


Abstract
Background/Aim: During the treatment of head and neck cancer (HNC), salivary problems may impair a patient's healing process. Botulinum toxin (BoNT) is accepted as an effective treatment option for reducing salivary flow. We aimed to describe the features of patients treated with BoNT to determine the effects of BoNT. Patients and Methods: Twenty-five patients over a five-year period were retrospectively included. The patients suffered at different stages of oncologic treatment. The cohort primarily had larger primary tumors that required complex oncological treatment. Results: The condition improved in more than three quarters of the 19 patients with functional hypersalivation. Four of six cases suffering from a salivary fistula demonstrated an obvious reduction in symptoms. Conclusions: Injection of BoNT, to temporarily reduce saliva flow, is a safe tool in the treatment of HNC even in situations involving repeated therapy or high dosage. The main clinical side-effect of BoNT is insufficient reduction of the salivary problem.
Surgeons, radiotherapists and oncologists frequently encounter saliva-associated problems in patients with head and neck cancer (HNC). Such situations may occur before, during or at different stages following any oncological treatment. Swallowing difficulties in HNC patients are not unusual because the disease and its treatment often compromise the meticulous coordination of bolus control and breathing. Therefore, hyper-salivation is not the primary issue; the main problem is the control of saliva swallowing (1, 2). In many cases, modern radiotherapy (3) can preserve salivary gland function, whereas previous treatments would have caused severe xerostomia. As problems with salivary control, such as functional hypersalivation, are part of underlying dysphagia (2), hyper-salivation is considered a presentation of dysphagia. The second main saliva problem for such patients is the occurrence of various fistulae during malignancy or after surgical interventions. In these cases, a reduction in saliva flow is required because the aggressiveness of saliva is believed to be a major contributor to poor wound healing (4, 5).
The following are indications for the use of botulinum toxin (BoNT) in the treatment of HNC patients: gustatory sweating after parotidectomy, postlaryngectomy voice and swallowing disorders, spasm in muscular flaps, post-radiation neck pain and salivary disorders (e.g., hypersalivation or fistula treatment) (6, 7). The use of BoNT in HNC patients is often very specific and is always an off-label use of BoNT. Furthermore, the use of BoNT has only been documented in individual cases of HNC patients.
The aim of the present work was to investigate the efficacy of BoNT therapy in HNC patients with salivary disorders at a university level ear nose and throat (ENT) hospital. The indication, safety and efficacy of BoNT therapy in HNC are highlighted.
Patients and Methods
A consecutive cohort of 25 patients visiting a single university hospital between August 2008 and March 2013 was used for the retrospective assessment. These patients suffered from saliva-associated difficulties at different stages of oncological treatment for HNC (Figure 1). Radiotherapy had already been completed in 12 of the 25 cases and the salivary problem occurred during cancer recurrence in eight of the cases. The T stage of patients' primary tumor size varied between 2 and 4 but all patients except one were classified Union Internationale Contre le Cance (UICC) stage IV (Figure 2). The surgical aspect of the oncological treatment was complex in most cases, reflecting the high rates of flap-closure (11/25), (temporary) tracheostomies (21/25), bilateral neck dissections (13/25) and interstitial brachytherapy at the time of tumour surgery (5/25). In this retrospective case series, only patients receiving BoNT treatment for their salivary problems were included. Patients with gustatory sweating (Frey's syndrome) were excluded from this analysis. In 19 patients, the salivary problem was dominated by swallowing difficulties caused by functional hypersalivation. Six patients had a pharyngocutaneous fistula and continuous saliva flow caused by the irregularity (Table I).
Demographic and clinical aspects of patients suffering from a salivary fistula.
