


Abstract
Aim: The aim of this retrospective study was to evaluate bevacizumab combined with weekly paclitaxel with and without carboplatin in pre-treated patients with non-squamous non-small cell lung cancer (NSCLC). Patients and Methods: Between November 2009 and October 2011, 43 pre-treated patients with non-squamous NSCLC received bevacizumab (15 mg/kg, day 1) plus weekly paclitaxel (60-80 mg/m2, days 1, 8, 15) with carboplatin (area under the curve=4-5, day 1) (n=36), or bevacizumab plus weekly paclitaxel (n=7) alone every four weeks. Results: The response rate and disease control rates were 48.8% (21/43) and 86.0% (37/43), respectively. Median progression-free survival was 5.7 months, and overall survival was 14.5 months. Grade 3/4 neutropenia was observed in 37.2% of patients and peripheral neurotoxicity in 0%. No bevacizumab-related death was observed. Conclusion: Even for heavily pre-treated patients, bevacizumab plus weekly paclitaxel with or without carboplatin was effective and tolerable in non-squamous NSCLC.
Lung cancer is the leading cause of cancer death worldwide (1). Non-small cell lung cancer (NSCLC) accounts for approximately 80% of all lung cancers, and the majority are already unresectable and metastatic upon their initial diagnosis. Systemic chemotherapies are the primary therapeutic option for these patients (2). Cytotoxic chemotherapies such as platinum-based regimens have been commonly administered, but the advancement of cytotoxic agents has reached a plateau. Several molecular-targeted agents have been developed, and the inhibition of epidermal growth factor receptor (EGFR) or vascular endothelial growth factor (VEGF) pathways has been shown to provide with clinical benefits (3, 4). Among these agents, bevacizumab is a recombinant, humanized monoclonal antibody directed against VEGF, a key factor in tumor-associated angiogenesis. The survival benefit of bevacizumab with paclitaxel plus carboplatin has been established in the front-line setting for metastatic non-squamous NSCLC, as demonstrated in a randomized phase III trial (4). The efficacy of the same regimen has also been demonstrated in Japanese patients in a phase II randomized trial (5). In this trial, the overall response rate (RR) was 60.7%, and median progression-free survival (PFS) was 6.9 months in the bevacizumab-containing arm. Its notably high RR and long PFS encouraged us to adopt this regimen for pre-treated patients. However, little data exist on the efficacy and safety of bevacizumab therapy in pre-treated patients.
Although the efficacy of bevacizumab with paclitaxel-plus-carboplatin has been established as a front-line chemotherapy regimen, its role in the treatment of chemo-refractory patients remains unclear. Additionally, in heavily pre-treated patients, severe, frequent neutropenia and peripheral neurotoxicity are major concerns for the conventional tri-weekly paclitaxel used in this regimen. Weekly administration of paclitaxel can reduce such toxicities, but there are few data regarding a combination therapy of bevacizumab with weekly paclitaxel plus carboplatin.
The aim of our study was to evaluate the efficacy and safety of bevacizumab plus weekly paclitaxel with or without carboplatin in pre-treated patients with non-squamous NSCLC.
Patients and Methods
Patients. Between November 2009 and October 2011, 43 pre-treated patients with non-squamous NSCLC underwent treatment with bevacizumab plus weekly paclitaxel with carboplatin (n=36), or bevacizumab plus weekly paclitaxel (n=7) at our Institutes. The patients were retrospectively identified using medical records and radiographic records. Patients had an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 to 3, without any severe organ dysfunctions. We excluded patients who had contraindications for bevacizumab such as having a history of severe pulmonary hemorrhage, pulmonary cavitation, or tumor invasion to major blood vessels. Patients with brain metastases received the bevacizumab regimen after stereotactic radiotherapy or whole-brain radiotherapy, according to the results of the PASSPORT study (6). Patients who reported never smoking in their lifetime were defined as never-smokers. Those who had smoked within one year of the diagnosis were categorized as current smokers. The rest were considered former smokers. In cases with available tissue or cytological specimens, we isolated tumor DNA from various specimens, and EGFR mutation status was analyzed using the peptide nucleic acid-locked nucleic acid polymerase chain reaction clamp method, as previously reported (7).
