


Abstract
Background/Aim: Tumor lysis syndrome (TLS) is a life-threatening oncological emergency, and control of serum uric acid level (S-UA) is most important. In this single-institution, short-term and pilot prospective study, the efficacy of a new xanthine oxidase inhibitor, febuxostat, as an alternative to conventional allopurinol, including its effects on hypoxanthine and xanthine, was evaluated in 10 consecutive patients with hematological malignancies at intermediate risk for TLS. Patients and Methods: Febuxostat at 40 mg (n=7) or 60 mg (n=3) daily was administered according to renal function, and induction chemotherapy was started within 24 h. The primary end-point was the reduction of S-UA to ≤7.5 mg/dl by day 5. Results: The median S-UA at base-line was 8.0 mg/dl (range=3.2-10.6 mg/dl). The median S-UA on day 5 after chemotherapy was 3.3 mg/dl (range=1.1-5.8 mg/dl) (p<0.0001, by paired t-test), indicating successful control of S-UA during chemotherapy. All patients achieved S-UA ≤7.5 mg/dl. A simultaneous decrease in serum creatinine and increase in estimated glomerular filtration rate were seen. Serum hypoxanthine and xanthine levels (as the consequence of inhibition of xanthine oxidase) were elevated along with the decrease in S-UA. Xanthine level was elevated higher compared to hypoxanthine level and reached the level reported to cause xanthine nephropathy, but no advance of renal impairment was observed. Serum febuxostat concentrations at 2 h after administration were 891.8±285.0 ng/ml (mean±SE) for the 40-mg dose and 770.6±242.7 ng/ml for the 60-mg dose (p=0.80, unpaired t-test), showing no accumulation in patients with renal impairment. No febuxostat-related adverse reactions were noted. No patients experienced progressive TLS. Conclusion: Febuxostat is promising for the management of TLS of an intermediate-risk patient and further observation and reevaluation regarding xanthine nephropathy should be performed.
Abbreviations: TLS, tumor lysis syndrome; UA, uric acid; S-UA, serum uric acid, S-Cr, serum creatinine; eGFR, estimated glomerular filtration rate; AML, acute myeloid leukemia; ALL, acute lymphoblastic leukemia; DLBCL, diffuse large B-cell lymphoma.
Tumor lysis syndrome (TLS) is a life-threatening oncological emergency that is characterized by metabolic impairment, including hyperkalemia hyperphosphatemia, hypocalcemia and hyperuricemia (1-3). It is caused by a massive lysis of cancer cells that accumulate very rapidly, or, more commonly, by the destruction of cancer cells secondary to initiation of chemotherapy (1-3). These metabolic complications can rapidly lead to renal insufficiency, cardiac arrhythmias, seizures, neurological disorder and ultimately death. However, TLS is preventable if detected and treated early in its course and it is essential to identify patients at risk of TLS who might benefit from prophylactic strategies or early treatment. Recently, sets of guidelines for the stratification of patients according to risk of developing TLS, optimal use of prophylactic measures and implementation of appropriate treatments have been published (1, 2). TLS can be divided into laboratory TLS and clinical TLS. Laboratory TLS is defined according to the abnormal serum values of uric acid (UA), potassium, phosphate or calcium (1, 2). Clinical TLS requires the presence of clinical manifestations in addition to the presence of laboratory TLS. Patients can be classified into low-, intermediate- and high-risk groups for the development of TLS, based on the type of malignancy, tumor burden and type of therapy, which thus enables stratification of appropriate treatment for each group (1, 2).
Control of serum uric acid (S-UA) level is most important in the management of TLS (4). The initiation of chemotherapy causes rapid lysis of tumor cells, and the subsequent release and catabolism of nucleic acids results in the massive production of UA (1, 2, 5). Specifically, purine nucleic acids are catabolized to hypoxanthine, then xanthine and finally to UA by xanthine oxidase. The rise in S-UA may induce precipitation of UA in the renal tubules, thereby leading to renal failure (4). According to published guidelines, two uric acid-lowering agents, a conventional xanthine oxidase inhibitor allopurinol and a recombinant uricase rasburicase are employed in the management of TLS; the former for intermediate-risk patients and the latter for high-risk patients (1, 2). Although rasburicase is quite potent, its use is limited by its immunogenicity and cost (6, 7). Allopurinol is a xanthine analog that, along with its metabolite oxypurinol, acts as a competitive inhibitor of xanthine oxidase, which otherwise converts hypoxanthine to xanthine and xanthine to UA (8, 9). Allopurinol has been shown to effectively decrease S-UA, thereby reducing the incidence of urate nephropathy in patients at risk of TLS (8, 9). However, allopurinol's onset of action is relatively slow (10, 11) and it can sometimes induce skin rashes, hypersensitivity and hepatic dysfunction (12). Importantly, some patients at a risk for TLS are complicated with reduced renal function, which would be a limitation to the use of allopurinol because the drug is primarily excreted from the kidney and renal impairment increases the risk of adverse events (13, 14). Therefore, allopurinol may not be the ideal agent for the management of TLS.
