the defect required undue tension, a V-Y fasciocutaneous advancement flap was used.
Groin dissection was performed through an 8-10 cm skin incision parallel and approximately 1 cm above to the groin crease. The incision was carried through the subcutaneous tissues to the superficial fascia (Camper fascia). The superficial fascia was incised and the lympho-fatty tissue between it and the fascia lata was removed over the femoral triangle. The dissection was then carried medially into the fossa ovalis deep to the cribiform fascia where the femoral vein was encountered. Femoral lymph nodes were dissected from the anterior and medial surfaces of the femoral vein above the lower limit of the fossa ovalis. The great saphenous vein was usually preserved during groin dissection. A 7 mm Jackson-Pratt flat drain was placed in the groin dissection and the wound was closed by two layers of interrupted stitches.
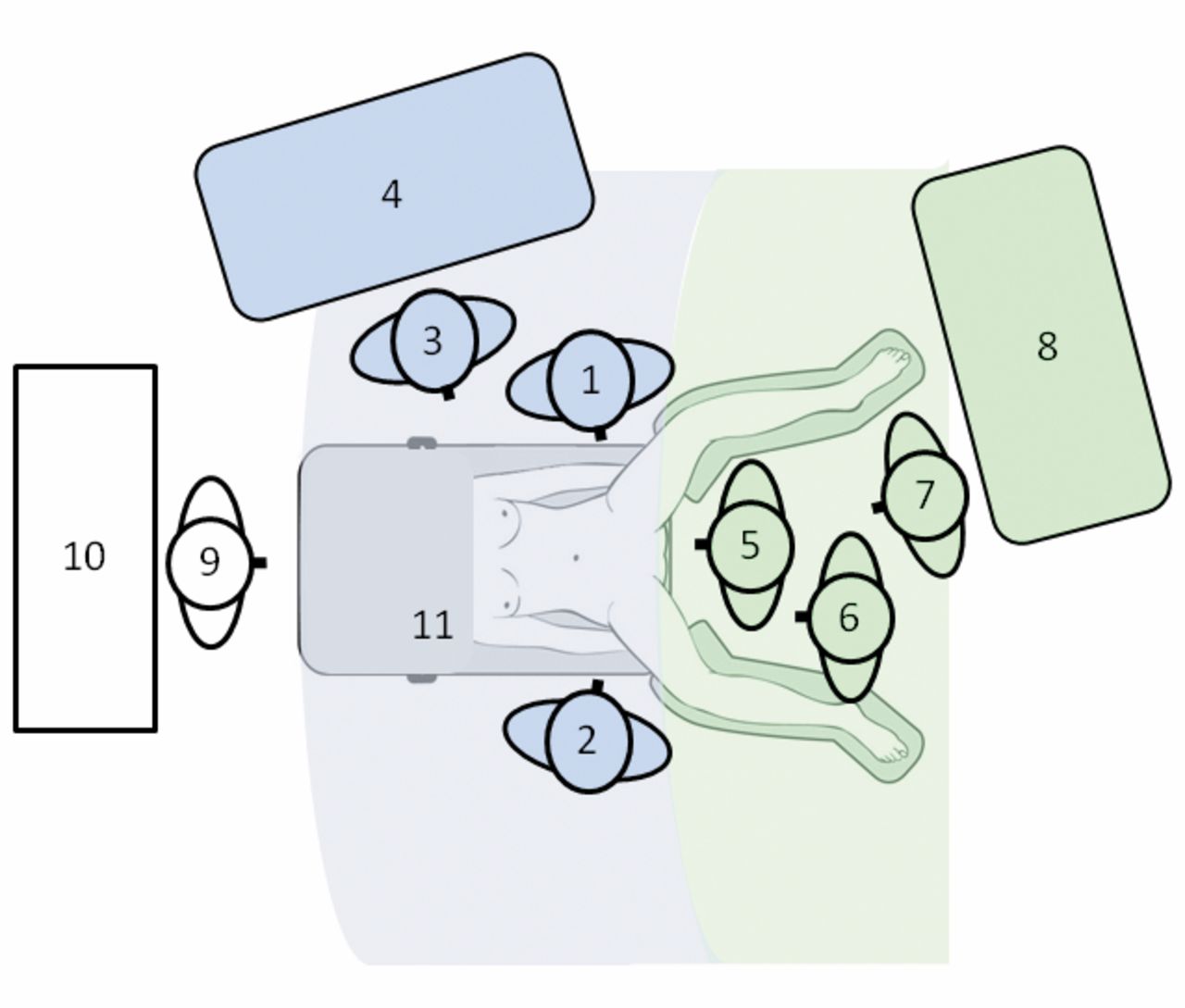
Positioning of patient and surgical teams during intervention. Surgical areas for perineal and inguinal procedures are colored in green and blue, respectively. 1: Primary surgeon; 2: first assistant; 3: scrub nurse; 4: instrument table; 5: primary surgeon; 6: first assistant; 7: scrub nurse; 8: instrument table; 9: anesthetist; 10: anesthesiology equipment; 11: surgical table with supine patient.