Written informed consent for the chemotherapy with bevacizumab was obtained from all patients.
Treatment methods. Bevacizumab (15 mg/kg, day 1) plus paclitaxel (60-80 mg/m2, days 1, 8, 15) with carboplatin (area under the curve=4-5, day 1) was administered every four weeks. In elderly or patients with poor PS, the same dose of bevacizumab plus weekly paclitaxel was administered without carboplatin. After completion of 4-6 cycles of the combination chemotherapy, bevacizumab-alone was continued as a maintenance therapy. Dose reduction or interruption was employed when intolerable toxicities were observed. Therapy was continued until disease progression, intolerable toxicity, or patient withdrawal.
Evaluation of efficacy and toxicity. Baseline evaluations, including medical history, physical examinations, and laboratory tests, were performed. Evaluation of treatment response by computed tomography scan was repeated every 4-8 weeks according to the Response Evaluation Criteria in Solid Tumors (RECIST) Committee (8). If a patient was documented to demonstrate a complete response (CR) or a partial response (PR), confirmation was necessary after more than four weeks. Disease control was defined as the best tumor response in cases with CR, PR, or stable disease (SD) that was confirmed and sustained for at least eight weeks. The RR and disease control rate (DCR) were defined as CR+PR and CR+PR+SD ≥8 weeks, respectively. PFS was defined as the period from the start of treatment to the date when disease progression or death was observed. Overall survival (OS) was defined as the period from the start of the treatment to the date of death. Adverse events were graded according to the National Cancer Institute Common Toxicity Criteria (version 4.0) (9).
Statistical analysis. The survival distributions (PFS and OS) were estimated by the Kaplan–Meier method. Statistical analysis was performed using JMP 7 (SAS Institute Inc., Cary, NC, USA).
Results
Patients' characteristics. Between November 2009 and October 2011, 43 pre-treated patients with non-squamous NSCLC underwent bevacizumab plus weekly paclitaxel with carboplatin (n=36) or bevacizumab plus weekly paclitaxel (n=7), and were retrospectively evaluated at our Institutes. Table I shows the patients' characteristics. The median age was 63 (range, 48 to 80). Twelve (47%) patients were over 70 years old. The median number of prior regimens was 2 (range=1-10). Seventeen out of the 43 (40%) patients were never-smokers, and 30% of all patients had poor PS (2/3). Most patients were diagnosed with adenocarcinoma, but four cases of large-cell carcinoma and one of adenosquamous carcinoma were included. Thirteen patients harbored EGFR-sensitive mutations, 23 were wild-type, and in seven the mutation status was unknown.
Patients' characteristics.
Drug delivery. The median number of treatment cycles was four (range=1-13). Twenty-nine (67%) out of 43 patients received more than four cycles of the regimen. Dose reduction or interruption was employed in 22 (51%) patients due to toxicities.
Tumor response. Out of 43 patients, one showed CR, 20 PR, 16 SD, and 6 progressive disease, yielding an overall RR of 48.8% [95% confidence interval (CI)=33.3-64.5%] and a DCR of 86.0% (95% CI=72.1-94.7%).
