


Abstract
Aim: Breast cancer can be divided into four subtypes: luminal-A, luminal-B, HER-2 enriched and triple negative breast cancer (TNBC) by the presence or absence of receptors. Each subtype has a typical clinical behavior and prognosis. Many chemotherapeutic agents are used clinically for breast cancer. The histoculture drug response assay (HDRA) is used for selection of effective chemotherapeutic agents for individual patients Materials and Methods: In the present study, the HDRA was used for eleven frequently-used single-agent or combinations on the four subtypes of breast cancer in order to determine the correlation of drug sensitivity profile and breast-cancer subtype. Fifty invasive ductal breast carcinoma patients who underwent cancer surgery and adjuvant chemotherapy between January 2012 and January 2013 had their tumors analyzed in the HDRA. Age, gender, height and weight, tumor-nodes-metastasis (TNM) stage, immunohistochemical (IHC profiles, breast-cancer subtypes and HDRA results were recorded. Results: The inhibition rate (IR) of each agent or combination for each breast-cancer subtype was determined. Drug to drug IRs were statistically distinct in all subtypes (p<0.05) but no correlation between response to chemotherapeutic agents and breast-cancer subtype was found (p=0.851 by two-way ANOVA test). Conclusion: The clear difference between average sensitivity of the chemotherapeutic agents tested and lack of correlation with breast-cancer subtype suggest the importance of individualized treatment for breast-cancer patients.
- Histoculture drug response assay
- HDRA
- chemotherapeutic agents
- inhibition rate (IR)
- correlation
- breast cancer
- subtype
- estrogen receptor
- progesterone receptor
- HER-2
- individualized therapy
Breast cancers are clinically heterogeneous and tend to have different clinical courses even if they are of the same stage (1). Breast cancer has been classified into four subtypes: luminal A, luminal B, HER-2 enriched and triple negative breast cancer (TNBC) depending on the presence or absence of estrogen/progesterone receptors (ER/RP) or HER-2 (Table I) (2). Clinical selection of chemotherapeutic agents usually depends on the size of the primary tumor, the presence of axillary lymph node metastasis and distant metastasis, all of which greatly influence the prognosis of the patient. Adverse reactions associated with most of chemotherapeutic agents, due to cytotoxicity, have promoted efforts to find optimum chemotherapy with minimum side effects using in vitro chemosensitivity assays (3, 4). Chemosensitivity assays can be divided into either two-dimensional culture or three-dimensional culture. Although two-dimensional cell culture may be more convenient (5), it lacks tumor-stromal interaction within intact tumor tissue, which is more representative of the patient's tumor in vivo (4, 5). The histoculture drug response assay (HDRA) uses three-dimensional tumor tissue culture and has been shown to have high clinical correlation for gastrointestinal GI cancer (6, 7), head and neck cancer (8) and ovarian cancer (9). The effectiveness of the HDRA in breast cancer has been demonstrated (10, 11).
There have been reports that Luminal B-type patients have had a better response, compared to luminal A types, to docetaxel. Preoperative chemotherapy (neo-adjuvant) of the HER-2 enriched type of breast cancer has had a reported better response to doxorubicin-docetaxel (12, 13).
The present study correlates chemotherapy sensitivity with the HDRA for eleven frequently-used single agents alone or in combination for the four subtypes of breast cancer.
Patients and Methods
Patients. Fifty breast cancer patients were operated at the KangNam Sacred Heart Hospital from January 2012 to January 2013. Each patient had invasive ductal carcinoma. Patients had breast conservation surgery or radical mastectomy with ipsilateral axillary lymph node dissection. The primary tumors were immunohistochemically analyzed and the breast cancer subtype was determined based on the results. The study was approved by the Institutional Review Board of the KangNam Sacred Heart Hospital, Hallym University Medical Center.
Immunohistochemical staining. Immunohistochemical analysis was conducted for the estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor-2 (HER-2). The results were semi-quantitatively expressed. For ER and PR, the tumor was judged as positive if the staining covered more than 10% of the nucleus or the cell membrane. HER-2 was judged as positive if the immunohistochemical staining was 3+ and the fluorescence in situ hybridization (FISH) was used to determine positivity if immunohistochemical staining was 2+.
