


Abstract
Background: The aryl hydrocarbon receptor (AhR) is a ligand-activated transcription factor which translocates from the cytoplasm to the nucleus after activation. AhR overexpression is positively associated with epidermal growth factor (EGFR) expression in non-small cell lung cancer (NSCLC). The association between AhR expression and types of EGFR mutation, and the prognostic value of AhR expression in NSCLC remain unclear. Patients and Methods: The AhR expression and detection of L858R and E746-750A deletion of EGFR in NSCLC was assessed using immunohistochemistry. Results: Nuclear translocation of AhR was more common in females, non-smokers, adenocarcinoma (AD) and NSCLC patients with EGFR E746-750A deletion. The overall median survival time (MST) was 20.4 months for patients with NSCLC, 21.8 months for these with AD and 15.4 months for these with squamous cell carcinoma (SQ). The MST was significantly reduced in patients with poor performance status, SQ or advanced cancer stage. AhR nuclear translocation was associated with cancer death in SQ (hazard ratio=3.714, p<0.001) but not in AD (hazard ratio=0.837, p=0.407). Conclusion: Nuclear translocation of AhR was associated with EGFR mutation, and conferred a poor prognosis for patients with lung SQ.
Lung cancer is an important cause of cancer death worldwide, including Taiwan (1). Adenocarcinoma (AD) and squamous cell carcinoma (SQ) are the major histological types of lung cancer and constitute about 80% of all non-small cell lung cancers (NSCLC) (2). Survival of patients with lung cancer can be predicted by classic clinical features consisting of age, gender, tumor histology, cancer stage at diagnosis, and surgical treatments (3, 4). It is well-known that cancer stage is a powerful predictor of patient survival and disease prognosis. Although some molecular markers have recently been associated with lung cancer survival (5-8), histology-associated factors for survival remain to be determined and need further investigation.
Cigarette smoking and environmental toxicants are the major etiologies of lung cancer. The involvement of the aryl hydrocarbon receptor (AhR) signaling pathway in lung carcinogenesis is supported by both animal and clinical studies (9-12). AhR is a ligand-activated transcription factor associated with xenobiotic and drug metabolism in humans. AhR is present in the cytoplasm and is associated with a complex of heat-shock protein-90, X-associated protein-2, and p23 (13). While ligand binding, AhR is translocated to the nucleus, where it forms a heterodimer with the AhR nuclear translocator (14) and transactivates the genes of several phase-I and phase-II drug/xenobiotic-metabolizing enzymes, including cytochrome P450 1A1 and 1B1 (CYPs) (15). AhR-regulated enzymes participate in activation or detoxification of some chemical carcinogens, such as 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) and benzo[a]pyrene (16). In addition, AhR modulates expression of some oncogenes including myelocytomatosis viral oncogene (c-MYC), rel reticuloendotheliosis viral oncogene homolog A (RELA), factor kappa-light-chain-enhancer of activated B cells (NFκB) and rat sarcoma (RAS) (17-19). We demonstrated that the reduction of AhR expression inhibited anchorage-independent growth of lung cancer cells, and cytoplasmic AhR expression was more common in lung AD than SQ (20). Another clinical study showed that increased CYP expression in bronchial cells of smokers was associated with poor prognosis among patients with NSCLC (21). However, based on our comprehensive literature review, there are no data discussing the association between AhR expression and survival of patients with NSCLC.
Epidermal growth factor receptor (EGFR), a tyrosine kinase receptor of the erythroblastic leukemia viral oncogene (ERBB) family, has intrinsic tyrosine kinase activity, which is involved in the behavior of malignant cells when they mutate (22). Patients with NSCLC with EGFR mutations have a good response to EGFR tyrosine kinase inhibitors (TKIs) (5, 23). Approximately 90% of EGFR mutation types are the EGFR L858R mutation in exon 21 and E746-750A deletion in exon 19 (24). Molecular techniques such as direct DNA sequencing, real-time polymerase chain reaction (PCR), and the scorpion-amplified refractory mutation system have been used to identify EGFR mutations (25). Mutation-specific monoclonal antibodies against the E746-750A deletion or L858R mutation of the EGFR have been developed and been used in immunohistochemistry (IHC) (26). Many studies have demonstrated good correlation between the molecular techniques and IHC staining for the detection of EGFR mutations (27-29).
