


Abstract
Background: Primary high-grade serous peritoneal carcinoma (PPSC) is a rare malignancy with an ambiguous pathogenesis. Case Report: We report on a 51-year-old woman presenting with a routine smear test cytology suspicious of adenocarcinoma. She underwent hysteroscopy, laparsocopy with multiple biopsies and bilateral salpingoophorectomy. She was diagnosed with a serous tubal intraepithelial carcinoma in situ (STIC) in the right fallopian tube. Subsequently, she underwent radical surgery and was diagnosed with peritoneal high-grade serous carcinoma. Interestingly, both ovaries remained histologically tumour-free. Discussion: High-grade serous carcinomas that arise on the peritoneum with tumour-free ovaries are rare. The findings in this case, coupled with current evidence, strongly suggest a precursor lesion in the fallopian tube (STIC lesions). The clinical implications of this theory reside in the potential for improving early detection strategies. Nonetheless, more data on precursor lesions in the fallopian tubes and their transformation to serous carcinoma are required to plan for future screening methods.
- Primary peritoneal cancer
- high-grade serous carcinoma
- serous ovarian carcinoma
- serous intra-epithelial carcinoma in situ
- STIC
Ovarian cancer is the eighth most common malignancy diagnosed in women and the leading cause of death among gynaecological cancer (1). Most ovarian carcinomas are of the serous type and can be classified into high-grade and low-grade types, based on cytological features (2). High-grade serous carcinomas are known to be more aggressive in nature than low-grade carcinomas (3). Subsequently, 70% of patients with high-grade serous carcinomas present with disease at advanced clinical stages, after spread to the ovarian surface and peritoneum, making prognosis very poor (3, 4). The disproportionately high, and largely unchanged, mortality rate of serous ovarian cancer is primarily attributed to the absence of early symptoms in many patients, unavailability of effective screening tools, and lack of clarity regarding the aetiology and development of the disease (5).
High-grade pelvic serous non-uterine carcinomas have usually been classified as ovarian carcinomas (1). However, in recent years, our understanding of serous ovarian carcinogenesis has evolved. Recent pathological and genomic studies indicate that many ovarian carcinomas are derived from non-ovarian tissues (6). In fact, it has been known that in 18-28% of cases presenting with classical signs of advanced primary serous ovarian carcinoma, the ovaries look normal and may even be tumour-free with involvement of the peritoneum (7). In these cases, where no other source is evident, the peritoneum is assumed to be the primary site.
The clinical entity of primary peritoneal serous carcinoma (PPSC) was first reported in 1959. It is a rare malignancy that refers to the diffuse involvement of peritoneal surfaces with a neoplasm appearing identical to ovarian serous carcinoma, in the absence of a demonstrable primary ovarian tumour (8, 9). There seems to be no significant epidemiological difference between serous cancer arising primarily within the ovary from that arising in the peritoneum (9). PPSC is clinically-indistinguishable from advanced high-grade serous ovarian carcinoma (HSOC) and is only diagnosed at laparotomy (9). Consequently, most PPSCs are initially thought to be ovarian carcinomas.
In contrast to serous ovarian carcinoma, the pathogenesis of PPSCs remains ambiguous (10). In fact, the main aspect influencing our understanding of these tumours is the lack of clarity regarding the precursor lesion responsible for the disease (1).
Recently, studies of women with breast cancer gene (BRCA) mutations undergoing risk-reducing salpingo-oophorectomy have highlighted the distal fallopian tube as a common (80%) site of tumour origin (11, 12). Additional studies of unselected women with pelvic serous carcinoma have demonstrated that serous tubal intraepithelial carcinoma (STIC) is a precursor in a significant proportion of these tumours (6, 13). This case report highlights the causal relationship between serous tubal intraepithelial carcinoma in situ of the fallopian tube and high-grade PPSC.

Serous tubal intra-epithelial carcinoma in situ of right fallopian tube with dissolute cells. Original magnification ×200.
