


Abstract
The mechanisms responsible for the poor prognosis of pregnancy-associated breast cancer (PABC) remain not well-understood. We studied angiogenesis and lymphangiogenesis as they are known prognostic factors in breast cancer. We conducted a case control study of breast cancer comparing women with and without PABC matched for age and histological parameters. Surgical specimen sections were immunostained with anti-CD31 for angiogenesis and anti-D2-40 for lymphangiogenesis, then analyzed using vessel density, ratio of the vascular area and the Chalkley count. Seventeen patients with PABC and 22 controls were included. Angiogenesis was significantly increased in tumor tissues, and tended to be higher in healthy breast tissues from the PABC group compared to controls. In contrast, no difference between the two groups was found concerning lymphangiogenesis both in tumor and healthy breast tissues. Pregnancy enhances angiogenesis in breast cancer. This phenomenon appears to explain the poor prognosis of PABC.
The incidence of several malignancies has increased in the Western world during the past decades, also showing a trend to occur at an earlier age. In addition, women tend to delay childbearing in developed countries. These factors probably contribute towards a higher occurrence of pregnancy-associated cancer (1). However, the consequences of pregnancy on malignant tumors remain currently poorly understood. Indeed, the secretion during gestation of multiple hormones and growth factors with pleomorphic effects may influence the proliferation of quiescent but mutated stem or initiating cells and affect the growth of an already established tumor as well as kinetics of the stromal reaction and angiogenesis. Breast cancer (BC) is one of the most frequent carcinoma associated with pregnancy, together with melanoma and cervix cancer (2). Pregnancy-associated breast cancer (PABC) is defined as BC diagnosed during pregnancy or in the year following delivery (3). It occurs in 1 in 10,000 to 3,000 pregnancies in developed countries and concerns 2.6% to 7% of all BC occurring among women under 45 years of age, but up to 15.6% in women younger than 35 (1, 4, 5). Compared with classical BC, PABC appears larger in size at diagnosis, although lymph node invasion does not appear to be more frequent (2, 5). Studies with large cohorts found an increased risk of cancer-associated death in women with PABC compared with non-PABC patients, with a hazard ratio (HR) from 1.23 to 1.95 after adjusting for age or for age and initial extent of disease (2, 6). Again, after adjusting for age and tumor size but also stage, hormonal receptor status and race, Rodriguez found a marginally-significant excess of cancer-associated death in patients with PABC (HR=1.14, p=0.046) (7). Women diagnosed with PABC during the post-partum period had a worse outcome (2, 4), with prognosis improving as time-from-delivery increased (8). Of note, in a recent cohort of 652 patients younger than 35 years, no difference in the mortality rate between women with PABC and women with non-PABC was found (5).
Some studies have focused on the mechanisms underlying the poor prognosis in PABC. A delay in diagnosis has been hypothesized. However this cannot be the only factor, as a worse outcome is still observed after adjusting for tumor size. The behavior of tumors can be modified in the context of pregnancy. In PABCs, we and others have reported a higher frequency of hormone-negative tumors (5, 7, 9) and we found a higher frequency of tumors over expressing human epidermal growth factor receptor-2 (HER2) (9). The expression of molecules associated with wound healing and inflammation in the extracellular matrix (ECM) of the mammary gland during involution was also proposed, as such molecules stimulate tumor progression and metastasis (10, 11). Angiogenesis and lymphangiogenesis play a major role in various types of tumors including BC. Indeed, BCs with a high degree of angiogenesis and lymphangiogenesis translate to a poorer outcome (12-16). Moreover, in recent studies from our laboratory, melanoma during pregnancy, both in women and in murine models, was characterized by an increase in lymphatic and blood vessel angiogenesis (17). This increase appeared to be due to circulating factors during pregnancy, although they have not yet been identified. Because of the influence of gestation on stromal angiogenesis, we aimed to assess angiogenesis and lymphangiogenesis in women with PABC as compared with control women with BC matched for age and histological characteristics.
Patients and Methods
Patient selection. All women surgically-treated at the Tenon University Hospital, Paris, France, from January 1, 2008 to December 31, 2010 for primary mammary carcinoma were selected from a prospective database. Patients who were treated with chemotherapy prior to surgery were excluded to avoid bias due to treatment-induced modifications. For each patient, the age and the following tumor characteristics were recorded: tumor size, node involvement, histological type, grade according to the Elston and Ellis classification (18), hormonal status, expression of HER2, proliferation rate determined by Ki-67 staining and presence of lymph vascular space invasion (LVSI). Women for whom the diagnosis of BC was made during pregnancy or the year following the delivery (PABC) were defined as cases. Control patients were selected from the women with BC who were not pregnant nor had delivered in the year before the surgery. They were matched with the cases for age (±2 years) and the following histological characteristics: histological type, grade, hormonal status, HER2 expression and Ki-67 rate.