The criteria for treatment with BoNT injections were lack of improvement with either with anti-edematous medication or swallowing therapy that was designed to activate compensation mechanisms (2) (Figure 3). In some patients, constant salivary flow and aspiration required cuffed tracheostomy tubes, which made the tracheostoma closure or the use of a speech cannula impossible (Figures 4 and 5). Most patients treated intravenously with glycopyrrolate two to three times daily had decreased saliva production. However, intravenous glycopyrrolate therapy is not possible as an outpatient treatment and is not an option for patients who suffer from anticholinergic side effects of glycopyrrolate, which include symptomatic transitory psychotic syndrome. Scopolamine patches are rarely used at our institution due to the previously mentioned side effects, a high rate of blurred vision, intolerable sedation and poor dosage management. Prior to BoNT therapy, patients were counselled on the treatment options for hypersalivation, the off-label-use of most medical interventions and the possible adverse effects. BoNT injection was administered under ultrasound guidance with topical anaesthesia with Xylocain® gel and ultrathin 27-gauge needles. The injection of 0.9% saline was approximately 0.5 to 1 ml per gland. For the glandula parotis,the treatment was distributed between two or three smaller injection points. All three BoNT type-A medical products available in Germany were used; 20 units for each submandibular gland and 30 units for each parotideal gland for Botox® (Allergan, 76275 Ettlingen, Germany) or Xeomin® (Merz, 60318 Frankfurt am Main, Germany) and 50 units (submandibular) and 70 units (parotideal) of Dysport® (Ipsen, 76275 Ettlingen, Germany). This initial standard dosage was modified when the submandibular glands had been removed (such as during oral cancer neck dissection) and was further increased in cases displaying insufficient effects (Figure 6). The treatment effect was documented after approximately ten days using an ordinal scale of no change, slightly improved or improved.
Results
In the six cases of pharyngocutaneous fistula, all patients showed reduced salivary flow and there was a relevant improvement in two thirds of the patients. Of the patients in the group suffering from (functional) hypersalivation, 11/19 patients improved, in 4/19 slightly improved and no change was observed in 2/19. Due to loss of follow-up in 2/19 cases, the effect of treatment could not be evaluated. There were 17 repeated injections in seven patients, which were administered after the effects of the first treatment diminished; these repeat injections were usually administered after approximately ten weeks (8 to 20 weeks). In summary, apart from some small hematomas, which appeared under current anti-coagulative medication, there were no serious side-effects (severe bleedings, facial nerve injury, antibody provocation or allergic reactions) from the 42 treatments administered to the 25 patients.
Case report. A 71-year-old male presented with severe aseptic radionecrosis of the cervical spine (Figure 6). Fourteen years prior, he underwent a laryngectomy with jejunum interponate as pharyngeal-esophageal reconstruction and adjuvant radiotherapy. After emergency spinal cord stabilization with external fixation, repeated anterior-lateral approaches for re-fixation were required. Due to infection and healing problems in the emaciated patient, the ventral circumference of the neopharynx dissolved. An enormous pharyngocutaneous fistula with eminent salivary flow to open neck wounds aggravated the situation. In January 2011, 500 units of Dysport® (Ipsen) were injected. This treatment decreased salivary flow to a minor level and facilitated wound care management. After the effect of injection had diminished in May 2011, 100 units of Dysport® per submandibular gland and 150 units into each parotis were administered. After another increase in salivary flow to the shrunken fistula, 70 and 180 units, respectively, were successfully injected in August 2011. The patient died in September 2011 due to pneumonia and acute respiratory failure.
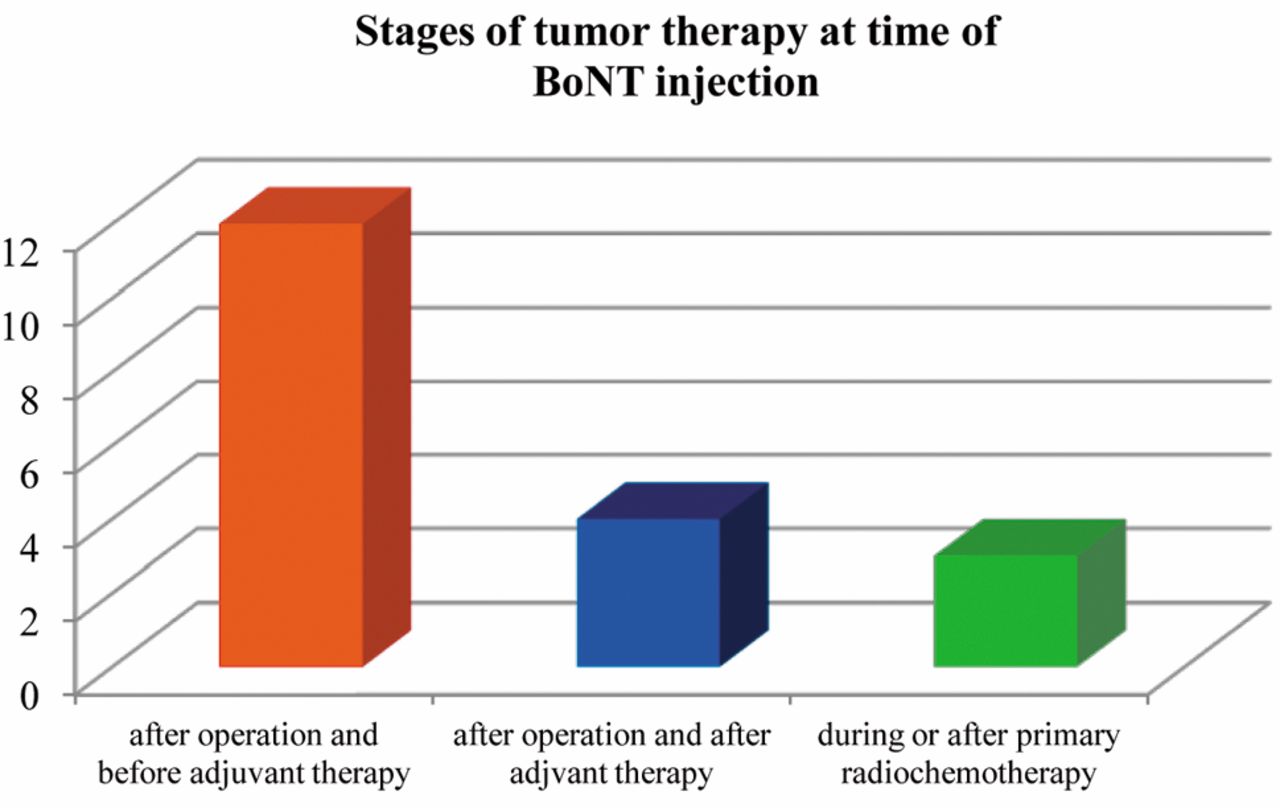
Therapy stages of the 19 patients at the time of BoNT injection due to hypersalivation.

T stage of the patients included for BoNT treatment.

