


Abstract
Background/Aim: In endometrial cancer, visceral obesity, as a risk factor, is associated with a chronic inflammatory process, confirmed by the elevation of serum inflammatory markers in obese patients. The aim of the present study was to evaluate the correlation between visceral fat, assessed by ultrasonography, and the systemic levels of interleukin (IL)-8 in patients with endometrial cancer. This study also evaluated the usefulness of abdominal ultrasonography in assessing the visceral fat correlated with systemic inflammatory status, as an alternative method to identify patients at risk of endometrial cancer. Materials and Methods: The study was a case–control analysis including two groups of patients: Group I: 44 patients diagnosed with endometrial cancer; group II: 44 patients with no gynecological pathology. The diagnosis of endometrial cancer was performed following histopathological examination that evaluated the tissue material obtained through endometrial biopsy. These patients underwent ultrasound examination by which intraperitoneal fat was determined. IL-8 levels were determined for each patient. The Student's t-test was used for the comparison of the means and the Mann–Whitney test for rank comparison of two independent samples. Results: In patients diagnosed with endometrial cancer, the visceral fat area evaluated by ultrasound was significantly larger (p<0.0001) compared to that of the control group. The plasma levels of IL-8 in the endometrial cancer group were significantly elevated (p<0.001) compared to the control group. A positive linear correlation was also found between the visceral fat area and plasma levels of IL-8. Conclusion: The plasma levels of IL-8 are positively linearly correlated with visceral fat. Determination of visceral fat in association with IL-8 levels may be a predictive factor for endometrial cancer.
In endometrial cancer, visceral obesity, as a risk factor, is associated with a chronic inflammatory process, confirmed by the elevation of seric inflammatory markers in obese patients. Obesity is known to increase the risk for many pathological processes including type-2 diabetes, cardiovascular diseases and endometrial cancer. In recent years, many studies have focused on the endocrine and paracrine function of adipocytes. Fat cells synthesize and secrete substances involved in regulation of food intake, energy expenditure, and local and whole-body carbohydrate and lipid metabolism (1). These substances include leptin, adiponectin, IL-6, IL-8, resistin, and many others (2).
Bruun et al. (3, 4) revealed that IL-8 is produced and secreted by human adipocytes. IL-8 is released from adipose tissue fragments into the medium, and IL-8 mRNA was found in isolated adipocytes. For these reasons, the correlation found between the severity of obesity and the development of type-2 diabetes, atherosclerosis, cardiovascular disease and endometrial cancer might be related to the ability of human adipose tissue to produce and release IL-8. However, there are no in vivo data regarding plasma IL-8 levels in obesity. IL-8 is related to obesity-related parameters such as the body-mass index (BMI) and waist circumference (5).
Recent studies have shown that visceral adipose tissue releases more circulating IL-8 than the subcutaneous and that circulating IL-8 is elevated in obesity (6, 7). The circulating level of IL-8 was found to be significantly higher with increasing waist circumference, supporting the idea that visceral fat may play a role in the elevation of circulating IL-8 in obesity.
IL-8 is expressed in macrophages and fibroblasts, being recognized as a macrophage-derived mediator of angiogenesis (8, 9). Fujimoto et al. found a significant correlation between infiltrated macrophage counts and IL-8 levels in endometrial cancer (10). IL-8 is expressed by many tumour cells, including breast (11), ovarian (12), cervical (13) and endometrial (14) cancer. A statistically significant correlation was also found between endometrial cancer stage and IL-8 expression (10).
Patient characteristics.
Materials and Methods
The study is a case–control analysis including two groups of patients: group I: 44 patients diagnosed with endometrial cancer; group II: 44 patients without gynecological pathology or inflammatory disorders (control group).
The diagnosis of endometrial cancer was determined through a histopathological examination where we analysed the tissue material obtained after an endometrial biopsy. The endometrial biopsy was carried in the case of significant metrorrhagia, or climax mettrorhagia, as well as for certain aspects assessed by ultrasonograply (US) (significantly thick and vascularised endometrium).