Increasing evidence from animal studies and cell models has shown that toxicities induced by AhR ligands such as TCDD are associated with AhR activation and EGFR phosphorylation (30-32). AhR nuclear translocator is involved in EGF regulation of cancer cells (33). Nonetheless, we found no study showing the relationship between AhR expression status and EGFR mutation type. Cytoplasmic AhR expression indicates AhR induction; AhR expression in the nucleus indicates the nuclear translocation of AhR. The CYP1B1 gene is a downstream marker for the AhR signaling pathway; therefore, CYP1B1 expression indicates activation of AhR through induction and nuclear translocation of AhR. We demonstrated positive associations between cytoplasmic AhR expression and CYP1B1 or EGFR expression in NSCLC (34). In this study, we investigated the association of AhR expression status with EGFR mutation types in NSCLC.
To elucidate the survival-associated factors including tumor histology and expression status of AhR and EGFR mutation types for NSCLC, we performed IHC on tissue microarrays (TMA). We now understand the relationships and effects of AhR and CYP1B1 expression on survival in NSCLC.
Patients and Methods
Study subjects and tissue microarray constructs. From 1998 to 2008, we identified 251 patients with NSCLC who were treated at the Chung Shan Medical University Hospital, and their lung tumor tissues were available for study. Approximately 30% of the patients were enrolled in our previous studies (34). TMAs were constructed using 251 paraffin tissue blocks obtained from the Department of Pathology. These lung cancer tissues were obtained during surgery or by core biopsy, and each tissue core was 1 mm or 2 mm in diameter. Of the TMAs constructed, all samples were investigated for AhR and CYP1B1 by IHC techniques. Only 178 cases collected from 2006 to 2008 were assessed for EGFR mutation IHC. This study was approved by the Institutional Review Board of the Chung Shan Medical University Hospital and those whose tissue samples were studied gave informed consent for this work approval (numbers: CS05091, CS09158).
Clinical features. The clinical features at diagnosis of gender, age, performance score, smoking history, tumor histology, chemotherapy of TKIs, and cancer stage were verified either from the hospital medical records or by telephone interview. Performance score, also called Eastern Cooperative Oncology Group (ECOG) score, ranged from 0 to 5, with 0 denoting perfect health and 5, death. Smoking history was recorded as “yes” or “no”. “No” smoking history was defined as those who had never smoked previously. Individuals who currently smoked, or had ever smoked, were counted as “yes” (smokers). For this study, only patients with SQ and those with AD diagnosed according to the World Health Organization classification criteria (35) were enrolled. Patients with other tumor histological types were excluded because of the small number of cases. The samples were divided into stages I to IV according to the TNM (tumor, node, metastasis) criteria outlined in the Cancer Staging Manual from the American Joint Committee on Cancer (36). Only 36 patients had received the TKI therapy in this study and most of them had stable disease after TKI therapy.
Immunohistochemistry. The IHC protocols for AhR and CYP1B1 expression, and mutation-specific antibodies for EGFR L858R in exon 21 and E746-750A deletion in exon 19 have been previously reported (27, 34). The TMA section slides were de-waxed with xylene and rehydrated with decreasing ethanol concentrations and ending with distilled water. Antigen retrieval was accomplished in a citrate buffer (pH 6.0) for 20 min using a pressure cooker (Cell Marque Corp, Hot Springs, AZ, USA). The primary antibodies used were against AhR (1:200 dilution; Biomol, Plymouth Meeting, PA, USA), CYP1B1 (1:1500 dilution, clone WB-1B1; Gentest Corp., Woburn, MA, USA), EGFR L858R (1:150 dilution, clone 43B2; Cell Signaling Technology, Danvers, MA, USA) and EGFR ΔE746-750A (1:150 dilution, clone 6B6; Cell Signaling Technology), which were used by incubation with slides for 8-16 h at room temperature. The secondary linked antibody and the polymer-peroxidase conjugate (Thermo Fisher Scientific, Cheshire, UK) were then incubated with the slides for 10 min each. The slides were stained with diaminobenzidine (Thermo Fisher Scientific) and counterstained with hematoxylin (Muto Pure Chemicals, Tokyo, Japan) for detection. Positive controls were lung tissues which had EGFR L858R or EGFR ΔE746-750A detected by nested PCR and DNA sequencing. Negative controls were prepared using normal serum or phosphate-buffered saline instead of the primary antibody.