Immunostaining. For each patient enrolled in the study, four paraffin-embedded sections were rigorously selected by a breast pathologist (MA): two of a representative sample of the tumor and two of the healthy breast tissue. Angiogenesis was analyzed using the antibody to Cluster of Differentiation 31 (CD31) (1:200; Dako, Glostrup, Denmark), while lymphangiogenesis was studied through the antibody to Podoplanin (D2-40) (1:100; Dako). Slides were observed under an Eclipse 90i microscope (Nikon Corporation, Tokyo, Japan). Images were obtained using a DS-Fi1c camera (Nikon Corporation) and analyzed with the NIS-Elements software (Nikon Corporation). All analyses were performed by a single investigator blinded to the clinical characteristics (ASG).
Evaluation of angiogenesis. Examination was performed on sections stained with antibody to CD31. For each slide, three foci of high vascular density (hotspots) were selected at low magnification (×40 and ×100) and then analyzed at high magnification (×200). For each hotspot, three different parameters were analyzed: the microvessel density (MVD), the proportion of the area that stained positively for CD31 (CD31 ratio) and the Chalkley count of CD31-stained vessels. For the MVD and the CD31 ratio, the study area consisted of an image of 1.2×106 μm2 obtained by the camera. The MVD resulted from counting the number of CD31-stained vessels in the field of this large image. The CD31 ratio was evaluated with the NIS software, which measures the labeled surface in the detailed image. The Chalkley count was analyzed directly under the microscope using a 25-point grid (22 mm Chalkley eye piece reticule; NG52, Electron Microscopy Sciences, Hatfield, PA, USA) as previously described (12, 13). The final data were determined as the means of the three hotspot scores for each method of evaluation. Data were obtained from the tumor tissue and from the healthy breast tissue.
Tumor characteristics of the entire study population.
Evaluation of lymphangiogenesis. The lymphatic vessel density (LVD), the proportion of the area that stained positively for D2-40 (D2-40 ratio) and the Chalkley count of D2-40-stained vessels were evaluated similarly to that described above on D2-40-stained sections.
Statistical analysis. Categorical variables were compared using the Chi-square test. Mean values were analyzed using the Mann-Whitney test. A p-value of less than 0.05 was considered significant.
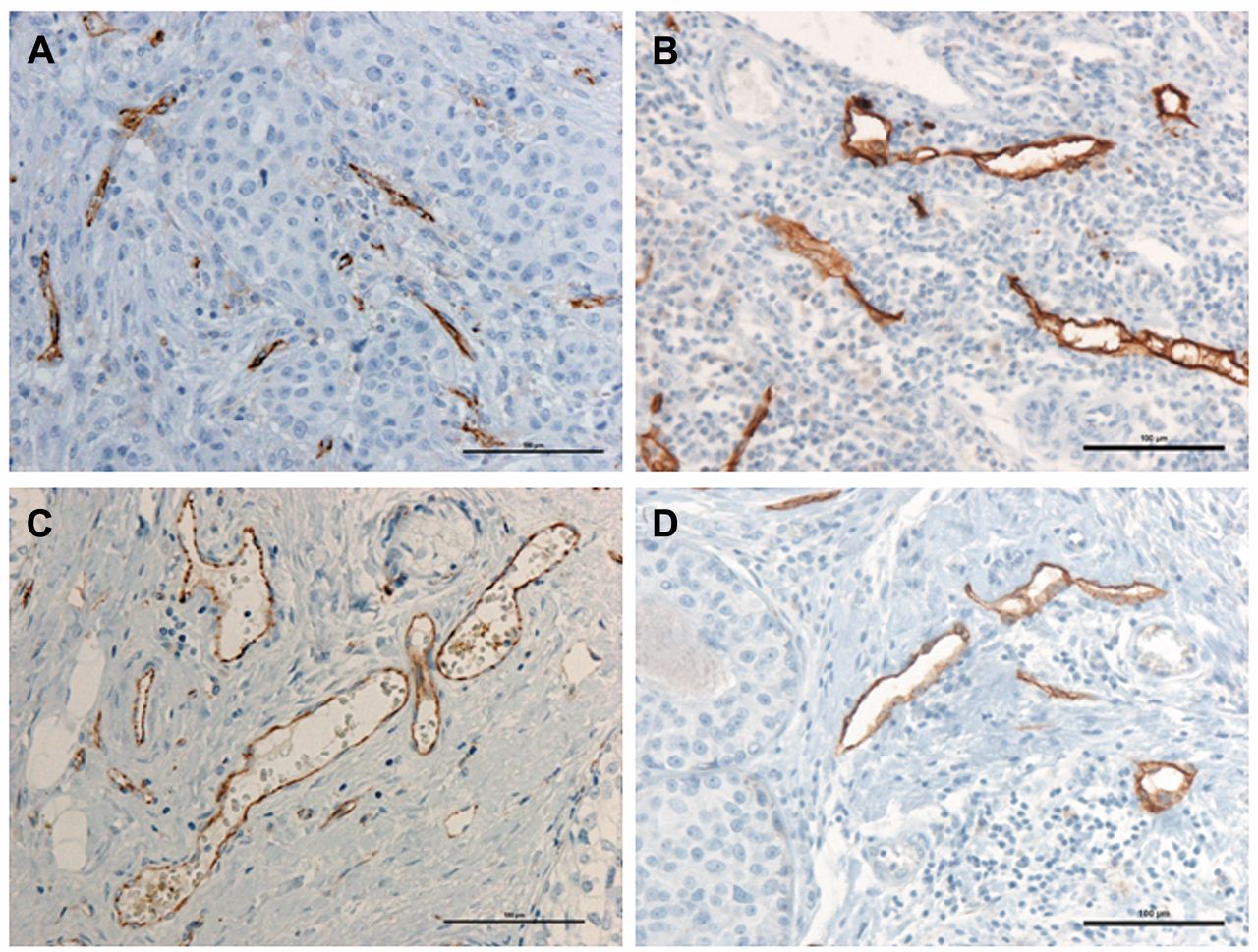