After the clinical examination and the anthropometric measurements of BMI and waist circumference, we assessed the intraperitoneal fat of these patients by US. BMI was calculated according to the formula BMI=weight (kg)/[height (m)]2. Waist circumference (cm) was measured while standing, at the level of the umbilicus. The ultrasonography evaluation (Voluson 730) was carried-out in the dorsal decubitus position at the end of a normal expiration after a 12-hour digestive pause in order to assess deposits of visceral fat. The visceral fat area determined by US was calculated according to the formula 9.008+1.191×[the distance between the internal surface of the right abdominal muscle and the splenic vein (mm)] + 0.987×[the distance between the internal surface of the right abdominal muscle and the posterior surface of the aorta (mm)] + 3.644×[the fat thickness of the right kidney posterior surface (mm)] (15).
From every patient included in the study, we collected 2 ml of blood by venepuncture in EDTA test tubes in order to carry-out a complete blood count, and 2 ml of blood in test tubes without anti-coagulants in order to determine the plasma level of IL-8. The serum obtained by centrifugation was separated and stored in freezing tubes of 600 μl each at a temperature of −30°C until samples were analyzed in order to avoid repeated frost–defrost cycles. The minimum detectable dose (MDD) of IL-8 (Human, IL-8 Immunoassay RD-D8000C R&D Systems USA) ranged from 1.5-7.5 pg/ml; the mean MDD was 3.5 pg/ml. The MDD was determined by adding two standard deviations to the mean optical density value of 20 zero standard replicates and calculating the corresponding concentration. The antibodies used for detection recognize both natural and recombinant human IL-8. No significant cross-reactivity or interference was observed.
We obtained the consent of all patients. The study was approved by the Ethics Commission of the Iuliu Hatieganu University of Medicine and Pharmacy, Cluj-Napoca.