Case Report
In the resent report, we present the rare case of a 51-year-old woman who was initially seen in the Outpatient Department following a routine PAP IIID smear test. The patient presented symptom-free but with a strongly-positive family history. Her mother was diagnosed with ovarian cancer at the age of 57 years.
Repeat speculum examination, as well as transvaginal, abdominal and pulmonary ultrasound scans, were unremarkable. The abdomen was soft with no palpable masses and no palpable supraclavicular or axillary lymphadenopathy. The tumour marker cancer antigen-125 (CA125) was mildly raised at 52 U/ml with a normal human epididymis protein 4 (HE4) level at 62.87 pmol/l. A repeat smear test cytology showed atypical cells suspicious of an adenocarcinoma.
Following a detailed discussion of the above findings, the patient underwent a hysteroscopy to obtain cervical and endometrial biopsies, and a laparoscopic bilateral salpingoophorectomy with samples obtained from the peritoneum and fluid from the pouch of Douglas. Intraoperatively, the macroscopic appearance of both ovaries was unremarkable.
Postoperative histology revealed a serous tubal intraepithelial carcinoma (STIC) in situ of the right fallopian tube (Figure 1). The specimen strongly expressed p53 on immunohistochemical staining (Figure 2). The right ovary was free of tumour cells. In the left fallopian tube, there were small areas of atypical cells with enlarged nuclei and free floating atypical cell complexes in the lumen of the tube. However, intra-abdominal fluid cytology interestingly showed a high quantity of atypical micropapillary cell complexes, suggestive of a malignant effusion with cells of a dimorphic adenocarcinoma (Figure 3). This raised the question of whether these tumour cells had spread from the previously diagnosed STIC or whether they were part of a synchronous manifestation of a PPSC of unclear origin.

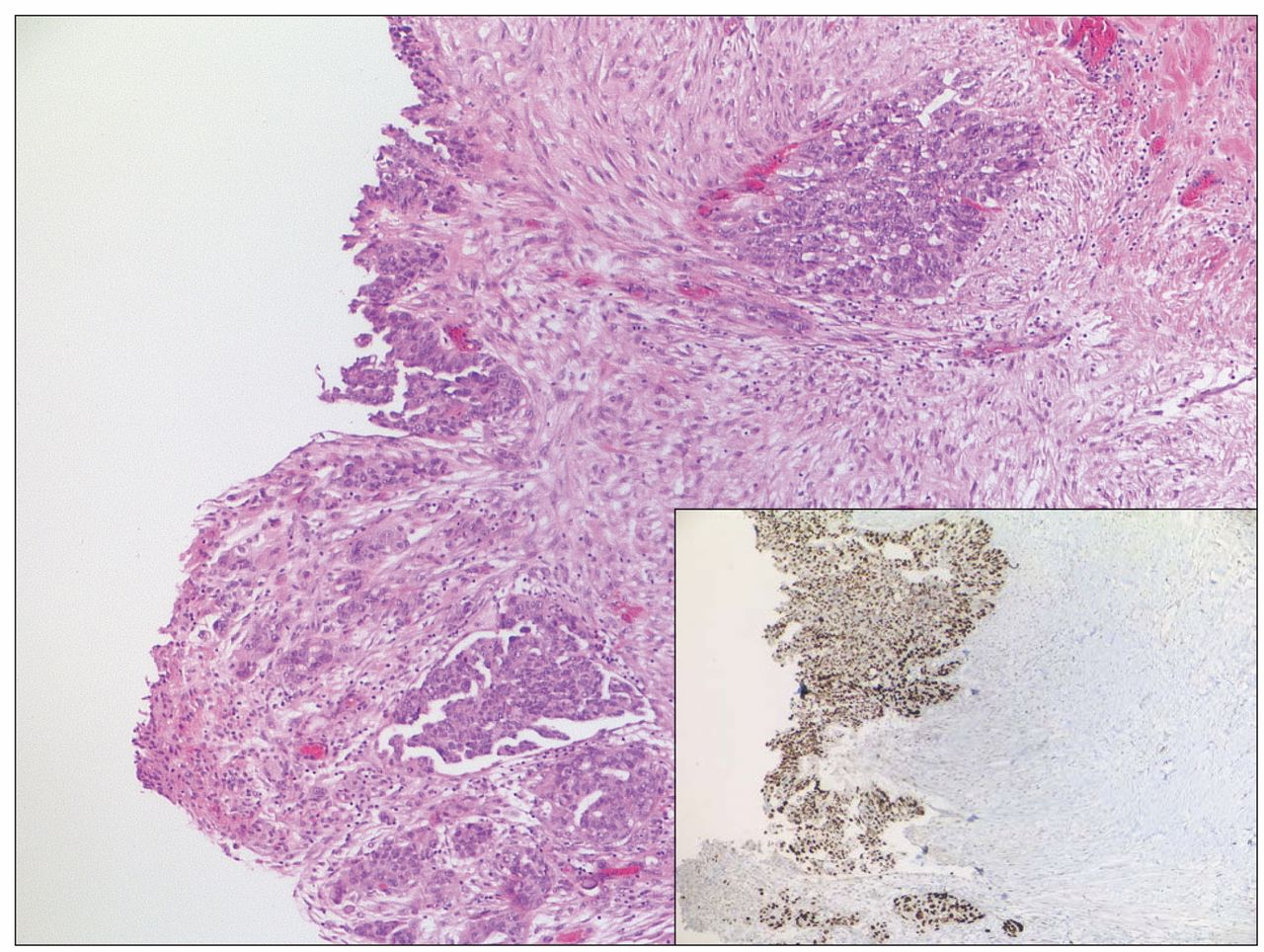
Serous tubal intra-epithelial carcinoma in situ of right fallopian tube. Note the positive immunohistochemical staining for p53. Original magnification ×200.