Immunostaining with antibodies against cluster of differentiation-31 (CD31) (blood vessels, A and C) and podoplanin (D2-40) (lymphatic vessels, B and D), ×200 magnification, scale bar=100 μm; A and B: intra-tumoral, C and D: peri-tumoral.
Ethical standards. All patients gave informed consent authorizing the use of surgical specimens for scientific purposes.
Results
Seventeen patients with PABC were enrolled in the study and were compared against 22 control patients with BC matched for age and histological characteristics. Among the PABC patients, seven were pregnant and 10 were in the post-partum period at the time of diagnosis. The characteristics of the study population are shown in Table I. The two groups were comparable for all the studied criteria. Within the tumor tissues, both blood and lymphatic vessels predominated in the periphery adjacent to the tumor and were generally larger in size than the intra-tumoral vessels (Figure 1). The tumor vascularity was analyzed within these tumor stromal vessels.
Breast tumor angiogenesis is enhanced in PABC. Blood vessel angiogenesis was significantly higher in the tumors from the PABC group than in the controls, using all three techniques of measurement. The means for the PABC and control patients were: MVD=77.6 vs. 59.4/section (p=0.04), CD31 ratio=0.62 vs. 0.41% (p=0.03), and Chalkley CD31=6.4 vs. 5.5/section (p=0.04) (Figure 2A), respectively. Importantly, these differences in angiogenesis parameters were correlated with pregnancy-only and never with other clinical or histological characteristics (Table II).
Breast tumor lymphangiogenesis appears not to be affected by pregnancy. No difference was observed between PABC and control patients with regard to lymphangiogenesis. The means for the PABC and controls were: LVD=14.1 vs. 14.0/section (p=0.68), D2-40 ratio=0.30 vs. 0.32% (p=1.00), and Chalkley D2-40=4.9 vs. 4.7/section (p=0.93) (Figure 2A), respectively. No relationship between lymphangiogenesis and the clinical and histological tumor characteristics was observed (Table III).
Angiogenesis and lymphangiogenesis in healthy breast tissue. In healthy breast tissue, angiogenesis seemed to be higher in tumors from the PABC group than in the controls, with a significantly higher CD31 ratio (0.28 vs. 0.18%, p=0.02), a trend for a higher MVD, although not significant (54.6 vs. 46.1/section, p=0.30), but no difference was observed concerning the Chalkley count (5.9 vs. 5.8/section, p=0.65) (Figure 2B). No significant difference was observed in lymphangiogenesis between healthy breast tissues from PABC and control patients (Figure 2B).