All parameters were included in the study database and version 13 of SPSS software and Microsoft Excel with Analysis Tool Pack were used for statistical analysis. The Kolmogorov Smirnov test was applied for the testing of normal distribution. Student's t-test was used for the comparison of the means and the Mann–Whitney test for rank comparison of two independent samples. For multivariate models, the stepwise linear regression method was used.
Results
The characteristics of the patients included in this study are presented in Table I.
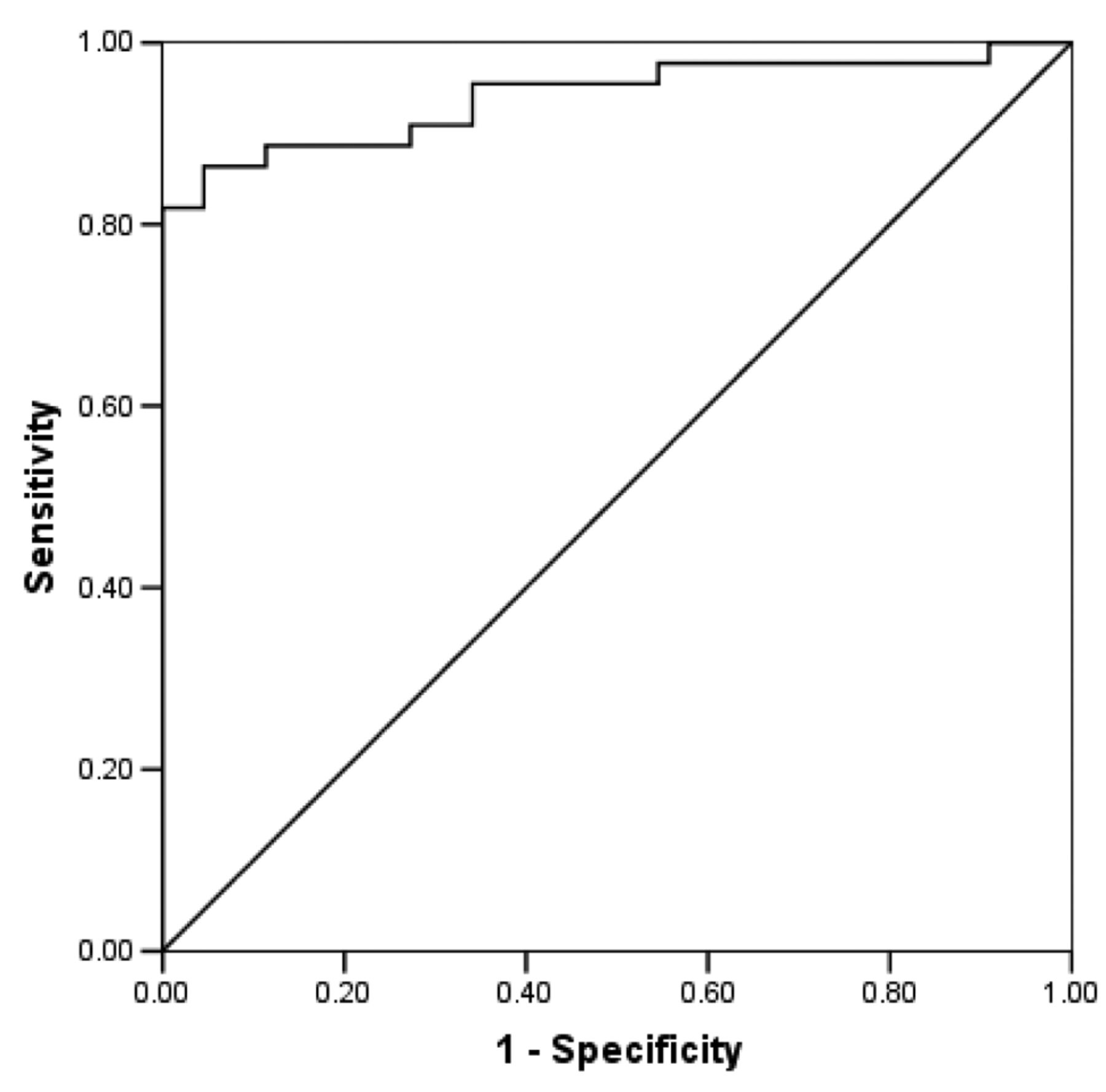
There was a statistically significant difference (p<0.0001) in visceral fat between the two groups. The (ROC) curve for identifying the cut-off point for visceral fat is shown in Figure 1. The area under the curve (AUC) was 0.95 (p<0.0001). The identified cut-off point was 172 (Se=0.863, Sp=0.935). Visceral fat of over 172 seems to be a cut-off value for the patients with endometrial cancer.
The median plasma IL-8 levels were significantly higher (p<0.001) in patients with endometrial cancer as compared to the control group.
The best IL-8 cut-off value to predict the risk for endometrial cancer is 6.96 pg/ml (Se=0.862, Sp=0.962, AUC=0.94, p<0.001). If a patient's plasma level of IL-8 exceeds 6.96 pg/ml, she is exposed to the risk of endometrial cancer (Figure 2).

ROC curve for identifying the cut-off point for visceral fat.
Visceral fat was positively linearly correlated with the plasma IL-8 level (Figure 3).
In order to establish the influence of the other variables on IL-8, a stepwise multivariate linear regression analysis was performed. The following variables were entered in regression: Age, BMI, waist circumference, visceral fat, age at menarche, and age at menopause. Out of these variables, only visceral fat had a significant influence on IL-8 levels.
Discussion
Visceral obesity is considered a low-level chronic pro-inflammatory state. The adipocyte is the central element that integrates multiple metabolic and endocrine signals. This cell is the source of a large number of bioactive peptides that play an essential role in the modelling of insulin resistance and inflammation.