Febuxostat is a new non-purine analog xanthine oxidase inhibitor (15-18). The active ingredient is 2-(3-cyano-4-[2-methylpropoxy] phenyl)-4-methylthiazole-5-carboxylic acid (15). The agent has been approved for use in the treatment of chronic hyperuricemia and gout in the US, Europe and Japan (16, 17, 19-21). It is a more selective and potent inhibitor of xanthine oxidase than allopurinol and is thought to have very little effects on other enzymes involved in purine or pyrimidine metabolism (22). Febuxostat is mainly metabolized by the liver and is excreted by both the liver and the kidney, suggesting that it might be less affected by impaired renal function when compared with allopurinol (16). Clinical studies in patients with gout and hyperuricemia have demonstrated that febuxostat controlled UA levels more effectively and without increasing adverse reactions, when compared to allopurinol (20, 21). These advantages suggest that febuxostat might be a better option than allopurinol in cancer patients who are at intermediate risk for TLS.
In this single-institution, short-term and pilot prospective study, the efficacy of febuxostat, as an alternative to allopurinol, and its pharmacokinetics were evaluated in 10 consecutive patients with hematological malignancies at an intermediate risk for TLS. In addition, the study of precisely characterized pharmacodynamic changes in hypoxanthine and xanthine levels as a consequence of the mechanisms of action of febuxostat as xanthine nephropathy, is reported.
Patients and Methods
Study design. This was an open-label, single institute study of febuxostat administration for the management of TLS. The primary objective was to evaluate the UA-lowering efficacy of febuxostat in patients with hematological malignancies at an intermediate risk of TLS. Secondary objectives included evaluation of the safety of the agent, renal function, the pharmacokinetic profile of febuxostat and the pharmacodynamic determination of the levels of hypoxanthine and xanthine, the metabolites that were affected by the action of febuxostat.
Patients. This study was approved by the Institutional Review Board of University of Fukui Hospital and was conducted in accordance with the Helsinki Declaration. Written informed consent was obtained from all participants. A total of 10 Japanese patients were recruited. Eligible patients were age ≥20 years, had an Eastern Cooperative Oncology Group performance status of 0 to 2, active hematological malignancies and were at an intermediate risk for TLS. The risk for TLS was classified according to the published guidelines (1, 2). Diseases associated with an intermediate risk for TLS included acute myeloid leukemia (AML) with a peripheral white blood cell count between 10,000-50,000/μl, acute lymphoblastic leukemia (ALL) with a peripheral white blood cell count between 50,000-100,000/μl, diffuse large B-cell non-Hodgkin's lymphoma (DLBCL) and any other diseases associated with factors that could increase the risk of developing TLS (e.g., elevated serum lactate dehydrogenase, extensive bone marrow involvement, pre-existing renal disease or reduced urinary output) (1, 2, 12). The main exclusion criteria were severe renal dysfunction with estimated glomerular filtration rate (eGFR) ≤30 ml/min/1.73 m2 and hepatic dysfunction with transaminase levels ≥×2 upper normal limit, congestive heart failure, uncontrolled diabetes mellitus, uncontrolled hypertension, prior administration of agents that might affect S-UA concentrations (e.g., losartan, fenofibrate, atorvastatin, pyraziamide, cyclosporine), concomitant treatment for solid tumors, pregnancy or lactation, or psychological disorders.
Treatment and assessments. Febuxostat was administered orally after breakfast once daily for at least 7 days. Induction chemotherapy was started within 24 h after the first administration of febuxostat. They also received increased hydration. The dose of febuxostat was 60 mg for patients with eGFR ≥90 ml/min/1.73 m2 and 40 mg for patients with eGFR between 30 and 90 ml/min/1.73 m2 because 26% increase in the maximum concentration (Cmax) was observed in patients with mild renal dysfunction (Feburic tablets™, Interview form, August, 2012, Teijin Pharma, Ltd, Tokyo, Japan) (19-21). The primary end-point was the overall response rate for febuxostat treatment, according to previous studies (1, 23, 24). Treatment was considered as successful and the patient was considered to be a treatment responder if S-UA level was ≤7.5 mg/dl by day 5 of chemotherapy (1, 23, 24). S-UA levels were determined in-house using a TBA-c16000 automatic analyzer (Toshiba, Tochigi, Japan) (25). Secondary end-points included adverse events, renal function, pharmacokinetics of febuxostat and hypoxanthine and xanthine levels. Adverse event reports and hematology and chemistry data were collected up to the 14th day of chemotherapy. The severity of adverse events was graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events 4.0 (May 28, 2009). Renal function was evaluated by determining serum creatinine (S-Cr) and eGFR. The pharmacodynamic determination of hypoxanthine and xanthine and the pharmacokinetic evaluation of febuxostat are described in detail in the sections below.
Patients' characteristics.