Results
During the study period, 207 patients with histologically-diagnosed SVC were admitted to our Institution for surgical treatment. Among these, 57 (27.5%) were diagnosed with locally advanced SVC (FIGO stages IB ≥4 cm–III) and all of them underwent surgery according to the described technique.
Patients' characteristics are listed in Table I. The mean age was 75.5±10.7 years, 54 (94.7%) patients had at least one comorbidity including hypertension, diabetes mellitus, previous thromboembolism and cardiovascular disease. Twelve (21.1%) patients were clinically/radiologically suspected as having unilateral or bilateral inguinal node metastasis.
All patients successfully underwent a TRV and bilateral IFL via a two-team simultaneous approach. Intra- and postoperative surgical data are described in Table II.
To obtain free surgical margins, a colostomy, a distal vaginal resection and a partial urethral removal were performed in one (1.7%), four (7.0%) and two (3.5%) patients, respectively. Perineal defect was closed primarily in 54 patients (94.7%), whereas in three (5.3%) cases, a V-Y fasciocutaneous advancement flap was performed. The mean duration of surgery was 108±37 minutes. All the procedures were successfully performed under regional anesthesia (RA): spinal: 19 (33.3%); spinal-epidural: 38 (66.6%). One case of intraoperative bleeding from the left femoral vein and one case of rectal perforation were observed during operations. Postoperative complications involving the surgical sites (wound infection or dehiscence) or lymphatic drainage (lymphedema or lymph cyst) were observed in 19 (33.3%) patients. None of them required surgical re-intervention.
Patients' characteristics (n=57).
Intra- and postoperative data (n=57).
After definitive pathological analysis, most patients (35, 61.4%) had a stage III cancer. Grade 3 was observed in 13 (22.8%) cases, lymph node metastasis in 35 (61.4%), and involved surgical margins in 10 (17.5%). Pathological results are detailed in Table III.
After surgery, 21 (36.8%) patients received ART. ART to the vulvar region was performed in five (8.8%) cases; pelvic and inguinal ART was performed in 11 (19.3%) cases. Five patients (8.8%) underwent ART to vulvar and inguino-pelvic areas.
Follow-up data are shown in Table IV. After treatment 29 (50.9%) patients developed local, regional or distant recurrence of disease, with a median progression-free survival of 39.5±20.9 months.
During a mean follow-up of 51.6±50.5 months, 19 (33.3%) patients died of primary disease, whereas two (3.5%) patients succumbed to comorbid diseases. OS for the entire cohort was 65.4%, with 3-year and 5-years OS of 60.5% and 48.6%, respectively. OS was significantly associated with the number of positive lymph nodes (p=0.02), with margin status (p=0.01), and with distant metastasis (p=0.003).
Pathological data (n=57).
Discussion
Over the past 20 years, surgical treatment for patients with SVC has become more conservative and individualized with the intention of reducing surgical morbidity without compromising the prognosis. The modification of TRV to wide local excision (6) and the introduction of the sentinel lymph node procedure represent the main advances in the field of surgical treatment for early-stage SVC (7).
Considering locally advanced SVC, certain studies support the use of concurrent primary chemoradiation as an effective alternative to primary ultra-radical surgery, with complete remission rates between 53% and 72% (8, 9). Moreover, although no randomized controlled trials have been completed, a recent Gynecologic Oncology Group phase II trial with neoadjuvant chemoradiation for inoperable locally advanced SVC showed 64% complete clinical and 78% pathological response rates, with acceptable toxicity (10).
However, despite recent efforts towards the individualization of care, up-front surgery still represents the first choice for locally advanced SVC when primary treatment will not require performing a stoma. For these patients, the surgical technique remained unchanged from the 1960s when Byron et al. introduced the triple-incision technique as an alternative for the en bloc approach (11). The surgical burden of radical treatment via the triple-incision technique has decreased compared to the en bloc operation but still remains significant.