Clear pooling of saliva in the neopharynx due to significant esophageal stenosis in a 65-year-old male patient who received a laryngectomy, bilateral neck dissection and adjuvant radiotherapy for laryngeal cancer in 1982. He suffered from hypersalivation after a tongue base cancer in 2008, followed by primary radiochemotherapy.

A patient with cuffed tracheostomy tubes due to saliva aspiration and dysphagia.

Clear signs of poor healing because of the constant saliva flow via the tracheostoma.
Discussion
In the last 15 years, a growing number of authors have described the impressive effects of BoNT in reducing functional hyper-salivation. Most reports have focused on patients with such neurodegenerative diseases as Parkinson's or on children with cerebral palsy. Reports investigating BoNT treatment for HNC are mainly of individual cases (8, 9) and very few cohort studies exist (10). In the present study, we present a large variety of head and neck tumors occurring at different junctures of HNC. We show that, even with repeated administration at a high dosage, BoNT is an effective and safe tool for reducing salivary problems in patients suffering from severe cancer. Most of patients in this study had high tumor stages and were elderly; one third suffered from recurrent disease. The surgical tumor therapy that patients received was usually complex and included a high rate of tissue transfer, tracheostoma or interstitial brachytherapy. These treatments severely impaired their ability to control the swallowing of saliva.
The following are the advantages of BoNT treatment: effects lasting for several weeks, relatively simple administration by a surgeon accustomed to ultrasound, good modulation of the individual dosage in response to the observed effects and hardly any systematic interactions with the medications currently prescribed to elderly HNC patients. The anti-cholinergic side-effects of previously used substances can be avoided. In contrast with other drugs, BoNT does not require ongoing patient compliance or multiple daily intakes. The main unforeseen consequence of BoNT injections used to treat functional hypersalivation in our series was little or no reduction of the salivary flow. Although this unforeseen consequence may have been due to the ineffective placement of submandibular injections in patients with heavy radioedema, despite the use of ultrasound, it is more likely the result of a too low administered dose in the first injection. A base rate of approximately 10% ineffectiveness was reported in previous larger case studies of hypersalivation treatment with BoNT (11), which is consistent with our study. In contrast to patients with hypersalivation caused by neurodegenerative diseases, such as Morbus Parkinson or cerebral palsy, most of our patients required only a single treatment. In post-surgical situations, dysphagia improved in most patients before the pharmacological effect of BoNT ended. The treatment effect outlasted the cancer treatment period in some (palliative) patients; in such cases, the long-lasting effect of BoNT did not result in sedation, which is a problem with systemic anti-cholinergic treatment. In some patients with a tracheal cannula, the combined saliva reduction treatment of glycopyrrolate and BoNT resulted in a very thick pharyngeal secretion that complicated cannula hygiene. Considering this clinical phenomenon in cannula patients in mind, we chose a lower-dose regime during the first injection and administered a second injection if the saliva reduction was insufficient. A short time interval between the BoNT injections correlated with a higher rate of antibody development (12). Hypersalivation in HNC patients differs from that in patients with other neurological diseases. Dysphagia issues are normally short-term in HNC patients; thus, as mentioned previously, in many cases, only a single treatment is necessary, which reduces the risk of antibody development. Therefore, we would not hesitate to use shorter intervals between BoNT injections to achieve good saliva reduction without causing the thick secretion that obstructs the cannula. Additionally, in several patients, dysphagia interfered with decannulation and tracheostoma closure during post-cancer treatment. Often, only less intensive swallowing therapy programs can be used because of ongoing saliva aspiration. In this study, the patients benefited from improved quality of life after a good response to the BoNT injection because they no longer required a tracheal cannula or, at least, could use a speech cannula.