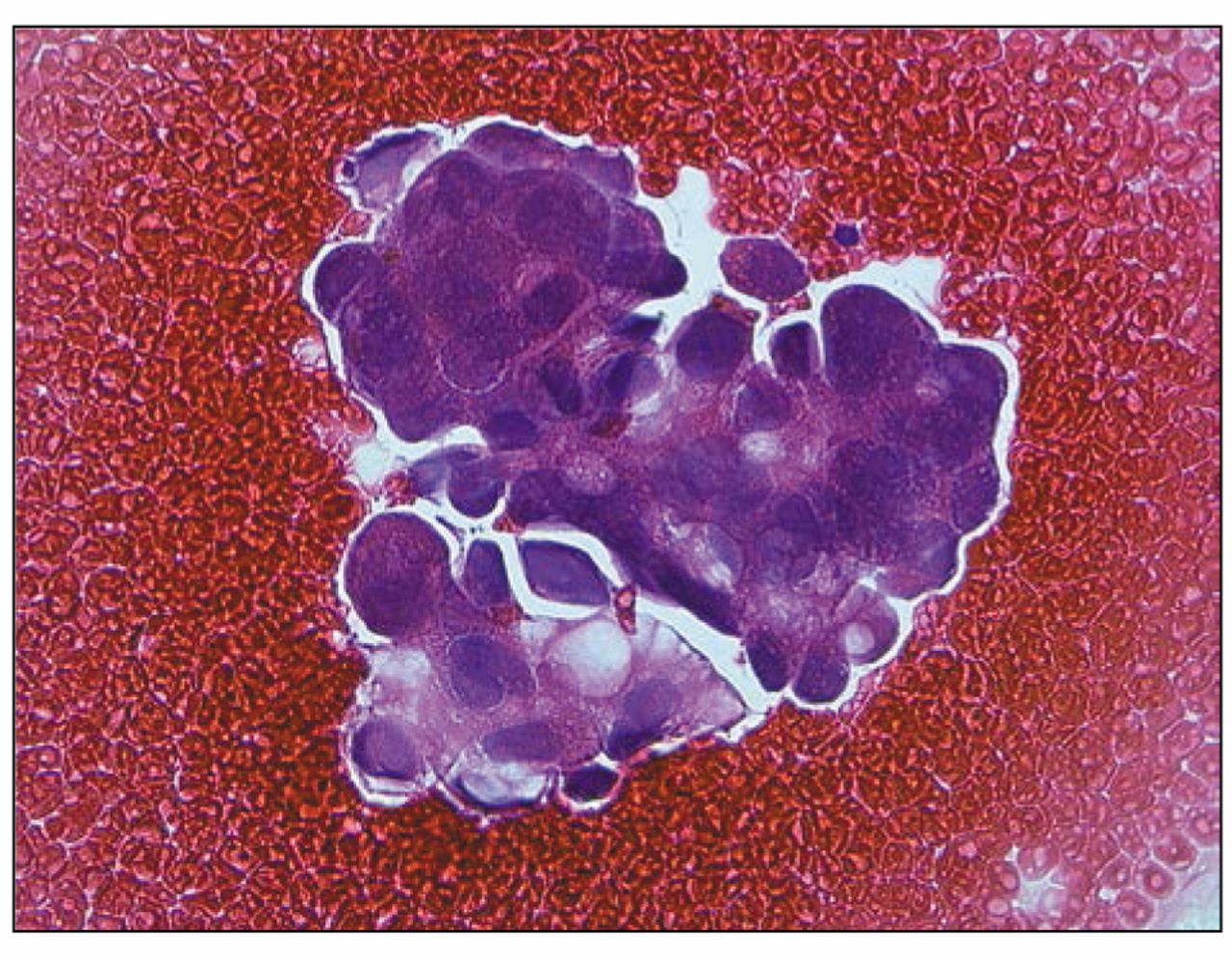
Serous carcinoma cells in fluid cytology. Original magnification ×400.
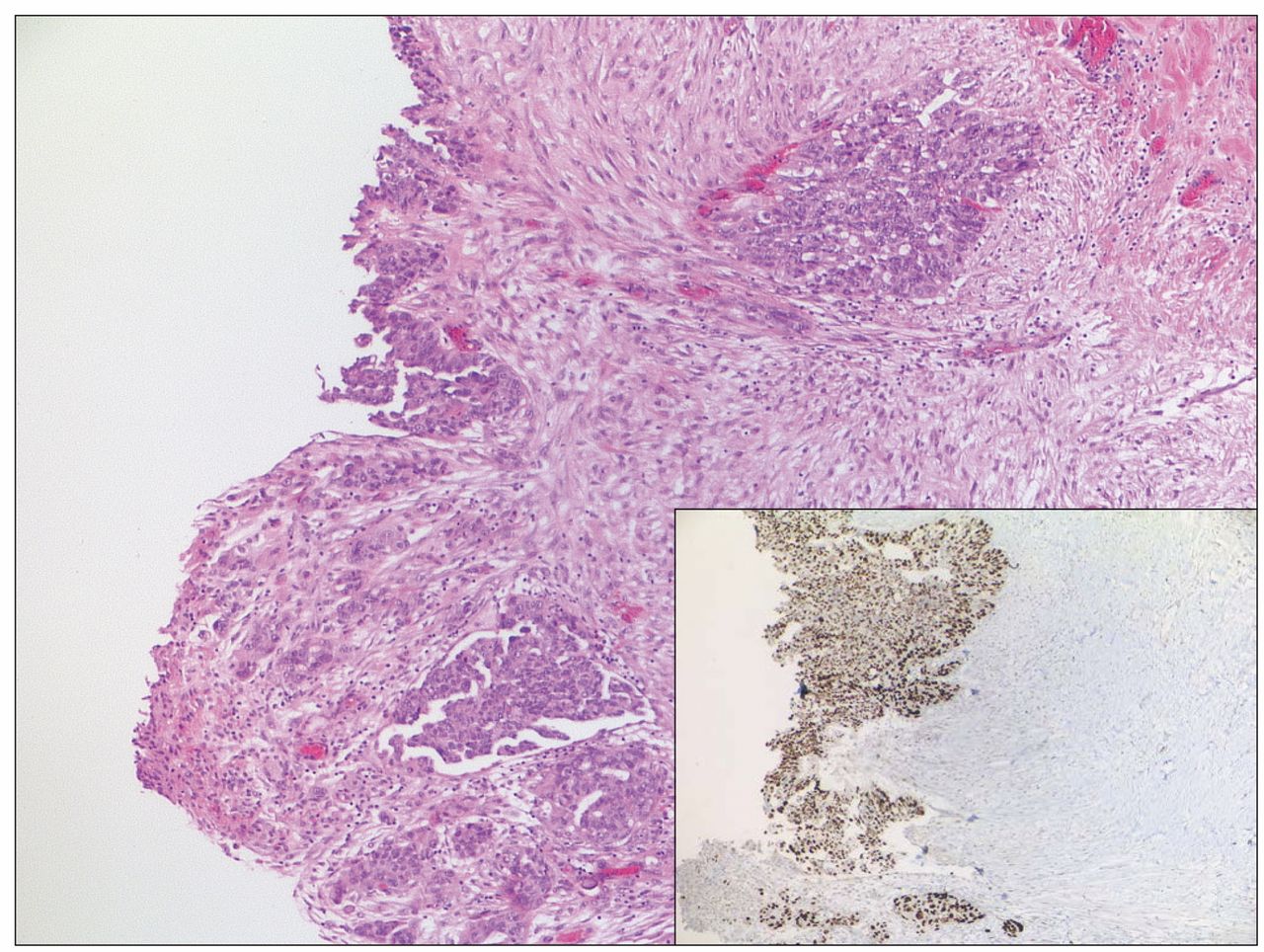
Pelvic peritoneum with focal invasive serous carcinoma, original magnification ×50. Note the strong nuclear positivity for p53 on immunohistochemical staining (Inset, original magnification ×50).
In light of the above results, the patient was re-admitted for a further staging laparoscopy with appendicectomy, partial omentectomy, pelvic lavage and repeat peritoneal samples and fluid cytology. A repeat hysteroscopy and curettage were also performed to obtain endometrial and cervical samples.
The histology was as follows: Cervical and endometrial samples: adenocarcinoma in situ; pelvic peritoneum: evidence of a small area of papillary serous carcinoma with focal reactive mesothelium. This area showed strong expression of p53, cytokeratin (CK) 7 and CA125 on immunohistochemical staining (Figure 4); omentum: invasive serous carcinoma. There was no evidence of malignancy in the appendix.
Subsequently, the patient underwent open hysterectomy, de-peritonealisation, infragastric omentectomy, and systematic pelvic and para-aortal lymphadnectomy.
Surprisingly, the histological report showed evidence of infiltrates of a serous high-grade carcinoma in the ileocaecal area. Serous carcinoma infiltrations were also detected in the serosa of the uterus, especially in the mesovarium bilaterally and in the cervix. Interestingly, both ovaries remained tumour-free.
Lymphangiosis carcinomatosa and invasive peritoneal carcinoma were detected in the peritoneum. Visible lymph node metastases were found in the infrarenal, infra-aortal, caval, supra and infra- mesenterial, bilateral external iliac, and pelvic areas.
Hence, the patient was diagnosed with a high-grade PPSC staged as pT2cpN1(14/98)G3L1V0 (FIGO III c) with a synchronous STIC in the right fallopian tube.
She recovered well postoperatively and commenced adjuvant chemotherapy with paclitaxel/carboplatin and bevacizumab as per the management of serous high-grade ovarian carcinoma.