One adipocyte-derived cytokine is IL-8 (3, 4). IL-8 is produced mainly by macrophages and monocytes, and plays a role in modulating an inflammatory response (16). IL-8 was significantly increased in obese individuals with BMI >30 kg/m2 compared to the non-obese controls (5). Recent studies have shown that visceral adipose tissue is a major source of chemokines such as IL-8 in obesity (6). The present study demonstrates that the plasma IL-8 levels have a positive linear correlation with visceral fat.
The plasma level of IL-8 may be an index linking visceral fat with obesity-related inflammation complications, such as endometrial cancer. The production of pro-inflammatory cytokines (tumor necrosis factor α, IL-6, IL-8, C-reactive protein) play an important role in endometrial cancer genesis. The present study demonstrates that circulating levels of IL-8 were significantly higher in patients with endometrial cancer compared to the control group.

curve for identifying the cut-off point for IL-8.

Correlation of intraperitoneal fat with interleukin-8 (IL-8).
The elevation of chemokines is often observed in inflammatory tissues (e.g. infection, autoimmune diseases, and atherosclerotic lesions) (17). Therefore, we hypothesized that chemokines are associated with the inflammatory condition in obesity. C-Reactive protein, a classical acute-phase protein, is a marker of the inflammatory cascade and its levels are known to increase in obesity.
Recent studies describe obesity through inflammation as a risk factor for endometrial cancer. This theory is supported by different hypotheses: the menstrual cycle is compared to an inflammatory process (18); oestrogen unbuffered by progesterone exerts an inflammatory effect on the endometrium (19); chronic inflammation of the endometrium is a risk factor for endometrial cancer (20); non-steroidal anti-inflammatory drugs (NSAIDs) inhibit endometrial cancer cells in vitro (21); menstrual suppression occurs in laboratory animals when administered long-lasting NSAIDs (22); there are no epidemiological studies showing the influence of NSAIDs on cancer of the endometrium, but populations with chronic inflammatory disorders who took NSAIDs long-term had a reduced risk for endometrial cancer (21).
With the onset of menopause, a low-grade pro-inflammatory condition also appears, which transforms into a spontaneous increase of serum levels of pro-inflammatory cytokines, such as: IL-1, IL-6 or IL-8 (23, 24). IL-8 is significantly higher in post-menopausal women with vasomotor symptoms than in women without vasomotor symptoms. In the post-menopausal group, the serum levels of IL-8 are similar to those of women with chronic inflammatory pathology (25). Therefore, increased plasma levels of IL-8 during menopause may be considered a risk factor for endometrial cancer.
IL-8 exerts its effects when it binds to the chemokine receptors CXCR1 and CXCR2 (26). This binding initiates many different signaling pathways, resulting in angiogenesis, mitogenesis and motogenesis. Furthermore, stimulating CXCR1 and CXCR2 activates two members of the RhoGTPase family, which in turn promotes polymerisation of the actin cytoskeleton. This leads to increased motility of tumour cells and invasion of carcinoma into underlying tissue (14). Overexpression of IL-8 by tumour cells attracts large numbers of leucocytes to the site of the tumour by chemotaxis. These leucocytes secrete growth factors and further promote tumor proliferation and growth (27)
Taking into consideration that on one hand IL-8 is correlated with visceral fat, which represents a risk factor for endometrial cancer, and on the other IL-8 promotes angiogenesis, control of IL-8 expression may be a valuable tool in designing new screening protocols and therapeutics for endometrial cancer.
Nevertheless, large-scale studies are needed to substantiate the accuracy and usefulness of IL-8 as a biomarker in endometrial cancer.
Conclusion
Plasma levels of IL-8 are positively linearly correlated with visceral fat. Determination of visceral fat in association with plasma IL-8 levels is a potential predictive factor for endometrial cancer.
Acknowledgements
This study was conducted with the support of Iuliu Haţieganu University of Medicine and Pharmacy, Cluj-Napoca, through financing contract no. 7020/14/15.11.2011.
- Received October 4, 2013.
- Revision received November 26, 2013.
- Accepted November 27, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}