Sagittal MRI of a patient with severe cervical spine radionecrosis.
The situation for patients with a pharyngeal fistula is even more complex. In addition to residual cancer, infections, low immune defense capacity and other risk factors during the healing of head and neck cancer, saliva leakage prolongs fistula closure (3). Patients are usually on multiple medications and, as a result, systemic anti-cholinergic drugs for saliva reduction have a high risk of pharmacological interference. One advantage of locally acting BoNT injections is that they minimize drug side effects or interference. Even at high dose BoNT application appears to be safe, as long as aspiration tests and ultrasound guidance are used to avoid intravascular injections (Figure 5). In conclusion, although BoNT injections in complex cases are relatively costly and the response for some patients can initially be limited, BoNT treatment is very low risk and has very few side effects.
The cohort in this study included a broad array of different tumor sites, cancer treatments and therapy stages. Although the five-year observation period is relatively long, a better balanced multicenter study with more patient groups is required to devise appropriate dosage regimes and answer the remaining questions. The main indication for treatment with BoNT in this study was too much saliva and the potential need for longer-term saliva reduction. Patients were also offered BoNT treatment when anticholinergic drugs could not be tolerated or were not an option because of comorbidities or when swallowing therapy, especially in tracheal cannula cases, showed little progress or was suspended due to the risk of saliva aspiration.
The quantitative assessment of hypersalivation is problematic, as noted in previous research (13), and there have been no recent advances in the methods for measuring hypersalivation. As a result, the evaluation of patients with hypersalivation is mainly based on questionnaires, such as the Drooling Severity and Frequency Scale (DSFS), established by Thomas-Stonell (14) and Crysdale (15). Another measurement method, especially for dysphagia in patients with a tracheal cannula, is the Bogenhausener dysphagia score (BODS-1/-2) (16), a disadvantage of which is that the ordinal items are not applicable in everyday use outside of specific dysphagia departments. The use of DSFS or BODS in this cohort was difficult because neither questionnaire sufficiently documents the problems associated with a salivary fistula. As a result, we used a simple three-point ordinal scale. Although this is a self-designed and non-validated measurement, which makes the assessment of success subjective, we could not teach a more reliable approach. This is an area that should be improved in future with research. The most recently reported studies cannot be compared because of differences in the initial hypersalivation severity and changes during treatment, different treatment modalities and dosage regimes, as well as differences in underlying diseases. There are initial reports that BoNT can prevent xerostomia after radiotherapy in HNC patients (17), considering the hypothesis that there is less tissue damage in the radiation field, with a reduced state of activity. The promising results reported by Corradino (10) showing fewer complications in microsurgical reconstruction of oral cancer after preoperative BoNT injections and provide additional evidence favoring early saliva-reducing treatment.
In conclusion, BoNT therapy offers HNC patients a new low-risk option for improved surgical recovery that may provide patients, especially tracheal cannula patients, with a better quality of life and reduce costs due to shorter hospital stays. The main clinical side-effect of the BoNT treatment is insufficient reduction of the salivary problem. When treating a fistula, BoNT treatment represents only one aspect in the entire treatment approach.
Footnotes
-
Presented at the 84th Annual meeting of the German Society of Otorhinolaryngology, Head Neck Surgery in Nuremberg, May 10th, 2013.
- Received June 27, 2014.
- Revision received July 25, 2014.
- Accepted August 4, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.