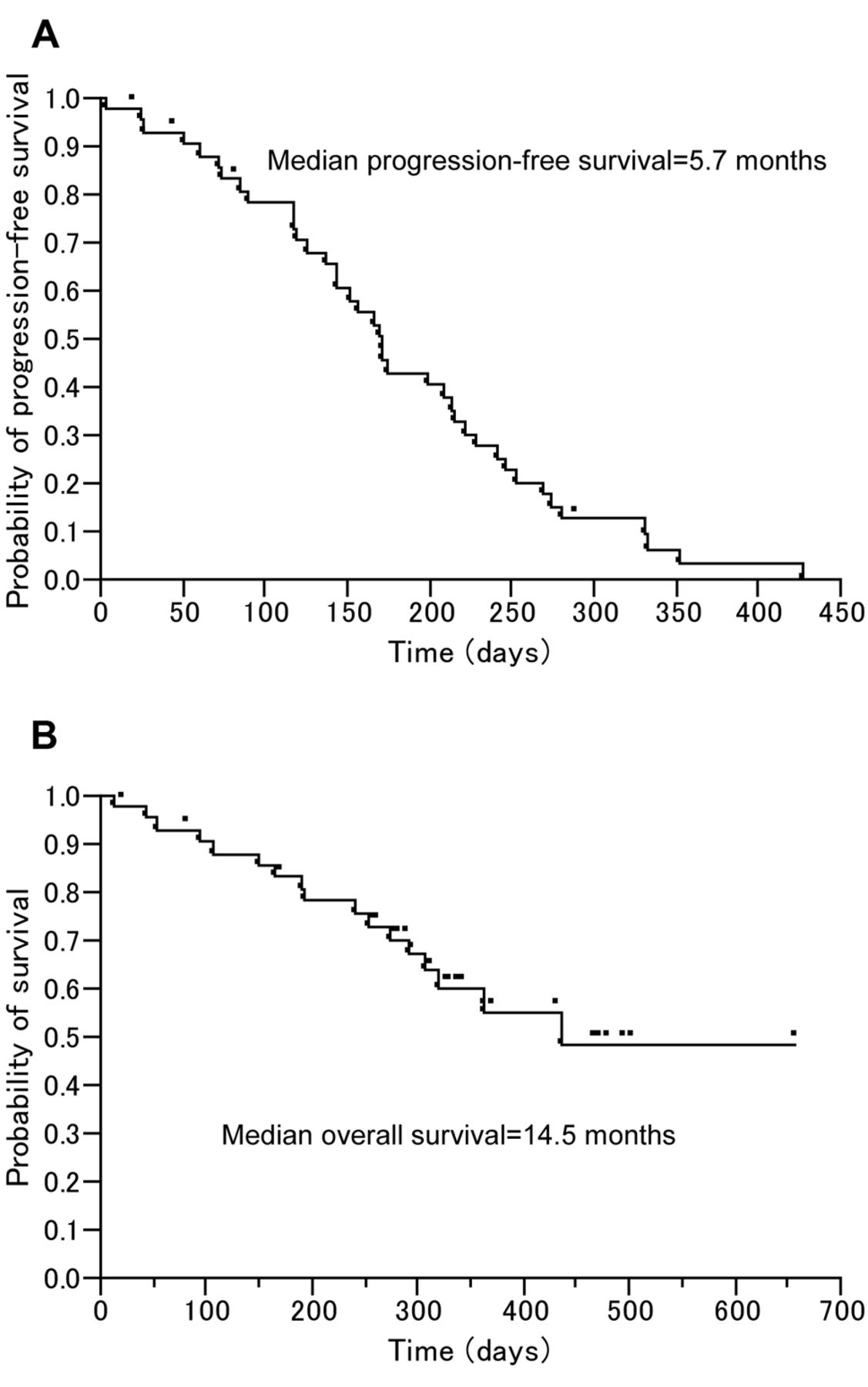
Survival. The median PFS was 5.7 months (95% CI=4.6-7.1 months; Figure 1a), and the median OS was 14.5 months (95% CI=9.7-undeterminable months; Figure 1b).

Curves of progression-free (A) and overall (B) survival.
Toxicity profile. The frequencies and grades of toxicities are shown in Table II. Grade 3/4 neutropenia and peripheral neurotoxicity were observed in 37.2% and 0% of all patients, respectively. Interstitial lung disease (grade 2) was observed in 1 (2.3%) out of 43 patients. Regarding bevacizumab-related toxicities, epistaxis and hypertension were observed in approximately 40% of patients. One (2.3%) grade 2 reversible brain hemorrhage was observed, but no severe thoracic bleeding or thromboembolism was confirmed. Reversible posterior leukoencephalopathy syndrome was suspected in one (2.3%) patient. There were no treatment-related deaths.
