


Abstract
Aim: To evaluate the results of postoperative radiotherapy (PORT) and to identify prognostic factors for gallbladder cancer (GBC). Patients and Methods: We retrospectively analyzed 86 patients with GBC who underwent potentially curative surgical resection and PORT between November 1993 and December 2009. All patients received three-dimensional conformal radiotherapy and 61 patients (71%) had concurrent chemotherapy. Survival outcomes including locoregional control (LRC), disease-free survival (DFS) and overall survival (OS) rates were analyzed. Results: The median follow-up period was 83 months for surviving patients. The 5-year OS, DFS and LRC rates were 42%, 36% and 73%, respectively. Isolated locoregional recurrence as first failure occurred in seven patients (8%). On multivariate analysis, the postoperative carbohydrate antigen 19-9 (CA 19-9) level was a significant prognostic factor for LRC, DFS and OS. Conclusion: Adjuvant radiotherapy might be an effective treatment in terms of LRC in GBC. Postoperative CA 19-9 might be useful as a surrogate marker for survival.
Gallbladder cancer (GBC) is a relatively rare disease and most patients are diagnosed at advanced stages (1-5). The gallbladder wall lacks a submucosa layer and on the side of the liver it lacks the serosa layer. Because of the thin wall of the gallbladder, GBC easily invades into the liver and other adjacent organs and shows early extension to lymphatics. Autopsy data show that the incidence of lymphatic and hematogenous metastases ranges from 91% to 94% and 65% to 82%, respectively (6, 7).
Complete surgical resection is the standard treatment for GBC and the 5-year overall survival (OS) rate in patients with T1 disease is approximately 90-100% after simple cholecystectomy (8-12). However, the long-term outcomes of patients with advanced-stage disease are poor despite extended cholecystectomy (12, 13). The 5-year OS rates in patients with stage II, III and IV GBC are approximately 50-78%, 0-69% and 0-11% (14, 15). These poor outcomes have been attributed to the high rate of locoregional recurrence (LRR) and/or distant metastasis (16-19).
To reduce LRR, postoperative radiotherapy (PORT) with or without chemotherapy has been attempted (18-23). Because of the rarity and poor prognosis of GBC, prospective randomized trials have not been conducted, whereas most retrospective studies are limited by a small sample size and heterogeneous population. Therefore, the role of adjuvant radiotherapy (RT) with or without chemotherapy remains unclear. In the present study, we performed a retrospective analysis to evaluate the results of PORT and to identify prognostic factors for GBC.
Patients and Methods
Patients. We retrospectively reviewed patients with GBC who underwent surgical resection followed by PORT at the Asan Medical Center between November 1993 and December 2009. The eligibility criteria for the present study were as follows: (i) histologically proven gallbladder adenocarcinoma; (ii) surgical resection with potentially curative aim; (iii) no evidence of distant metastasis other than N2 lymph nodes; (iv) no history of malignancy other than skin cancer; (v) Eastern Cooperative Oncology Group (ECOG) performance status ≤2; and (vi) radiation dose >30 Gy. Patients who underwent incomplete resection with grossly residual disease or palliative bypass surgery were excluded from the analysis.
The pathological stage was determined according to the American Joint Committee on Cancer (AJCC) 7th edition TNM stage classification. The status of residual disease after surgical resection was reported as R0 (complete resection with grossly and microscopically negative margins of resection), R1 (grossly negative but microscopically positive margins of resection) and R2 (grossly and microscopically positive margins of resection). This study was approved by the Institutional Review Board of Asan Medical Center.
Adjuvant treatments. All patients received three-dimensional conformal radiotherapy (RT) using 6 or 15 MV photon beams. The clinical target volume (CTV) included regional lymphatics with or without the primary tumor bed, and a planning target volume (PTV) margin of 1-2 cm was added to the CTV to compensate for setup and respiratory motion-associated uncertainties. The regional lymphatics included the porta hepatis, peripancreatic, celiac, origin of the superior mesenteric artery and para-aortic nodes. In patients who underwent R1 resection, boost RT was delivered to the tumor bed. In certain patients, concurrent chemotherapy was delivered in two cycles of monthly 5-fluorouracil (5-FU; 375–500 mg/m2/day) ± leucovorin (20 mg/m2/day) for 3 days per cycle on day 1 and day 28 of PORT, oral uracil/tegafur (300 mg/m2/day) ± leucovorin (90 mg/day) or capecitabine (1650mg/m2/day) initiated on the first day of RT. Additional chemotherapy after PORT was occasionally performed according to the physician's preference.