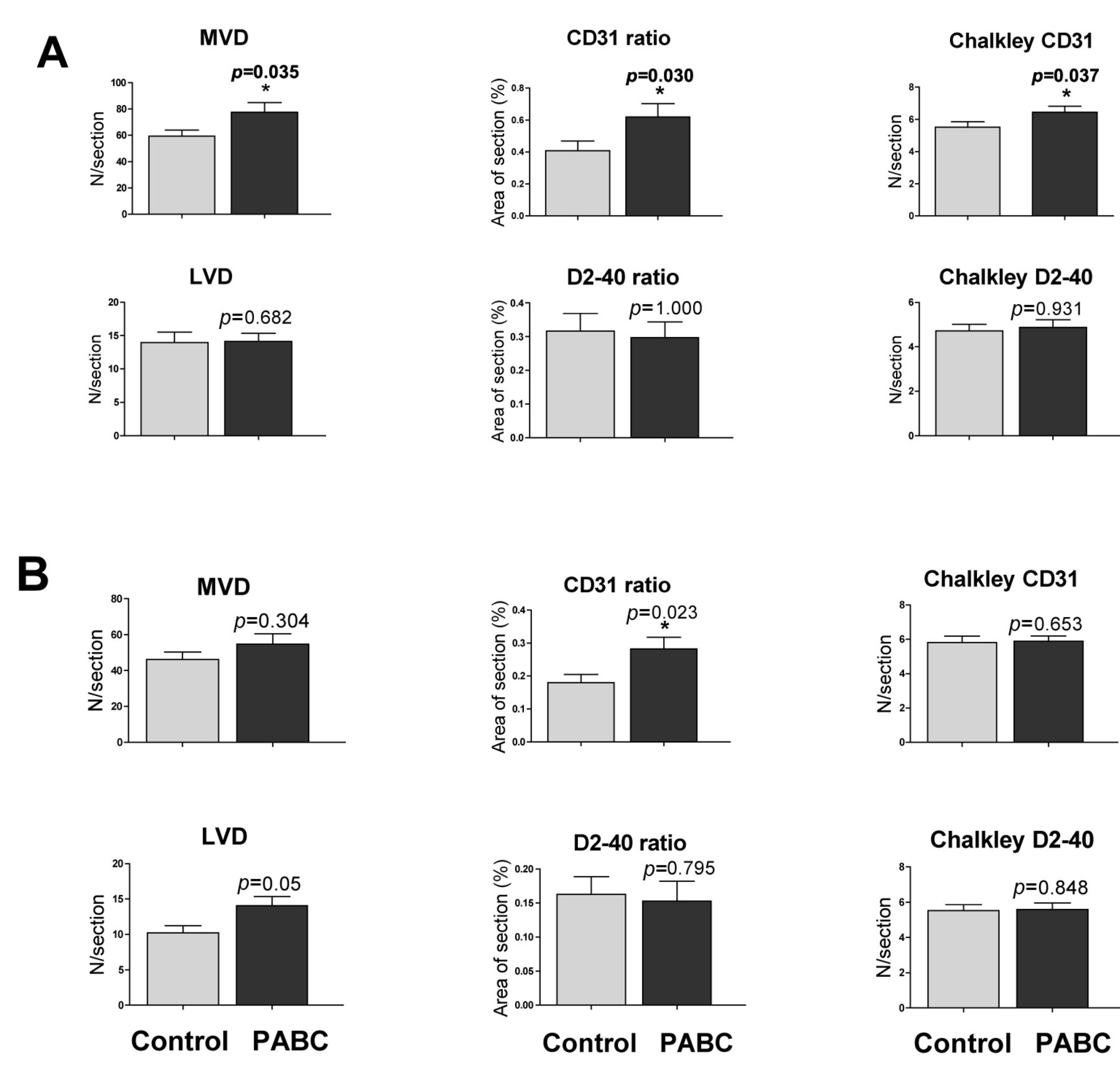
Comparison of angiogenesis and lymphangiogenesis according to the patient status pregnancy-associated breast cancer (PABC) or control. The results are presented as the means±SEM (vertical bar). MVD, Microvessel density; CD31 ratio, percentage of the section that stained positively for CD31; LVD, lymphatic vessel density; D2-40 ratio, percentage of the section that stained positively for D2-40. A: Tumor tissue; B: healthy breast tissue.
Discussion
In the current study, we analyzed PABC because BC is one of the most frequent malignancies occurring during pregnancy (2). Since the prognosis of PABC appears to be poorer compared to non-PABC (2, 6-8), there is a need for translational studies that investigate the behavioral status of BC in the context of pregnancy. Our aim was original since we planned to evaluate the influence of pregnancy on the BC stroma rather than on the tumor clone itself, as far as we are aware, for the first time.