HDRA. The HDRA cultures tumors in three dimensions on Gelfoam®. 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) was used for determining drug response (6, 10). Primary tumors >150 mg are placed in Hank's balanced salt solution (HBSS) and sliced into fragments (0.5-1 mm in diameter) and placed on Gelfoam® for one day. On day-2, the tumors were further cultured with either single or combination chemotherapeutic agents including: A+Cx (doxorubicin and cyclophosphamide), Txl (paclitaxel), G+N (gemcitabine and vinorelbine), E+DTx (epirubicin and docetaxel), A+DTx (doxorubicin and docetaxel), Cx+E (cyclophosphamide and epirubicin), CP+Txl (cisplatinum and paclitaxel), XEL (capecitabine), CbP+Txl (carboplatinum and paclitaxel), DTx+XEL (docetaxel and capecitabine) and DTx (docetaxel) for 72 hours. After removing the culture medium, HBSS (100 μl) and collagenase (0.1 mg/ml) and MTT (100 μl) dissolved in PBS (5 mg/ml) were pipetted into each culture well with incubation for four hours at 37°C. After removing the fluid, each well was treated with dimethyl sulfoxide (0.5 ml). The resulting formazan crystal was extracted and the absorbance was detected with a spectrophometer. Using the measured absorbance, the inhibition rate (IR) is calculated by the formula:

T=Absorbance of the specimen treated with a chemotherapeutic agent(s)
C=Absorbance of the control treated with PBS
Sensitivity of the tumor is scored if the IR exceeds 30%.
Breast-cancer subtype definitions.
Statistical analysis. The SPSS 13.0 program (SPSS Inc., Chicago, IL, USA) was used. The Student's t-test or the least-squares deviation verification was used to determine each breast cancer subtype sensitivity to each single or combination chemotherapeutic agents. In order to determine whether the IR of single or combination chemotherapy has a different pattern for each subtype, the one way-ANOVA test, the Fisher exact and the Pearson chi square test were used. Statistical significance was determined if the p-value is below 0.05.
Results
Patients. The average age of the patients was 48.54 with a range of from 24 to 87 years. The staging distribution was as follows: 18 patients (36%) had stage I; 17 patients (34%) had stage IIa; 8 patients (16%) had stage IIb; 7 patients (14%) had stage IIIa. There were no patients with stage IIIb or over (Table II).
Immunohistochemical staining identified 37 ER-positive patients (74%); 32 PR-positive patients (64%); 15 HER-2-positive patients (30%) and 8 TNBC patients (16%) (Table III). Based on the immunohistochemical study results, the breast cancer patients were classified into four subtypes. Luminal A type was most frequent with 27 patients (54%) (Table IV).