SVC typically affects elderly patients who are likely to have pre-existing health issues. The pre-diagnostic health status of patients with SVC may affect patterns of care and treatment decisions. A recent Surveillance, Epidemiology, and End Results analysis indicates that compared with younger women, older women with SVC were more likely to present with advanced disease and less likely to undergo surgery and groin dissection, but were more likely to receive primary radiation (3). This may have been due to the reluctance of physicians to undertake standard surgery in older patients because of the increased potential for post-surgical complications.
Follow-up data (n=57).
In the present study, we describe a modified triple-incision technique for locally advanced SVC performed by two surgical teams operating simultaneously under RA.
Data on patient characteristics revealed advanced age at diagnosis, with high rate of comorbidities and a high ASA score. These findings are consistent with those from previous studies (10, 12), confirming that locally advanced SVC is diagnosed in elderly and surgically high-risk patients.
Technically speaking, we described a classic triple-incision TRV with IFL. Indeed our surgical approach differs from previously described procedures in two main aspects. Firstly, the perineal and inguinal phases are performed by two independent surgical teams operating simultaneously, allowing a reduction (ideally a halving) of surgical time. The proper positioning of the patient enables good exposure of surgical fields, allowing fast and safe procedures in both inguinal and perineal areas. Our surgical findings (number of removed lymph nodes, estimated blood loss, complications, re-operations, hospital stay) are consistent with those reported by others (13-16), suggesting the appropriateness of this simultaneous approach from a technical viewpoint. In terms of oncological outcomes, all the variables in the current study are also comparable with previous published data (2, 4, 6, 12, 17), even if a randomized controlled trial should be performed to validate our findings. A two-team approach previously described to shorten the time of surgery in some gastrointestinal (18), head and neck (19), and orthopedic (20) interventions. The mean operative time recorded in our series is shorter than those reported by others using classic sequential triple-incision technique (21), although the comparison may not be reliable given the difference in the use of reconstructive procedures. However, it is reasonable to believe that whatever the technique used and procedures combined, the simultaneous approach has a beneficial effect on reducing overall operative time.
Secondly, the reduction of operative time associated with this simultaneous approach enables use of RA instead of general anesthesia (GA). Several studies have shown that RA is associated with significantly reduced intraoperative blood loss and with better control of respiratory parameters both intraoperatively and perioperatively when compared to GA (22, 23). RA is also associated with reduced pain and faster mobilization after surgery (24). Several authors showed that early ambulation together with a daily prophylaxis with enoxaparin might allow for reduction of the risk of thromboembolism (25). In a previous study comparing mini-laparotomy and vaginal surgery for obese high-risk surgical patients with endometrial cancer, we observed that RA was associated with a lower use of supplemental drugs for pain control, a lower incidence of thromboembolic events, and a shorter hospital stay when compared to GA (26). In a recent overview of systematic reviews, RA reduced the zero to 30-day mortality and the risk of pneumonia compared to GA (27). In a systematic review of all trials with randomization to RA or not, overall mortality was reduced by about a third in patients allocated to RA. RA also reduced the odds of deep vein thrombosis by 44%, pulmonary embolism by 55%, transfusion requirements by 50%, pneumonia by 39%, and respiratory depression by 59% (all p<0.001). There were also reductions in myocardial infarction and renal failure (28). Moreover, considering elderly patients, mental and psychomotor function may be delayed following the intravenous administration of anesthetic drugs because of a physiological reduction in drug metabolism. For this reason, delirium may occur in up to 50% of elderly patients after major surgical procedures performed with GA, and is associated with increased mortality, longer hospital stays, and cognitive and functional decline (29).
In conclusion, clinical research on the treatment of locally advanced SVC is moving toward the implementation of chemoradiation alone or combined with less aggressive surgery. However, the efficacy of more conservative therapies using adjuvant/neoadjuvant radiation with/without chemotherapy still needs to be addressed. The evaluation of treatment strategies in clinical trials is limited by the fact that most advanced tumors are diagnosed in elderly patients with compromised health status, limiting the surgical approach but also chemotherapy and radiation treatments. At present, surgical resection of primary vulvar disease still represents the best treatment choice, achieving the best possible survival outcomes. In a high-risk cohort of patients with locally advanced SVC, we performed a standard triple-incision technique through a simultaneous approach using RA techniques. Our results seem to reveal that the procedure is safe, with surgical and oncological outcomes comparable to existing data. The shortening of the surgical duration along with the use of RA can have significant advantages for perioperative care, reducing the global burden of treatment and increasing the number of patients eligible for therapeutic surgery. Randomized trials comparing our procedure with classic sequential technique are warranted to confirm our surgical and oncological outcomes.
- Received July 23, 2014.
- Revision received September 8, 2014.
- Accepted September 10, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.