Adverse events occurring during and within 3 months after PORT were defined as acute toxicities and events occurring 3 months after PORT were defined as late toxicities. The severity of toxicity was assessed according to the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE), version 4.02 (24).
Statistics. Follow-up duration was calculated from the date of the start of PORT. LRR was defined as any recurrence in the primary tumor bed and regional lymphatics, as well as locoregional control (LRC) rate was calculated from the date of the start of PORT to the date of LRR. Disease-free survival (DFS) was calculated from the date of the start of PORT to the date of LRR, distant metastasis (DM) or death of any cause. LRC, DFS and OS were estimated according to the Kaplan–Meier method and log-rank tests were performed for univariate analysis of prognostic factors. The Cox proportional hazards model was used for multivariate analysis. All statistical tests were two-sided and performed at the 5% level of significance by using the SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA).
Results
Patient and treatment characteristics. A total of 86 patients with gallbladder adenocarcinoma underwent surgical resection with potentially curative intent and subsequent PORT at Asan Medical Center between November 1993 and December 2009. Forty-two patients received simple cholecystectomy and 44 patients received extended cholecystectomy. Fifteen patients were incidentally diagnosed as GBC after simple cholecystectomy and seven of these patients underwent further extended resection. The median total RT dose was 50 Gy (range=43.2–60 Gy) in 1.8- or 2.0=Gy fractions. Sixty-one patients (71%) received concurrent chemotherapy. Among these patients, 25 (41%) received two cycles of monthly 5-FU±leucovorin, 18 received oral uracil/tegafur±leucovorin and 18 received capecitabine during RT. Additional chemotherapy after PORT was performed in ten patients (12%).
Patients' characteristics are shown in Table I. The median age was 61 years (range=37–85 years) and the male/female ratio was 1.2. Forty-five patients (52%) were pT2, 40 (47%) were pT3 and one was pT1b with involvement of N1 lymph nodes. Among the 48 patients who underwent lymph node dissection, 20 were pN0, 24 were pN1 and four were pN2. The overall stage was II in 36 patients (42%), III in 46 patients (54%) and IV in four (5%) patients. All four patients with stage IV disease had involvement of N2 lymph nodes without DM. Seventy-two patients (84%) underwent R0 resection and 14 patients (16%) had R1 resection. On pathology, tumors were poorly-differentiated in 13 patients (15%). Perineural invasion and lymphovascular invasion were positive in 26 (30%) and 21 (24%) patients, respectively. Preoperative carbohydrate antigen 19-9 (CA 19-9) was <37 U/ml in 40 patients (47%), ≥37 U/ml in 17 patients (20%) and unknown in 29 patients (34%). Postoperative CA 19-9 was ≥37 U/ml in 11 patients (13%).
Patients' characteristics.

Locoregional control (LRC), disease-free survival (DFS) and overall survival (OS) rates in all patients.
Survival. The median follow-up period was 50 months (range=6-225 months) for all patients and 83 months (range=26-225 months) for surviving patients. The 5-year LRC rate was 73% (Figure 1) and no significant difference in LRC was observed between patients undergoing simple cholecystectomy and those undergoing extended cholecystectomy (5-year LRC rates, 76% vs. 71%, p=0.570). In the 15 patients who were diagnosed with GBC incidentally, the LRC was also similar between the simple-cholecystectomy and extended-cholecystectomy groups (5-year LRC rates, 69% vs. 50%, p=0.721). In patients who underwent R0 and R1 resection, the 5-year LRC rates were 74% and 76%, respectively (p=0.127) (Figure 2).