Measurement of levels of oxypurines (hypoxanthine, xanthine). Serum and urinary hypoxanthine and xanthine concentrations were determined using a liquid chromatography-tandem mass spectrometry (LC-MS/MS) method (26). Blood samples were collected daily until day 7, while urine samples were obtained on day 0, 1 and 7. The sample (20 μl) was then mixed with the internal standards (hypoxanthine-15N4 for hypoxanthine, xanthine-1,3-15N2 for xanthine) in phosphate-buffered saline (in total of 110 μl) from which an aliquot (20 μl) was added to 10 mM ammonium acetate-methanol (5:95 v/v) (200 μl). The sample was then centrifuged (10,000 × g, 5 min) and the supernatant was isolated and used for the measurement of oxypurines. Chromatographic separation was performed on an Inertsil HILIC (150×2.1 mm, 5 μm) column (GL Science, Tokyo, Japan). The mobile phase was 10 mM ammonium acetate-acetonitrile (10:90 v/v) with a 0.3 ml/min flow-rate at 50°C. Hypoxanthine, xanthine and the corresponding internal standards were detected in multiple reaction monitoring negative mode. The mass transitions (m/z) monitored were 135→92 for hypoxanthine, 151→108 for xanthine, 139→95 for the internal standard for hypoxanthine and 153→109 for the internal standard for xanthine. The quantification range was 0.1 μg/ml to 1 mg/ml for both determinants.
Pharmacokinetics of febuxostat. Plasma concentrations of febuxostat were determined during the drug administration. Blood samples (5 ml) were taken before and 2 h after administration of the first dosing and at appropriate time points for measurement of trough drug levels from days 2-7. Serum concentrations of febuxostat were determined using the LC-MS/MS method (in preparation). Briefly, the sample was mixed with the internal standard (TEI-6720d3) and deproteinized by acetonitrile. The sample was then centrifuged and the supernatant was isolated and applied for LC-MS/MS. The quantification range was 4 to 4,000 ng/ml.
Statistical analyses. All statistical analyses were performed using the Microsoft Excel 2007 software (Microsoft, Redmond, WA, USA). All graphs were generated using the GraphPad Prism software (version 5.0) (GraphPad Software, Inc., San Diego, CA, USA).
Results
Patients. A total of 10 patients (4 males, 6 females; median age=67 years; age range=52-79 years) who were admitted to the University of Fukui Hospital between April and December of 2012, were enrolled in this study (Table I). All patients had hematological malignancies, such as leukemia and lymphoma, and underwent induction chemotherapy (Table I). All patients were classified into an intermediate-risk group of TLS; 6 patients had hyperuricemia (Table II).
Drug administration. Febuxostat was administered to all patients and the drug was continued for at least 7 days. Three patients received 60 mg of febuxostat, while 7 patients received 40 mg of febuxostat, according to the study protocol (Table II).
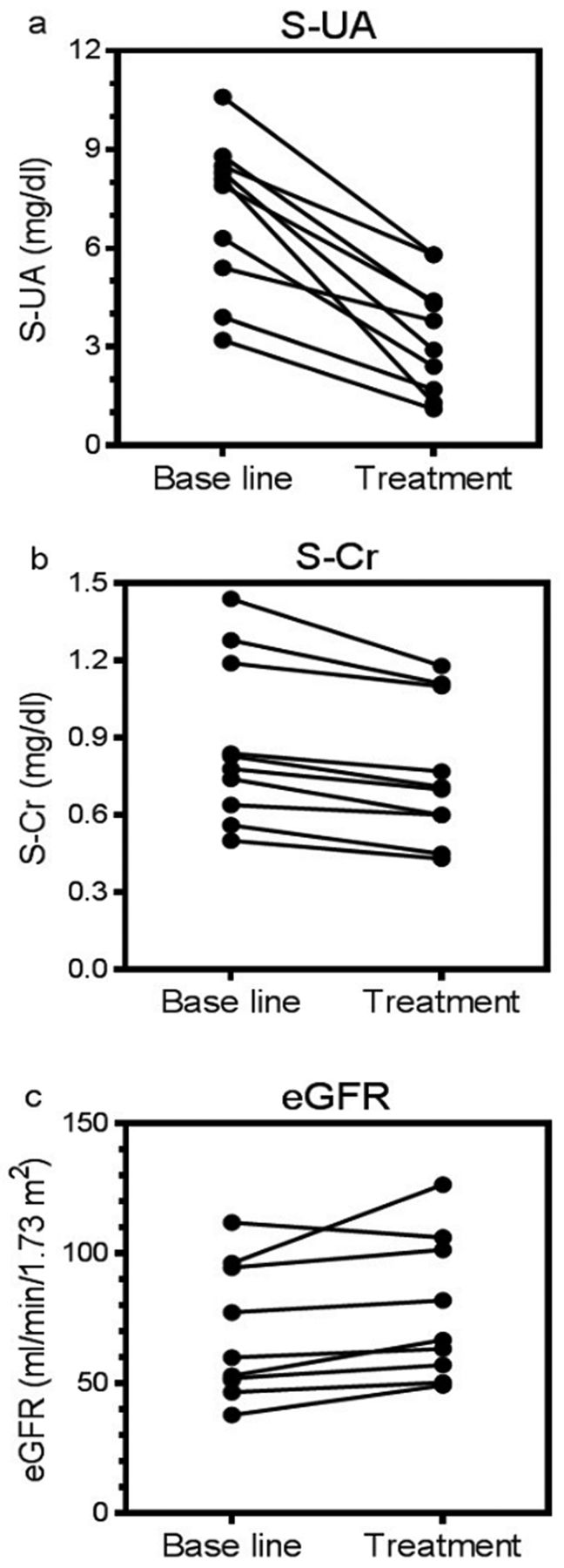
Time courses of S-UA and S-Cr. S-UA and S-Cr levels were monitored before and during the induction chemotherapy in all patients (Figure 1). Overall, S-UA levels differed among the patients but tended to decrease over time, although an increase in UA level was supposed by chemotherapy-induced tumor lysis. This supported the efficacy of febuxostat (Figure 1a). S-Cr levels decreased more slowly when compared to S-UA (Figure 1b), suggesting that renal function improved secondary to the reduction of S-UA levels and that febuxostat did not induce renal damage.