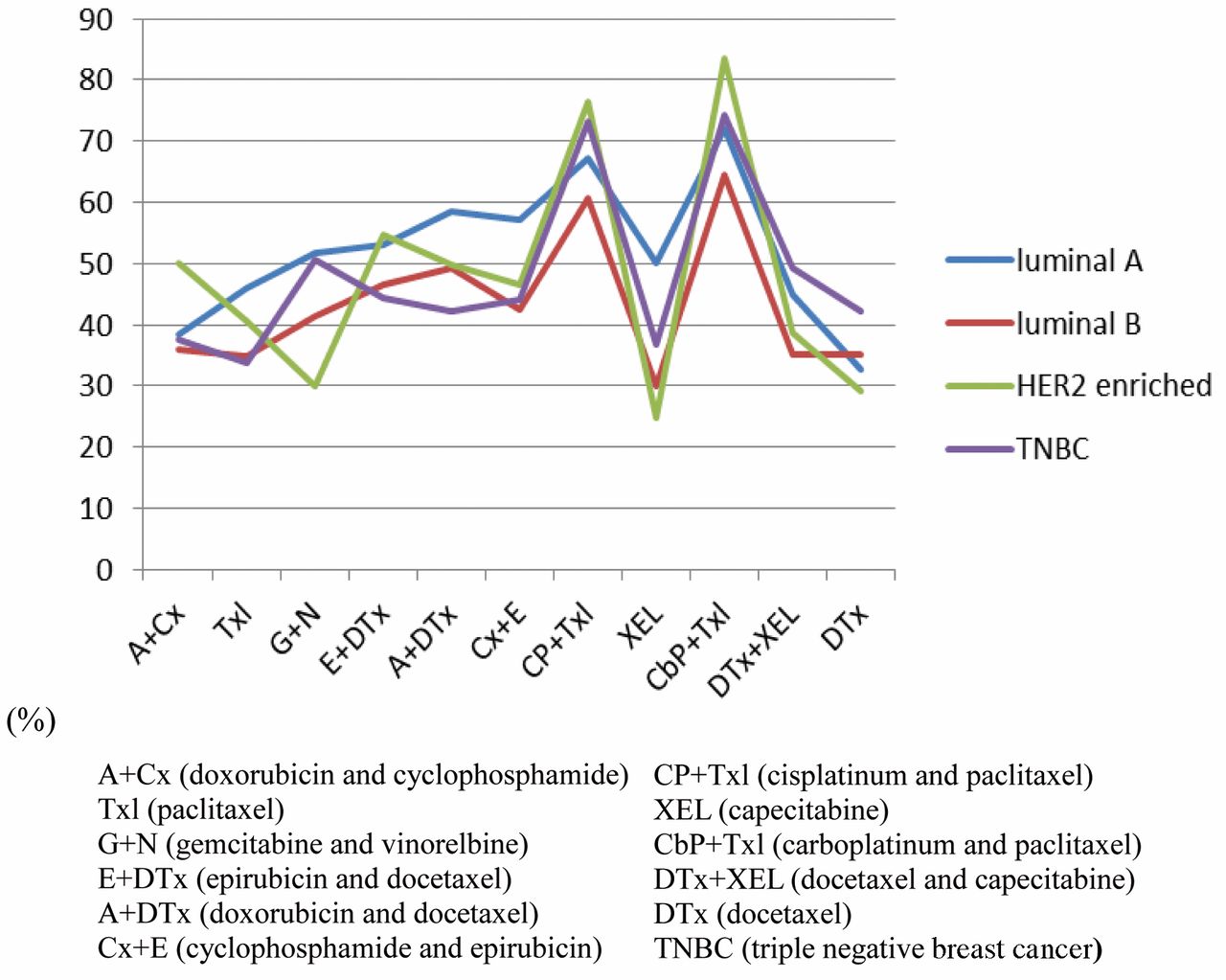
After the subtype was determined for each patient, the HDRA was conducted and the average of the IR of each chemotherapeutic agent was calculated for each subtype (Table V and Figure 1).
Combination chemotherapy of CP+Txl and CbP+Txl had the highest sensitivity (66% and 70%, respectively) (Figure 1). The two-way ANOVA test shows that the IR of each of the single agents or combination chemotherapies is statistically different (p<0.05). However, the one-way ANOVA test demonstrates no significant correlation between IR of any agent or combination with breast cancer subtype (p=0.851).
Discussion
Breast cancers are clinically heterogeneous and the patients tend to have different clinical courses even if they have the same stage or the same histological characteristics (1). The responsiveness of each breast cancer subtype to various chemotherapeutic agents has been reported (12-15). However, such studies emphasize the empirical selection of chemotherapeutic agents. The predictivity of the HDRA for many cancer types has been established (6-9).

Mean inhibition rate by subtypes.
Patient age and stage.
The HDRA three-dimensionally histocultures the cancer tissues on a collagen sponge (Gelfoam®) which provides an in vivo-like environment (16). The tumor grows structurally resembling the in vivo tumor and it should generate more accurate results compared to chemosensitivity tests using two-dimensional cell culture.
The present study classified breast cancer into four major subtypes and analyzed the IR for eleven frequently-used single or combination cytotoxic chemotherapy agents on each subtype. Each single agent or each combination chemotherapy had a statistically-different IR (p<0.05). However, the distribution of IRs was similar when comparing the average chemosensitivity for each breast cancer subtype (Figure 1) (p=0.851). Therefore, the study demonstrates that the efficacy of a chemotherapeutic agent depends on the individual tumor rather than the breast cancer subtype. Future experiments will correlate the response in the HDRA and individual breast cancer patients of each subtype. Such experiments should further demonstrate the need for individualized drug testing of breast cancer patient tumors in order to design rational effective therapy for the patient.
Immunohistochemical staining results.
Breast cancer patient subtype distribution.
Mean inhibition rate (IR) of chemotherapy drugs by breast cancer subtype (%).
- Received September 11, 2014.
- Revision received October 1, 2014.
- Accepted October 7, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}