The 5-year DFS rates were 36% in the entire cohort (Figure 1) and 41% and 31% for simple and extended cholecystectomy patients, respectively (p=0.268). According to the residual disease status, 5-year DFS rates were 40% and 14% for R0 and R1 resection, respectively (p=0.001) (Table II). Median survival period was 51 months, with a 5-year OS rate of 42% (Figure 1). The OS did not differ significantly according to the extent of cholecystectomy (simple vs. extended, 45% vs. 38%, p=0.452). The 5-year OS rates for patients with R0 and R1 resection were 45% and 21%, respectively (p=0.003) (Table II).
Prognostic factors. On univariate analysis, postoperative CA 19-9 level was the only significant prognostic factor for LRC. Patients with postoperative CA 19-9 level <37 U/ml showed better LRC than those with elevated postoperative CA 19-9 level (78% vs. 49%, p<0.001) (Table II). Regarding DFS, T stage (p=0.002), overall stage (p=0.012), residual disease status (p=0.001), differentiation (p=0.027), lymphovascular invasion (p=0.021), preoperative CA 19-9 level (p=0.031) and postoperative CA 19-9 level (p<0.001) were significant prognostic factors in the univariate analysis (Table II). T stage (p=0.002), overall stage (p=0.027), residual disease status (p=0.003), differentiation (p=0.045), lymphovascular invasion (p=0.010) and postoperative CA 19-9 level (p<0.001) were significant prognostic factors for OS in the univariate analysis (Table II).
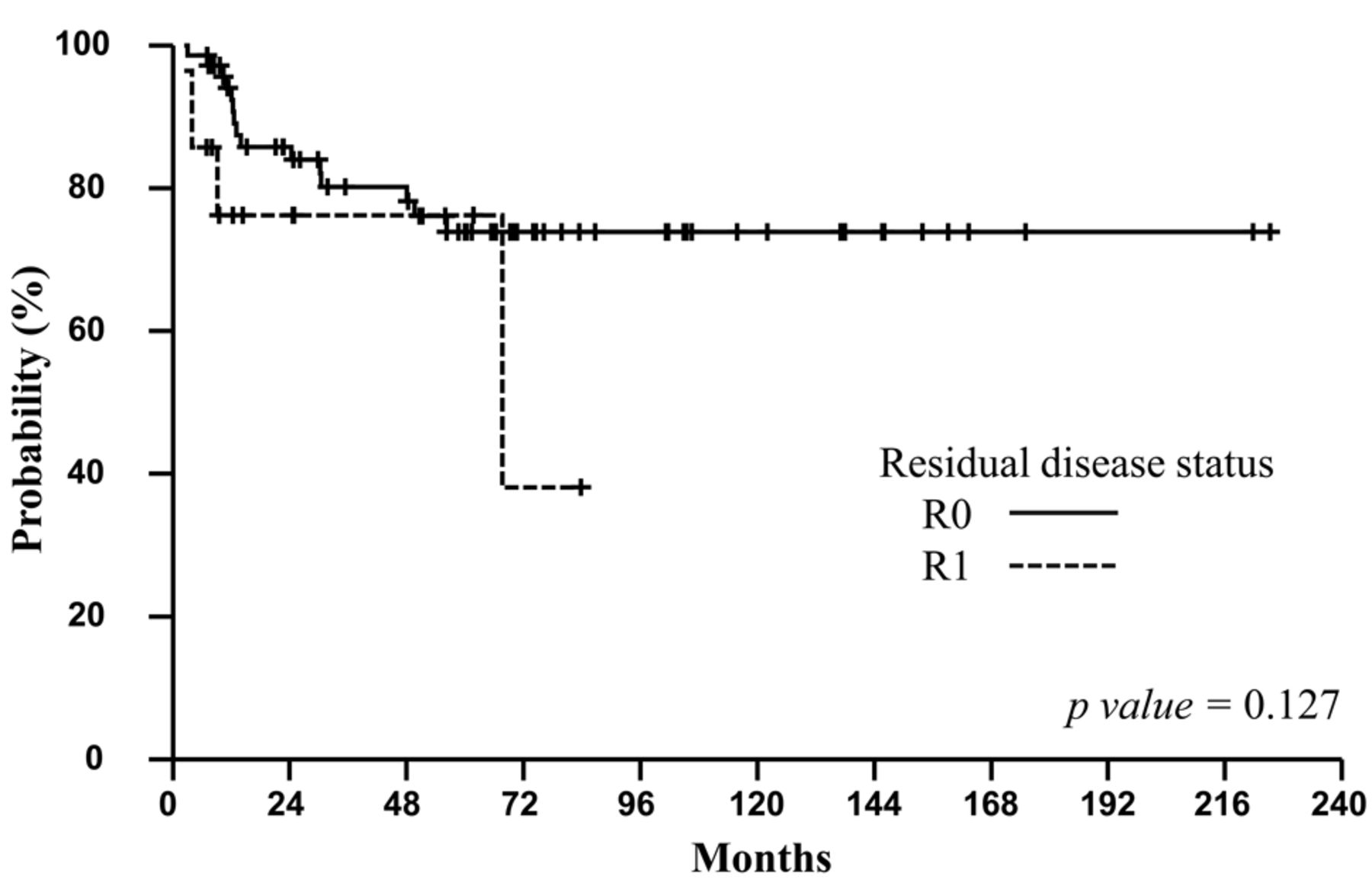
Locoregional control (LRC) rates according to residual disease status in all patients.
Patients with higher T stage showed inferior OS rates (5-year OS rates of pT1–2 vs. pT3, 58% vs. 23%) (Figure 3A). No significant differences in OS according to pN stage were observed, with 5-year OS rates of 54%, 33%, 25% and 42% for pN0, pN1, pN2 and pNx, respectively (p=0.141) (Figure 3B). In the 38 patients with pNx stage, the 5-year OS rate was 42% and it did not differ significantly from that of patients with pN0 stage (p=0.505) or pN1 stage (p=0.260). When