Therapeutic efficacy. The primary end-point of the present study was the S-UA maintenance or reduction to ≤7.5 mg/dl by day 5 of chemotherapy. Although the median S-UA at base-line was 8.0 mg/dl (range=3.2-10.6 mg/dl), the median S-UA on day 5 was 3.3 mg/dl (range=1.1-5.8 mg/dl) (p<0.0001, by paired t-test) (Figure 2a), indicating a successful control of S-UA during chemotherapy. The median S-Cr levels decreased from 0.81 mg/dl (range=0.5-1.44 mg/dl) to 0.72 mg/dl (range=0.57-1.35 mg/dl) (p<0.0003, by paired t-test) (Figure 2b). The median eGFR value increased from 56.4 ml/min (range=37.8-111.9 ml/min) to 66.7 ml/min (range=49.2-126.5 ml/min) (p=0.038, by paired t-test) (Figure 2c). These results, thus, suggested that febuxostat therapy resulted in successful control of S-UA and improvement in renal function.
Adverse events. The adverse events that occurred from the initiation of febuxostat until the 14th day of induction chemotherapy are summarized in Table III. Decreases in blood cell counts were reported but these hematological toxicities are more likely attributable to the concomitant administration of anticancer agents. The administration of chemotherapeutic agents might also be responsible for fatigue, nausea and loss of appetite. Grade 3/4 hepatic and renal dysfunction were not reported. None of the patients developed acute gout flares. Thus, these results suggested that no severe adverse reactions were noted in association with febuxostat administration.
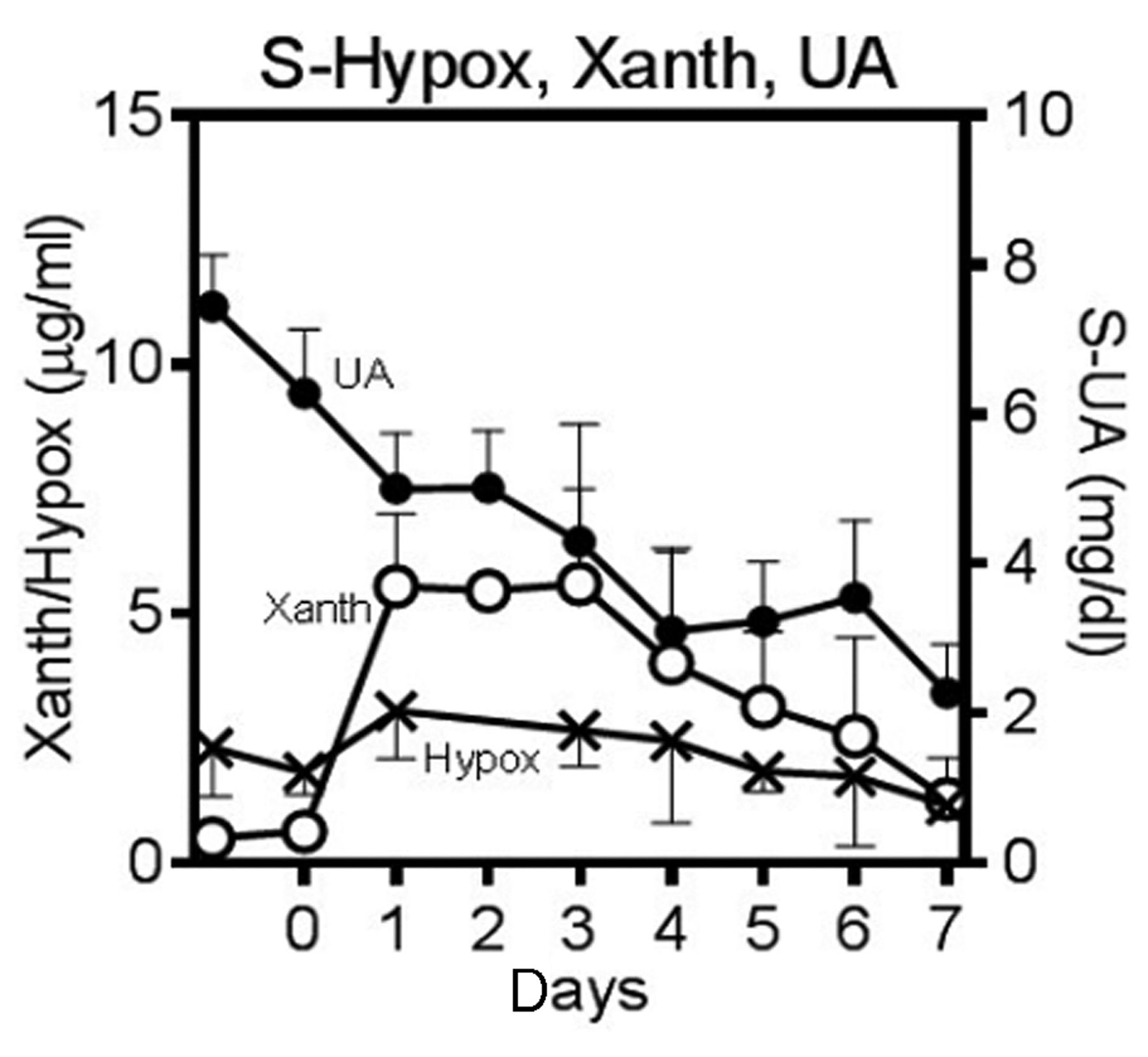
Measurement of levels of oxypurines (hypoxanthine and xanthine). Febuxostat and allopurinol are both xanthine oxidase inhibitors that inhibit the conversion of hypoxanthine to xanthine and inhibit the conversion of xanthine to UA. Figure 3 demonstrates the time courses of S-UA, serum hypoxanthine and serum xanthine. While S-UA decreased over time, serum hypoxanthine and xanthine concentrations increased on day 1 and persisted at these levels through day 4 (Figure 3), which might reflect the 2-step inhibition of the conversion of oxypurines to UA. Urinary UA concentration decreased over time (Figure 4a and 4d), a trend which might correspond with changes in S-UA. The serum and urinary hypoxanthine and xanthine concentrations increased on day 1, which resulted from the inhibition of xanthine oxidase by febuxostat (Figure 4). The mean±SE serum hypoxanthine and xanthine concentrations increased on day 1 (3.1±1.0 μg/ml and 5.6±1.5 μg/ml, respectively) and decreased on day 7 (1.2±0.4 μg/ml and 1.3±0.8 μg/ml, respectively) (Figures 4b and 4c). The mean±SE urinary hypoxanthine