Discussion
High-grade serous carcinomas that arise as masses on the peritoneal surface with normal tumour-free ovaries are rare (10). Such cases have traditionally included tumours arising from the ovary, as well as PPSC (10). However, many studies have demonstrated that clinically and histologically, PPSC and ovarian carcinoma are currently indistinguishable (14-16). This has led to the re-classification of 10% of supposed ‘ovarian’ carcinomas as PPSC (14). Moreover, the recently published recommendations by Vaughan et al. (6) suggest that the term ‘serous ovarian carcinoma’ encompasses a series of distinct diseases frequently arising from non-ovarian tissues but sharing an anatomical location, and that a better term would be ‘pelvic or peritoneal cancer (6). The clinical and pathological similarities between PPSC and serous ovarian carcinoma indicate that they may have the same origin (14).
Consequently, the subject of the origin and development of high-grade PPSC has been controversial for many years (7). There have been multiple theories regarding the histogenesis of PPSC. The first is that it develops from the ovarian surface epithelium (OSE) then spreads throughout the peritoneal cavity (9). The primary tumour is thought to be microscopical and therefore undetectable, or to have regressed completely for unknown reasons (17). The OSE may be vulnerable to malignant transformation as a result of repeated injury following ovulation, due to hormonal factors (18). The incessant ovulation theory proposed by Fathalla (19) in 1971 suggests that the perpetual cycle of damage and repair of the OSE during and following ovulation increases the risk of malignant transformation (2, 20). Observational studies suggest that ovarian inclusions arise following ovulation through the invagination of the OSE into the ovarian stroma. Following the invagination, the OSE is assumed to undergo Müllerian metaplasia and then malignant transformation (20). Supporting evidence suggests that factors suppressing ovulation (e.g. combined oral contraceptive pill, pregnancy, breast-feeding) reduce the occurrence of ovarian cancer (17, 20, 21), whereas a higher number of accumulated lifetime ovulations increases the risk of ovarian cancer (21). The hormonal theory postulates that oestrogen and gonadotrophins also cause stimulation and potentially malignant transformation of the OSE (17, 20).
In our case, these arguments seem relatively weak as both ovaries were macroscopically normal with no inclusion cysts and were histologically tumour-free. In fact, the evidence to support the OSE origin of PPSC remains circumstantial. The OSE is continuous with the mesothelium lining the pelvis. The OSE or mesothelium is embryologically different from Müllerian epithelia in general. However, serous ovarian carcinomas are Müllerian in nature and rarely exhibit the immunohistochemical or ultrastructural features of malignant mesothelioma (2, 5, 8). In addition, when examining the OSE and ovarian inclusion cysts, a true precursor lesion of high-grade serous carcinoma has been rarely found (5, 8). As for hormonal factors, oestrogen and progesterone receptors are not consistently present in PPSC, making their role speculative (9).
The second theory is that PPSC arises de novo from the peritoneum (9). Studies suggest that in some cases, PPSC can be polyclonal, arising in multiple primary peritoneal sites (9, 18). However, arguments against this theory emphasize that malignant mesothelial cells (lining the peritoneum) result in malignant mesothelioma which is entirely different from serous carcinoma (7). Therefore, evidence regarding PPSC clonality remains controversial (9).
Hence the question in our case remains of whether the serous carcinoma originated from the fallopian tube spreading to the peritoneum, or whether it was indeed a peritoneal primary that spread to the endosalpinx and subsequently induced the development of STIC.
Accumulating evidence suggests that the fallopian tube epithelium, mainly in the fimbria, is the source of a significant proportion of high-grade serous carcinomas previously thought to be of ovarian or peritoneal origin (7, 14).
A study conducted by Carlson et al. (10) demonstrated the presence of STIC in the fimbrial end of the fallopian tubes of a significant percentage (47%) of women with PPSC. In related studies (22, 23), patients with serous carcinomas were divided into those with and those without a dominant ovarian mass. STIC was found in 45% of patients without a dominant ovarian mass compared to 11% of those with a mass(22). These studies suggest that cases of PPSC are more likely to harbour STIC. More recently, a study by Seidman et al. (7), confirmed the above observations by examining fallopian tubes of 51 women diagnosed with PPSC. The study concluded that at least half (56%) of PPSC cases are associated with STIC of the fallopian tube, mostly involving the fimbrial region (46%). In a smaller study (1) involving 34 patients with PPSC, fallopian tube involvement was identified in more than 70% of cases, with 17% of cases demonstrating presence of STIC in the tube.