pNx stage patients were classified as pN0, marginally-significant differences in OS were detected between pN0, pN1 and pN2 stage patients (5-year OS rates, 46% vs. 33% vs. 25%, p=0.080) (Figure 3C). The overall stage was a significant prognostic factor for OS, with 5-year OS rates of 55%, 33% and 25% for stage II, III and IV patients, respectively (p=0.027) (Figure 3D). Patients with postoperative CA 19-9 level <37 U/ml showed superior 5-year OS rate than those with elevated postoperative CA 19-9 level (46% vs. 0%) (Figure 3E).
In the multivariate analysis, postoperative CA 19-9 level was a significant prognostic factor for LRC (hazard ratio (HR):12.978, confidence interval (CI):1.662–101.300, p=0.015), DFS (HR:7.605, CI:2.535–22.810, p<0.001) and OS (HR:10.335, CI:2.953–36.170, p<0.001). T stage was significant for OS (HR:2.349, CI:1.051–5.249, p=0.037) and RM status was significant for DFS (HR=2.557, CI=1.165–5.614, p=0.019) (Table III).
Prognostic factors for survival by univariate analysis.
Patterns of failure. Among the 86 patients, 49 (57%) experienced failure and the site of first failure was isolated LRR in seven patients (8%), distant metastases in 36 patients (42%) and both in six patients (7%) (Figure 4). Nineteen patients (22%) eventually experienced LRR and the site of LRR was the local area in five (22%) and regional lymph nodes in 14 (78%) patients. The most common sites of DM were the liver (n=20), peritoneum (n=12), lung (n=9), distant lymph nodes (n=6), soft tissue (n=2) and bone (n=2). Among eight patients with involvement of pancreaticoduodenal lymph nodes, five (63%) did not experience LRR or DM and three of these five patients are still alive with 5-year OS and DFS rates of 63%. Three of the eight patients died from recurrence of disease (peritoneum (n=2) and resection margin of the liver (n=1)). All pN2 stage patients (n=4) developed DM and died.

Overall survival (OS) according to T stage (A), N stage (B, C), overall stage (D) and postoperative CA 19-9 level (E) in all patients.