and xanthine concentrations increased on day 1 (94.3±31.0 μg/ml and 191.8±47.5 μg/ml, respectively) and decreased on day 7 (16.3±4.0 μg/ml and 58.5±12.1 μg/ml, respectively) (Figures 4e and 4f). The trends in hypoxanthine and xanthine were compatible with each other in both serum and urinary levels. Notably, when the ratio of concentration (day 1/day 7) was compared between hypoxanthine and xanthine, the higher value was observed in xanthine in both serum and urine, suggesting the second step of enzyme reaction, xanthine to UA, could be inhibited more potently compared to the first step, hypoxanthine to xanthine by febuxostat.
Pharmacokinetics of serum febuxostat. Serum febuxostat concentrations were determined before and 2 h after the first administration of the agent, and just prior to dosing (trough levels) on each day up to the 8th day. The estimated Cmax, the serum concentrations at 2 h after the first administration of febuxostat, which was the time of tmax in previous studies (27), were 891.8±285.0 ng/ml for the 40 mg dose of febuxostat and 770.6±242.7 ng/ml for the 60 mg dose of febuxostat (p=0.80, unpaired t-test) (Figure 5). The concentration-time curves suggested no drug accumulation during the treatment period for both doses (Figure 5). Table IV demonstrated the levels of S-UA, S-Cr and eGFR in association with serum febuxostat concentrations. The UA-lowering effects were comparable between the 2 doses, 40 mg and 60 mg.
Discussion
Due to the potential severity of TLS-related complications, prevention and/or early treatment of TLS is critical to improving outcomes in patients undergoing chemotherapy for cancer (4, 12). Since the incidence of TLS varies according to risk factors, TLS risk classification can identify patients who might need closer monitoring or use of prophylactic agents. Controlling S-UA levels is most important for prevention and treatment of TLS because hyperuricemia most often develops 48-72 h after the start of chemotherapy (28). According to published guidelines, hydration plus allopurinol is appropriate for patients at intermediate risk and hydration plus rasburicase is appropriate for patients at high risk (1, 2).
The present study was the first to evaluate the UA-lowering effect of a new, non-purine analog xanthine oxidase inhibitor, febuxostat, focused in cancer patients at an intermediate risk for TLS. Febuxostat is the recently approved UA-lowering agent; it was approved in the US in 2009, in Europe in 2010 and in Japan in 2011. By 2013, febuxostat was approved for use in 30 countries for the treatment of gout and hyperuricemia (18).