PFS with and without carboplatin. In patients who received bevacizumab plus weekly paclitaxel with carboplatin (n=36), the RR, DCR, and median PFS were 58.3% (95% CI=40.8-74.5%), 88.9% (95% CI=73.9-96.9%), and 5.8 months (95% CI=4.2-7.4 months), respectively. In patients who received bevacizumab plus weekly paclitaxel (n=7) - only, RR, DCR, and median PFS were 14.3% (95% CI=0.4-57.9%), 71.4% (95% CI=29.0-96.3%), and 4.8 months (95% CI=2.6-undeterminable months), respectively. PFS curves by treatment with or without carboplatin are shown in Figure 2.

Comparison of progression-free survival with and without carboplatin.
Case Report. We herein document one case with a good response to bevacizumab plus weekly paclitaxel with carboplatin despite heavy pre-treatment.
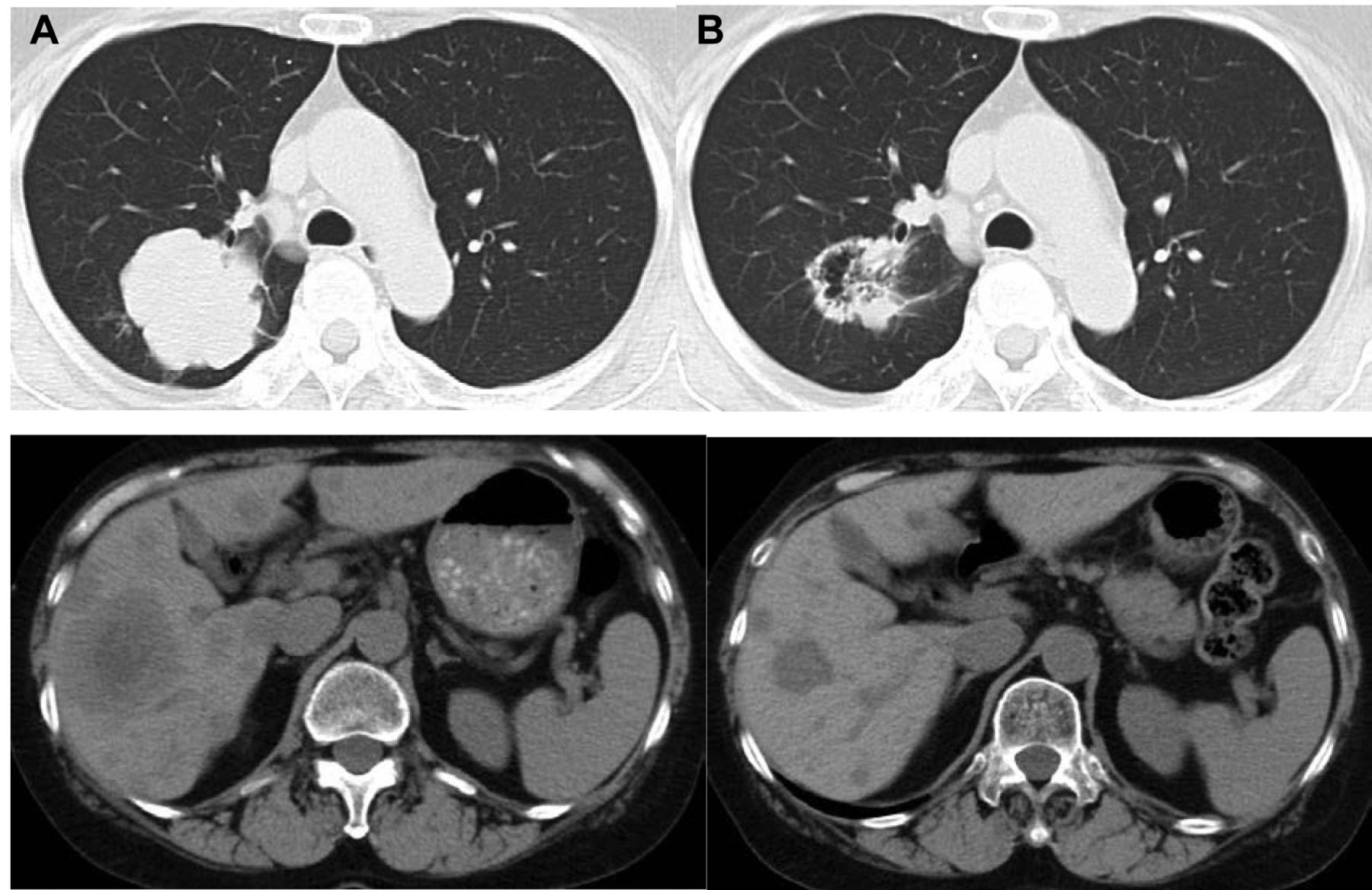
A 63-year-old woman was diagnosed with metastatic adenocarcinoma of the lung. She received cisplatin plus vinorelbine, gefitinib, and docetaxel, consecutively. After these regimens, she underwent multiple chemotherapies. Bevacizumab plus weekly paclitaxel with carboplatin was administered as the 11th line of chemotherapy, and PR was achieved for 5.2 months (Figure 3). The treatment was well-tolerated.