Toxicities. Acute hematologic toxicity occurred in four patients with grade 3 and 4 neutropenia in one and three patients, respectively; however, no neutropenia-related infection was reported. One patient had G3 vomiting during RT but improved with supportive care. Late gastrointestinal toxicities included grade 3 duodenal bleeding in three patients at 4 months, 11 months and 5.3 years after PORT. Patients were treated with endoscopic sclerotherapy, hemo-clipping and conservative management. Two patients who received a total dose of 50 and 60 Gy experienced grade 5 duodenal bleeding that was not controlled by endoscopic intervention because of the broad-based ulceration and died at 11 and 12 months, respectively. One patient had grade 3 anastomotic stricture at 6.3 years after RT and improved after balloon dilatation.
Prognostic factors for survival determined by multivariate analysis.
Discussion
The results of the present study show that adjuvant RT with or without chemotherapy might be an effective treatment for GBC in terms of LRC, DFS and OS. Most patients with GBC are diagnosed at an advanced stage and show poor prognosis despite extended cholecystectomy (1-5), which has been attributed to high rates of LRR and/or DM. Because the major pattern of failure is DM, whether adjuvant RT to reduce the rate of LRR is beneficial for patients with GBC remains controversial. Jarnagin et al. analyzed the patterns of initial disease recurrence after resection of GBC and showed that 53 of 80 (66%) patients experienced recurrences (16). In that study, the major pattern of initial failure was DM (85%) with or without LRR, and isolated LRR occurred in 15% of patients. The authors concluded that adjuvant RT to reduce LRR is not beneficial for patients with GBC after curative resection (16). However, the median follow-up time (24 months) in that study was relatively short and the clinical outcome was poorer (median survival of 31.3 months) than that reported by other studies (18-23) (Table IV). Although the major pattern of failure is DM, several studies have shown that LRR after curative resection in patients with GBC is not uncommon (17-19). Gold et al. reported that 34 of 73 (47%) patients who underwent curative surgical resection experienced recurrence and the rate of LRR was 35% (12 of 34) of all recurrences (18). Moreover, 25 of 73 patients received adjuvant chemoradiotherapy and showed slightly lower LRR rates than the 48 patients who underwent surgery alone (30% vs. 36%), despite the fact that patients treated with adjuvant chemoradiotherapy were at more advanced stages. In the present study, the major initial failure pattern in the 49 of 86 patients (57%) who experienced recurrences was DM (86%) with or without LRR, and isolated LRR occurred in 14% of patients. Although the pattern of initial failure in the present study was similar to that reported by Jarnagin et al., the overall recurrence rate was lower and LRC was relatively high (5-year LRC, 73%). This improvement of LRC might be related to the relatively superior overall survival. Moreover, several studies also reported that adjuvant RT with or without chemotherapy is associated with better survival rates (5-year OS rate of range from 33% to 45%) than those of surgery alone reported in historical studies (18-23) (Table IV).

First site of failure for all patients.
Literature review of adjuvant radiotherapy for gallbladder cancer.
Extended cholecystectomy and residual disease status have been reported as prognostic factors for GBC (9, 11, 12). Among recent reports on the outcomes of PORT for GBC, several studies also reported the prognostic value of extended cholecystectomy (22) and residual disease status in patients treated with PORT (20, 22, 23). In the present study, LRC rates were not significantly different according to the extent of cholecystectomy or residual disease status. There are two possible explanations for these results. First, PORT might control microscopic residual disease, and thus reduce LRR or prolong the time to LRR. Furthermore, none of the present patients had gross residual disease, unlike those of the other two studies that reported the prognostic value of residual disease status (20, 23). Second, because the incidence of LRR was relatively low, the sample size might be too small to detect differences.