Moreover, many studies of women carrying a BRCA germline mutation endorse the concept that STIC is the earliest known malignant alteration in women with genetic risk factors (4). Examination of prophylactically-removed fallopian tubes in BRCA-positive women showed that a significant number (2-17%) of early serous carcinomas involve the fallopian tubes, with up to 100% of involvement being in the fimbrial end of the tube (4, 5, 11, 12, 24-26). Our patient had a positive family history and was, therefore, regarded as being at high risk. She was sent for genetic counselling and testing for possible BRCA mutations.
Further supporting evidence was found when examining fallopian tube specimens for p53 mutations. The most common molecular genetic change in high-grade serous carcinomas is a mutation in the p53 tumour-suppressor gene (27). In previous studies (10, 23), p53 mutations were compared in both peritoneal and tubal lesions. This analysis disclosed the same p53 mutation in both STICs of the fallopian tube and the remote peritoneal tumour, genetically linking the two (4). This corresponds to the histological findings in our case, where p53 was strongly expressed in the STIC cells of the right tube and the peritoneal sample.
All the above observations support the theory that STIC, which is almost always detected in the fimbriae of the fallopian tubes, may be the source of high-grade serous carcinomas in both BRCA-postive women and women with no predisposition to ovarian cancer. Nonetheless it is still unclear how STIC arises in the fallopian tube and eventually leads to PPSC. The most plausible explanation is that mutagenic factors (possibly inflammation) eventuate the formation of intraepithelial neoplasms in the fallopian tube (20). Chronic inflammation caused by infectious agents has been associated with cancer development. In fact, pelvic inflammatory disease has been linked to ovarian cancer (2). Through the process of retrograde flow from the endometrium, the fallopian tube is constantly exposed to inflammatory agents which can increase the potential for mutations (2). This potential is further increased in susceptible patients with BRCA mutations. Once such lesions have formed in the tubes, the loosely-cohesive cells can easily shed and implant on the ovarian surface and peritoneum (20), resulting in PPSC.
In our case, the above model explains the possible migration of STIC cells to the peritoneum, cervix and endometrium. The above evidence supports STIC as an established step in the serous carcinogenic sequence and the occasional discovery of STIC as the only lesion in women with established PPSC emphasizes its potential to exfoliate cells with metastatic potential (10).
Ultimately, the clinical implication of STIC of the fallopian tube being the likely precursor to pelvic serous carcinomas resides in the potential for interrupting the disease before it spreads (10). Currently, screening for enlarged ovaries in high-risk women does not target the appropriate group for a successful screening test (7). Instead, screening efforts should be focused on the fallopian tubes and detection of low-volume advanced stage, rather than early-stage serous cancer, as recommended by Vaughan et al. (6). The possibility of bilateral salpingectomy in BRCA-positive women with retention of the ovaries as primary prevention also merits consideration. However, more data on the natural history of precursor lesions in the fallopian tube epithelium and their transformation to serous carcinoma needed to plan for future screening methods and risk-reducing surgery.
Conclusion
The findings in our case, coupled with current evidence, strongly endorse the fallopian tube, especially the fimbrial region, as being the source of a significant proportion of PPSCs. The ‘tubal model’ proposing STIC in the fallopian tube as a precursor explains many features of PPSC. Despite extensive research, the pathogenesis of PPSC remains unclear and progress is largely hindered by the advanced stage of this tumour at the time of diagnosis. However, the implications of the new paradigm on screening and risk-reducing surgery is profound. More clinical studies are needed focusing on early detection of precursor lesions in the fallopian tube and outcomes of prophylactic salpingectomies.
- Received October 4, 2013.
- Revision received December 3, 2013.
- Accepted December 4, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.