Discussion
Our present study demonstrates that the RR, DCR, median PFS, and OS were 48.8%, 86.0%, 5.7 months, and 14.5 months, respectively. In a randomized phase III trial conducted among Western populations (ECOG 4599) comparing paclitaxel plus carboplatin with or without bevacizumab, the RR, median PFS, and OS were 35%, 6.2 months, and 12.3 months, respectively, in the bevacizumab-containing arm (4). Similarly, Japanese investigators reported a randomized phase II trial (JO19907) in which the RR, DCR, median PFS, and OS were 60.7%, 94.0%, 6.9 months, and 22.8 months, respectively, in the bevacizumab-containing arm (5). Although our study included many heavily pre-treated patients, our present results are comparable to the results of these two studies of front-line settings utilizing bevacizumab with paclitaxel plus carboplatin. Similarly, some investigators reported the efficacy of bevacizumab plus paclitaxel with or without carboplatin in patients with chemorefractory disease. Tamiya et al. demonstrated the efficacy of bevacizumab with paclitaxel plus carboplatin where the RR, DCR, and median PFS were 47.6%, 71.4%, and 6.1 months, respectively (10). Also among patients with chemorefractory disease, Habib et al. showed the efficacy of bevacizumab with weekly paclitaxel where the RR, DCR, and median PFS were 15.0%, 75.0%, and 6.4 months, respectively (11).
Frequencies and grades of toxicities.
Bevacizumab and paclitaxel are commonly administered tri-weekly with carboplatin in front-line settings. However, conventional tri-weekly paclitaxel occasionally induces severe, frequent neutropenia and peripheral neurotoxicity, particularly in heavily pre-treated patients. Tamiya et al. used tri-weekly paclitaxel plus bevacizumab with carboplatin in heavily treated patients, and grade 3/4 neutropenia and neurotoxicity were 86% and 24%, respectively (10). In the JO19907 trial, grade 3/4 neutropenia and peripheral neurotoxicity were observed in 91.2% and 8% of all patients, respectively (5). We, thus, adopted weekly paclitaxel plus carboplatin with bevacizumab to reduce these toxicities. Consequently, grade 3/4 neutropenia and peripheral neurotoxicity were observed in 37.2% and 0% of our patients. Several reports have demonstrated that weekly administration of paclitaxel plus carboplatin reduces neurotoxicity and neutropenia, while maintaining efficacy (12, 13). In the Japanese phase II trial, the prevalence of grade 3/4 neutropenia was 88% in the conventional tri-weekly paclitaxel arm vs. 41% in the weekly paclitaxel arm, and the respective rates of grade 3/4 peripheral neurotoxicity were 25% vs. 0%. Our study included not only heavily pre-treated patients but also patients with poor PS and elderly patients; nevertheless, the chemotherapy was generally well-tolerated. Especially for frail patients, we administered the same dose of bevacizumab with weekly paclitaxel without carboplatin. The results for bevacizumab plus weekly paclitaxel were only slightly inferior to those for bevacizumab plus weekly paclitaxel with carboplatin, except for the lower response rate. Bevacizumab plus weekly paclitaxel without carboplatin can be a treatment option for previously treated frail patients, such as patients with poor PS or the elderly.