The present study clearly demonstrated that febuxostat successfully controlled S-UA in patients with hematological malignancies at intermediate risk of TLS. S-UA decreased over time after administration of febuxostat, and the treatment was considered successful according to criteria outlined in the present protocol (Figures 1 and 2). The successful control of S-UA was accompanied by a concomitant improvement in renal function. A recent multi-center phase III study by Cortes et al. compared UA in patients receiving rasburicase alone (0.20 mg/kg/day), rasburicase followed by allopurinol and allopurinol alone (300 mg daily) (23). The primary efficacy variable was the S-UA response rate, defined as the percentage of patients achieving or maintaining S-UA ≤7.5 mg/dl during days 3 to 7 (23). The S-UA response rate was 87% with rasburicase, 78% with rasburicase plus allopurinol and 66% with allopurinol. A randomized phase II study was conducted in Japan to compare between febuxostat and allopurinol for the treatment of gout and hyperuricemia (21). Patients were randomly assigned to receive a maintenance dose of 40 or 60 mg/day febuxostat or 300 mg/day allopurinol for 16 weeks. S-UA levels changed by -42.96% and -52.47% of base-line UA levels for the febuxostat 40- and 60-mg/day groups, respectively, and changed by -36.55% of base-line UA levels in the allopurinol group (21). Moreover, the percentage of patients who attained the target S-UA level (≤6.0 mg/dl) at 16 weeks was 88.9% and 100% for the febuxostat 40- and 60-mg/day groups, respectively, and was 68.8% for the allopurinol group (21). These data suggested that febuxostat at doses of 40 and 60 mg/day exhibited greater efficacy than did 300 mg/day allopurinol. Thus, despite the lack of a direct comparison between febuxostat and allopurinol for TLS, the present findings suggest that febuxostat is a promising agent for the management of TLS.

Time course of the mean S-UA (a) or S-Cr (b) concentrations during induction chemotherapy. S-UA and S-Cr concentrations were determined before the initiation of febuxostat and at days 0 to 7 of chemotherapy. S-UA, Serum uric acid; S-Cr, serum creatinine.
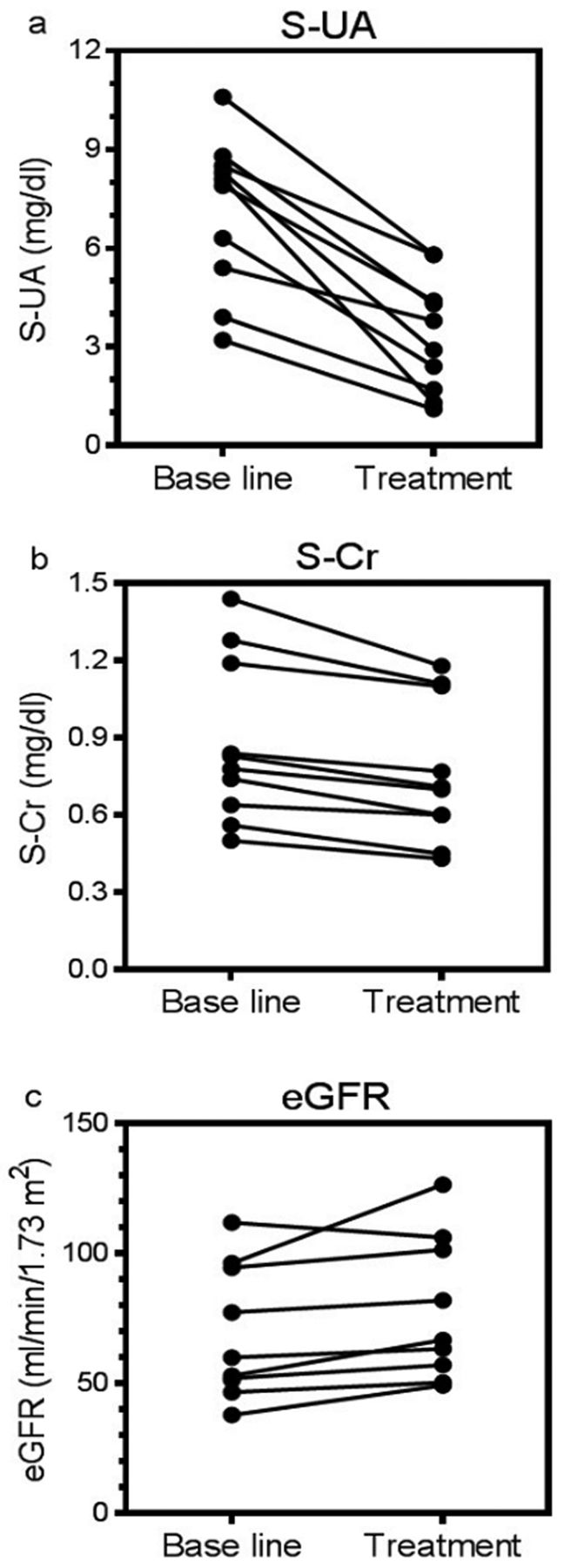
S-UA (a), S-Cr (b) and eGFR (c) levels at base-line and on day 5 of chemotherapy. S-UA, serum uric acid; S-Cr, Serum creatinine; eGFR, estimated glomerular filtration rate.
Patients' characteristics associated with tumor lysis syndrome.
The main adverse events were hematological toxicities (Table III) but these events might have been related to the chemotherapeutic agents rather than febuxostat. Adverse events, including hepatic dysfunction and skin toxicity, which could be considered to be specific to febuxostat, were not reported. In previous studies of gout patients, febuxostat-treated patients with a history of gout have higher rates of acute gout flares than those treated with allopurinol, and it has been suggested that this is due to the rapid reduction in S-UA levels, which induces mobilization of UA deposits (18). However, no acute gout flares occurred in the patients enrolled in this study. This suggested that the elevation in UA was acute or sub-acute rather than chronic in cancer-related hyperuricemia. In general in Japan, febuxostat is initiated at a dose of 10 mg and is gradually increased to 40-60 mg to avoid gout flares in patients with a history of gout. The present results suggest that the use of maintenance dosing (40-60 mg) of febuxostat is more appropriate than the use of the starting dose (10 mg) of febuxostat in patients at a risk of TLS. Such titration is not used in the US and Europe. Thus, the present study suggested that febuxostat was safely administered to cancer patients undergoing chemotherapy.