In this case control study, we found that tumors from patients with PABC had a significant increase in blood vessel angiogenesis compared to classical BC. These data appear robust as all three in situ techniques indicated a 30% increase in blood vessel angiogenesis in PABC. In previous studies, angiogenesis has been reported to be an independent marker of poor prognosis in BC (12-14). In all of these studies, neoangiogenesis was considered to be a consequence of the tumor itself but was not related to the host characteristics. In contrast, we believe that the increased stromal tumor angiogenesis that we observed in PABC was due to the pregnancy-associated status. Indeed, our two study groups had significant differences neither in the local tumor stage, nor in the tumor histological characteristics, including hormone receptor status. Furthermore, angiogenesis also appeared to be increased in the non-affected breast tissue of patients with PABC. Another parameter from breast tumor stroma that may be implicated is that of the ECM (10, 11, 19). In an in vitro model, ECM from involuting mammary gland of rats inhibited the ductal development in normal mammary cells but rather promoted invasion of tumor cells, whereas the ECM of mammary gland of nulliparous rats had the opposite effects (11). In vivo, in female rats, the injection of tumor cells with ECM from involuting breasts led to an increase in metastasis through increased angiogenesis when compared with the injection of tumor cells with ECM from the breasts of nulliparous rats (11). Our data fit well with the enhanced angiogenesis observed in normal, pre-malignant or tumor skin analyzed during gestation (20, 21).
Comparison of the mean measurements of tumor angiogenesis according to the clinical and histological characteristics.
Lymphangiogenesis was reported to be correlated with reduced overall survival in patients with BC (15, 16). In our population we found that lymphangiogenesis was not affected by gestation in either the tumor or the healthy breast tissue. This result was in contrast to what we previously observed for melanoma (17). However, our finding may have been influenced by discrepancies in the two study groups. Indeed, although the difference did not reach significance, the control patients were more likely to have node-positive disease (62%) than the PABC patients (38%, p=0.24), and were more positive for LVSI than the PABC patients (56% vs. 23%, p=0.07). As lymphangiogenesis correlates with LVSI and nodal invasion (15, 16), we therefore cannot exclude the possibility that a true increase in lymphangiogenesis could have been induced by pregnancy but was not detected in our study.
During normal pregnancy, there is an increase of several angiogenic factors secreted by the placenta such as placental growth factor (PlGF), vascular endothelial growth factor A (VEGFA) and FMS-like tyrosine kinase 1 (Flt1) (22). Pregnancy also leads to the transfer of fetal progenitors that may participate in the angiogenesis of maternal injured tissues such as wound healing (23) or melanoma (24). Gestational serum was also found to stimulate the secretion of VEGFA by melanoma cells, although it was not possible to assign this property to a specific molecule (17). Therefore, we speculate that the mixture of pregnancy-secreted factors stimulates the proliferation of normal and tumoral breast, either directly or through modification of the paracrine repertoire of the carcinoma. In pre-eclampsia, angiogenic factors normally increased during pregnancy such as PlGF, VEGF and Flt1 are found at lower levels, whereas anti-angiogenic factors such as soluble Flt1 or soluble endoglin are increased (22). Interestingly, women with pre-eclampsia are less likely to develop cancer later than women without pre-eclampsia, indicating a long-term anti-tumoral effect of reduced angiogenesis during pregnancy (25-27). Our results together with these data point towards the effect of gestation on tumoral tissues. Finally, in BC, the anti-angiogenic drug bevacizumab is used with benefits in the metastatic stage (28, 29). Adjuvant bevacizumab has also demonstrated benefit (30, 31). Currently, all anti-angiogenic therapies are contraindicated during pregnancy because of their toxicity profile, including high blood pressure, proteinuria in humans and pre-eclampsia in pregnant mice (22). However, since most cases of PABC were diagnosed during the post-partum period, the question of the use of antiangiogenic agents early in the therapy strategy for patients with PABC could be raised.
Comparison of the mean measurements of tumor lymphangiogenesis according to the clinical and histological characteristics.
Acknowledgements
We express our thanks to Anita Rodenas for technical support in immunostaining.
Footnotes
-
↵* These Authors contributed equally to the study and should both be considered as senior authors.
-
Funding
ASG was the recipient of an Assistance Publique-Hôpitaux de Paris grant for the study. The work was also supported by the Institut National du Cancer and the Réseau Cancers Associés à la Grossesse.
- Received October 15, 2013.
- Revision received November 18, 2013.
- Accepted November 20, 2013.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}