Interestingly, the superiority of weekly administration of paclitaxel has been demonstrated in other types of cancers. In ovarian cancer, the superiority of weekly paclitaxel plus carboplatin has been demonstrated over the conventional tri-weekly paclitaxel plus carboplatin (14). Similarly, in breast cancer, the superiority of weekly paclitaxel has been demonstrated over the conventional tri-weekly paclitaxel in an adjuvant setting (15). These data encouraged us to explore the combination therapy of weekly paclitaxel and bevacizumab.

Chest computed tomography before (A) initiation of the regimen and after two cycles (B) of therapy.
Only a few reports exist regarding the use of a bevacizumab-containing chemotherapy in relapse/chemorefractory settings. Herbst et al. suggested the efficacy of additional bevacizumab to salvage agents such as erlotinib, docetaxel, or pemetrexed for pre-treated patients (16). Due to the small sample size, their results were not statistically significant, but the median PFS (4.4 vs. 3.0 months) and OS (13.3 vs. 8.6 months) tended to be better compared to the use of these salvage agents without bevacizumab. Heist et al. also reported the efficacy of a combination therapy consisting of oxaliplatin, pemetrexed, and bevacizumab (17). In their study, the RR, median PFS, and median OS were 27%, 5.8 months, and 12.5 months, respectively. Our regimen palliated some patients' cancer-related symptoms, including the presented case. Considering the higher RR and longer PFS with a bevacizumab-containing regimen, its use in relapse settings is potentially effective for palliation of cancer-related symptoms such as cancer pain, even in heavily pretreated patients.
In a pre-clinical investigation, paclitaxel appeared to have a better synergistic effect than other cytotoxic drugs in combination with bevacizumab (18). Additionally, paclitaxel has demonstrated a clinical benefit with bevacizumab in other kinds of cancers. A randomized phase III trial among patients with breast cancer demonstrated that weekly paclitaxel plus bevacizumab had a higher efficacy compared to weekly paclitaxel alone (19): higher RR (48.9% vs. 22.2%) and longer PFS (11.3 vs. 5.8 months) were shown in the bevacizumab-containing arm. Two randomized phase III trials involving patients with ovarian cancer also demonstrated the efficacy of the addition of bevacizumab to therapy with paclitaxel plus carboplatin (20, 21). These pre-clinical and clinical data suggest a synergism between paclitaxel and bevacizumab.
Several NSCLC guidelines recommend single-agent chemotherapies such as gefitinib, erlotinib, docetaxel, or pemetrexed for second- and third-line treatments. However, the use of these agents without bevacizumab in pre-treated patients resulted in RR, DCR, and median PFS of approximately 10-20%, 30-50%, and 2-3 months, respectively (3, 22-24). These results are not satisfactory for salvage therapies. Therefore, we should explore more active regimens for previously treated patients. We consider bevacizumab-containing regimens to be promising salvage therapies. In fact, Herbst et al. showed the efficacy of adding bevacizumab to salvage agents such as erlotinib, docetaxel, or pemetrexed (16). Our regimen and Heist et al.'s regimen, which consist of a tolerable and effective platinum regimen with bevacizumab, are good candidates for more active salvage therapies.
In conclusion, bevacizumab plus weekly paclitaxel with or without carboplatin was effective and well-tolerated in non-squamous NSCLC, even for heavily pre-treated patients. Weekly administration of paclitaxel reduced neutropenia and neurotoxicity, while maintaining efficacy, in combination with bevacizumab. However, our study is retrospective and of a small sample size, RR and PFS are very ‘soft’ end-points, and the RR and PFS were assessed by the investigators. In addition, the interval for restaging imaging was highly variable, and this represents a bias for PFS assessment. Bevacizumab-containing chemotherapies for previously treated patients warrant further prospective studies. We are therefore planning a phase II trial to investigate the efficacy and safety of bevacizumab with weekly paclitaxel plus carboplatin for patients with chemorefractory disease.
Acknowledgements
We thank Mr. David Martin for his writing support.
Footnotes
-
Conflicts of Interest
None declared.
- Received October 10, 2013.
- Revision received November 18, 2013.
- Accepted November 20, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}