The time course of the mean concentrations of S-UA (●) and serum oxypurines (hypoxanthine [○], xanthine [×]). The values represent the means±SEs.
Allopurinol can also cause an increase in serum levels of the purine precursors, hypoxanthine and xanthine (1). Because of the lower solubility of xanthine in urine, there is the risk of xanthine crystal deposition in the renal tubules, which can result in acute obstructive uropathy. Hande et al. measured the urinary excretion of hypoxanthine, xanthine and UA in 11 patients with rapidly growing chemotherapy-sensitive lymphomas who were receiving concomitant allopurinol therapy (29). The mean maximal post-chemotherapy urinary concentrations of UA, hypoxanthine and xanthine were 288, 115 and 179 μg/ml, respectively (29). The solubility of hypoxanthine in urine is 1,400 μg/ml at pH 5 and 1,500 μg/ml at pH 7, while the solubility of xanthine in urine is 50 μg/ml at pH 5 and 150 μg/ml at pH 7 (29). In the present study the urinary xanthine concentrations on day 1 (191.8±47.5 μg/ml) was comparable to the solubility limit of xanthine (Figure 4). Therefore, urinary excretion level of xanthine could conceivably exceed reported concentrations associated with xanthine nephropathy. However, as shown in Figures 1 and 2, no progress of renal impairment was observed in our cases, suggesting the possibility that the increased level of serum and urinary concentration of xanthine for short-term might not cause severe nephrotoxic action, as reported previously. Thus, careful observation and management, as well as re-evaluation should be required for this issue in the patients whose xanthine levels are elevated but UA levels are well controlled.
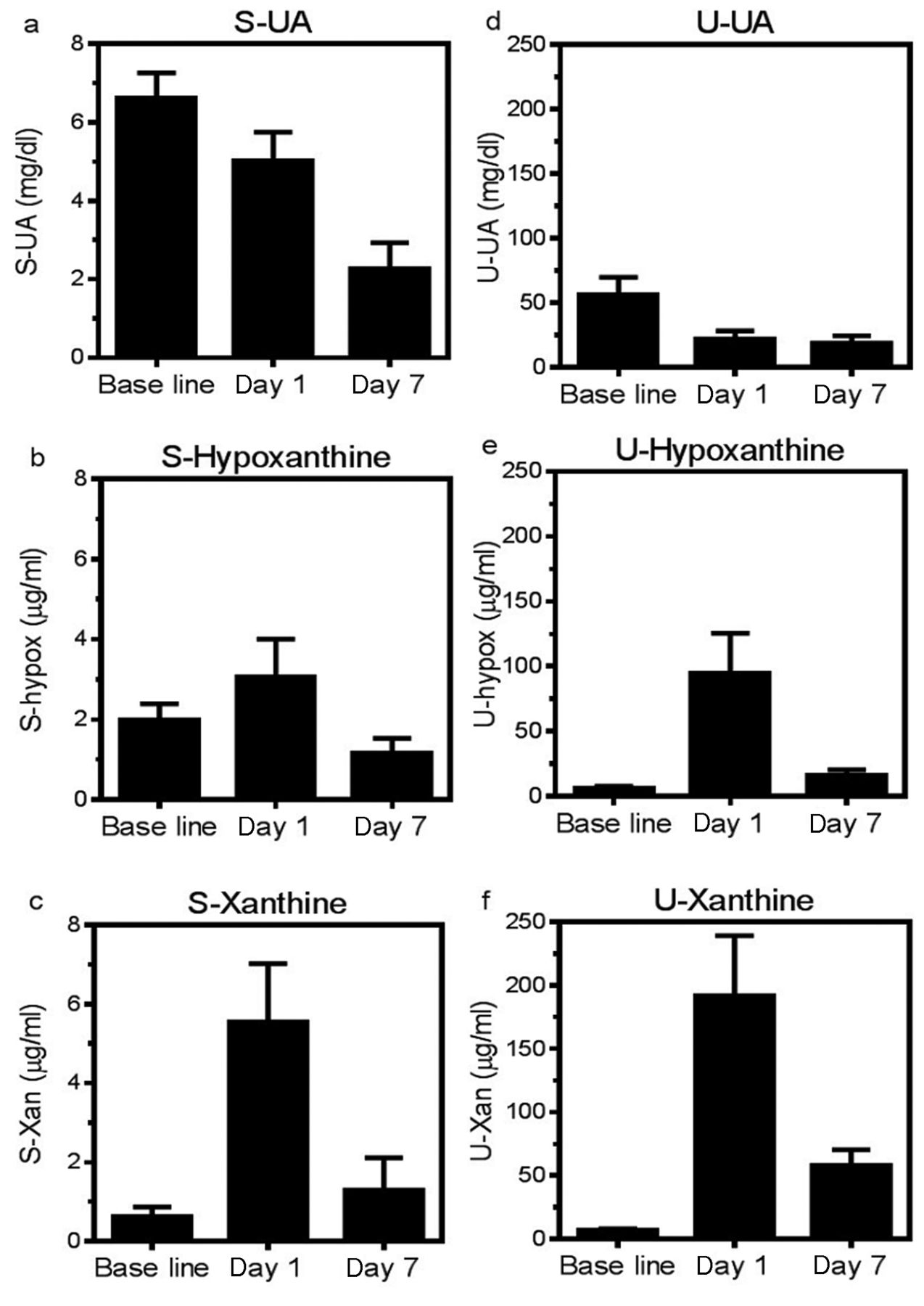
Concentrations of urinary UA (b), urinary hypoxanthine (c) and urinary xanthine (d) at base-line and on days 1 and 7 of chemotherapy. S-UA, serum uric acid; Hypox, hypoxanthine; Xan, xanthine; U-UA, urinary uric acid. The values represent the means±SEs.