In the present study, 38 patients (44%) did not undergo lymph node dissection and were staged as pNx. The 5-year OS of pNx stage patients was 42% and, although not statistically significant, the OS of pNx patients was superior to that of pN1 or pN2 patients (5-year OS of pN0, pN1 and pN2: 54%, 33% and 25%, respectively, p=0.141). Kim et al. analyzed the outcomes of patients who did not undergo lymph node dissection and reported that the 5-year OS of patients with pNx (n=10) disease was inferior to that of patients with pN0 or pN1 disease (5-year OS of pN0, pN1 and pNx: 41%, 54% and 25%, respectively, p=0.194) (23). However, the difference was not statistically significant and among patients who received R0 resection, those with pNx stage showed similar survival to those with pN0 or pN1 disease (5-year OS of pN0, pN1 and pNx: 46%, 60% and 44%, respectively, p=0.625). The authors'explanation for this result was that four out of ten patients with pNx stage had R1 or R2 resection and the residual disease status might influence the poor survival outcome of pNx patients. Although the OS of patients with pNx stage was relatively good in the present study, unlike that of the patients in the study of Kim et al., only 7 of 38 patients had R1 resection and this could be related to the relatively favorable survival rates of pNx stage patients. Furthermore, all the patients in the present study received RT at regional lymphatics, which might be considered as an alternative to lymph node dissection.
According to the AJCC 7th edition TNM stage classification, pancreaticoduodenal lymph node involvement indicates N2 stage (stage IV) and surgical resection is considered inappropriate for patients with pancreaticoduodenal lymph nodes (25). However, in the Japanese staging system, pancreaticoduodenal lymph nodes are classified separately from other N2 node diseases and several studies showed that patients with only pancreaticoduodenal lymph node involvement have better survival than those with other N2 diseases (26, 27). In the present study, eight patients (9%) had pancreaticoduodenal lymph node involvement and their 5-year OS was 63%, which was more statistically significant than that of patients with pN1 or pN2 disease. Furthermore, five of these eight patients (63%) did not experience any LRR or DM and two of five patients are still alive. Because of the favorable survival rates of patients with pancreaticoduodenal lymph nodes, we classified these patients as pN1. Whether pancreaticoduodenal lymph nodes should be considered as regional lymph nodes is a subject of debate. However, long-term survivors with pancreaticoduodenal lymph node involvement have been reported, which indicates that clinicians should carefully consider whether to give up curative surgical resection in these patients.
In the present study, postoperative CA 19-9 level was a significant prognostic factor for LRC, DFS and OS. In our previous study, postoperative CA 19-9 was identified as a prognostic factor for extrahepatic bile duct cancer (28). Although postoperative CA 19-9 level is a well-known prognostic factor for pancreatic cancer (29), its prognostic value in biliary cancer has not been reported to date. Our results showed that among the 78 patients (90%) with postoperative CA 19-9 data, 11 (13%) who had an elevated postoperative CA 19-9 level showed significantly poorer OS than those with normalized postoperative CA 19-9 levels (median survival, 56 months vs. 8 months). Moreover, only one out of these 11 patients showed normalization of CA 19-9 levels after PORT. Although a definite conclusion cannot be made because of the retrospective nature of the study and the small number of patients with elevated postoperative CA 19-9, our results indicate that postoperative CA 19-9 may be related to the aggressiveness of tumors showing poor responsiveness to PORT as well as residual tumor burden. Further evaluation with a larger sample size is necessary to determine whether aggressive treatment might benefit these patients with an elevated postoperative CA 19-9 level.
The present work has certain limitations associated with the heterogeneous population and the retrospective nature of the study, similar to previous studies on GBC. However, in the present study, all patients underwent CT simulation-based three-dimensional conformal RT and two thirds of the patients received concurrent chemoradiotherapy. To the best of our knowledge, the present study is one of the largest series analyzing patients treated with relatively modern adjuvant chemoradiotherapy for GBC. In conclusion, adjuvant radiotherapy might be an effective treatment in terms of LRC for patients with GBC. Finally, postoperative CA 19-9 might be useful as a surrogate marker for LRC, DFS and OS.
Footnotes
-
Conflicts of Interest
No potential conflicts of interest exist. None of the Authors have any external funding or grants to disclose.
- Received June 7, 2014.
- Revision received July 19, 2014.
- Accepted July 22, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}