Adverse events.
Parameters according to the dose of febuxostat.

The concentration-time curve of serum febuxostat in patients receiving a 40 mg (×) or 60 mg (○) dose. The concentrations of febuxostat were measured using the LC-MS/MS method.
Khosravan et al. reported that febuxostat concentrations were between 1,000 ng/ml and 3,440 ng/ml at the tmax of 1.8-2.3 h when the agent was administered at doses between 40 mg and 120 mg (27). The concentration fell to the trough level between10 ng/ml and 100 ng/ml at 24 h after administration. Another study by Khosravan et al. demonstrated that the Cmax of febuxostat was dose-proportional across the doses between 10-240 mg (30). Zhang et al. also reported the dose-dependent increase in the Cmax in healthy subjects who received febuxostat at doses of 40 mg, 80 mg and 120 mg (31). In another study of healthy volunteers, after oral administration of 40 mg or 80 mg of febuxostat, the Cmax values were 2,270.3±866.7 ng/ml 3,765.3±1,008.3 ng/ml, respectively (Feburic tablets™, Interview form, August, 2012, Teijin Pharma, Ltd, Tokyo, Japan). Several studies have examined the effects of renal impairment on the pharmacokinetics and pharmacodynamics of febuxostat. Hoshide et al. reported less than a 2-fold difference in the area under the curve value of plasma unchanged febuxostat with either normal, mild (creatinine clearance 50-80 ml/min) or moderate (creatinine clearance 30-50 ml/min) renal impairment who were administered a single dose of febuxostat 20 mg (32). Mayer et al. investigated pharmacokinetics and pharmacodynamics of febuxostat in subjects with normal renal function or renal impairment who received febuxostat (80 mg/day) orally for 7 days (33). The Cmax values of unbound febuxostat were 2,860 [1,250] μg/ml (mean [SD]) in patients with normal renal function, 4,030 [1,690] μg/ml in patients with mild renal impairment and 2,920 [1,060] μg/ml in patients with moderate renal impairment (33). The area under the curve values of unbound febuxostat were 7,502 [2,680] (ng·h/ml) (mean [SD]) in patients with normal renal function, 11,135 [1,356] (ng·h/ml) in patients with mild renal impairment and 11,130 [2,924] (ng·h/ml) in patients with moderate renal impairment (33). Upon administration of 20 mg febuxostat, the Cmax values were 495.6 [157.6] ng/ml in patients with normal renal function, 504.1 [146.5] ng/ml in patients with mild renal impairment and 621.8 [270.9] ng/ml in patients with moderate renal impairment (Feburic tablets™, Interview form, August, 2012, Teijin Pharma, Ltd, Tokyo, Japan). In the present study, the dose of febuxostat was reduced in patients with renal dysfunction and the pharmacokinetic determinants were comparable between the 2 does, 40 mg and 60 mg (Figure 5). Previous studies have demonstrated that pharmacokinetic difference by renal function appears to be of little clinical importance because renal impairment did not markedly reduce the effects of febuxostat on S-UA levels (32-34). Therefore, further investigations are required to elucidate the necessity of dose adjustment of febuxostat by renal function for the management of TLS.
In conclusion, the present study demonstrated that febuxostat was effective for controlling S-UA without major adverse reactions in cancer patients at an intermediate risk for TLS. A careful observation and re-evaluation should be performed about the possibility of xanthine nephropathy. This study was performed in a single institution with a small number of patients. Nevertheless, it was suggested that febuxostat would be a promising alternative to allopurinol for the management of TLS. Multi-institutional prospective trials are now undergoing.
Acknowledgements
This work was supported in part by Grants from the Gout Research Foundation (2011, 2012).
Footnotes
-
Clinical trial register: This study was registered at http://www.umin.ac.jp/ctrj/ (UMIN000007538).
-
Conflicts of Interest
The following Author indicated a financial interest that is relevant to the subject matter under consideration in this article. Takanori Ueda received funding from Teijin Pharma, Ltd.
- Received August 2, 2014.
- Revision received September 11, 2014.
- Accepted September 18, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}