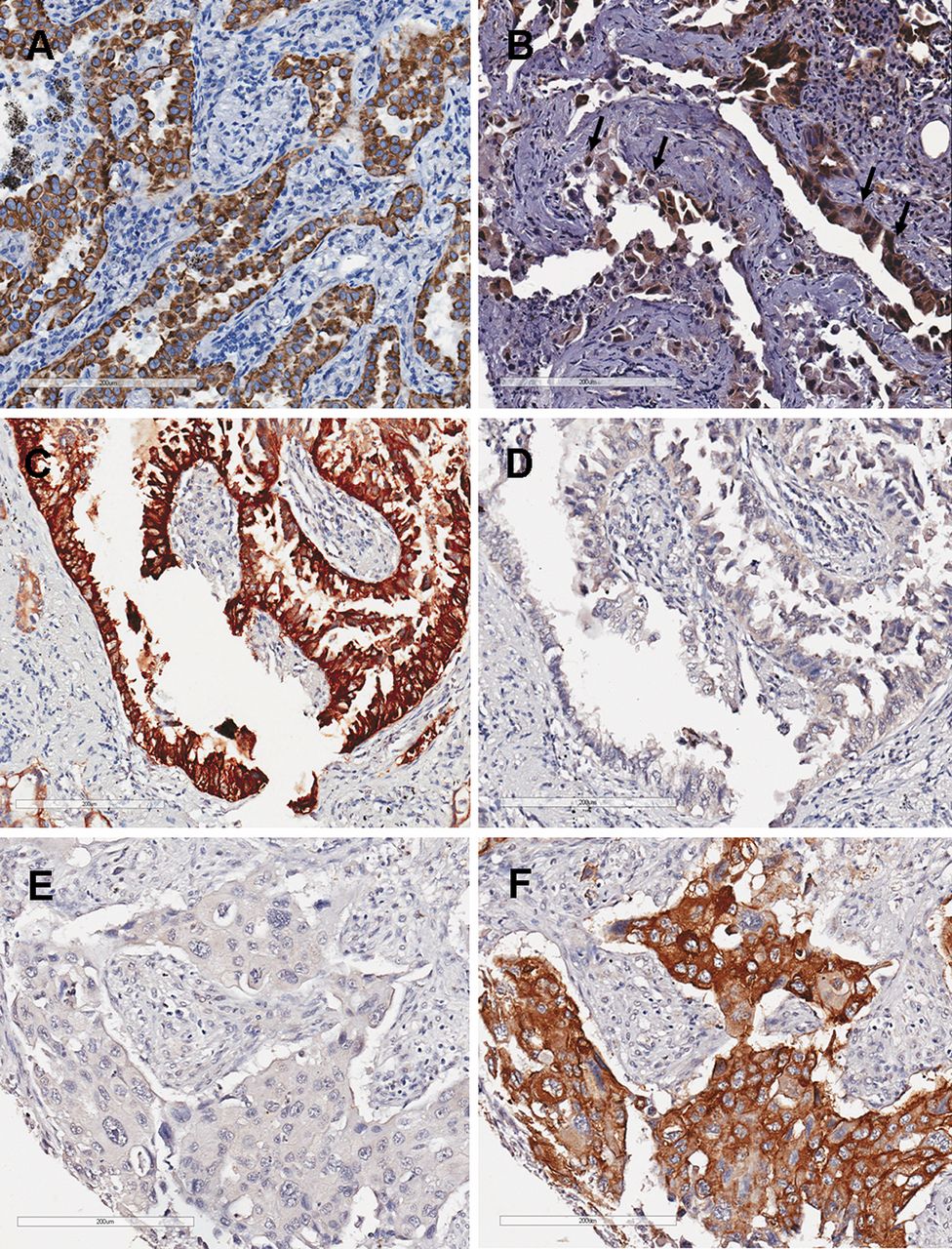
Assessment of AhR, CYP1B1, EGFR L858R mutation, and EGFR E746-750A deletion. Immunoreactivity of each biomarker was assessed by the staining intensity and proportion of stained tumor cells in each tissue core on the TMA arrays. AhR was expressed in cytoplasm or in nucleus (Figure 1, A and B). The levels of CYP1B1 expression, and detection rates of EGFR L858R and EGFR E746-750A deletion were assessed using cytoplasmic staining (Figure 1, C–F). All AhR, CYP1B1, EGFR L858R, and EGFR E746-750A deletion immunostains reacted negatively with stroma.
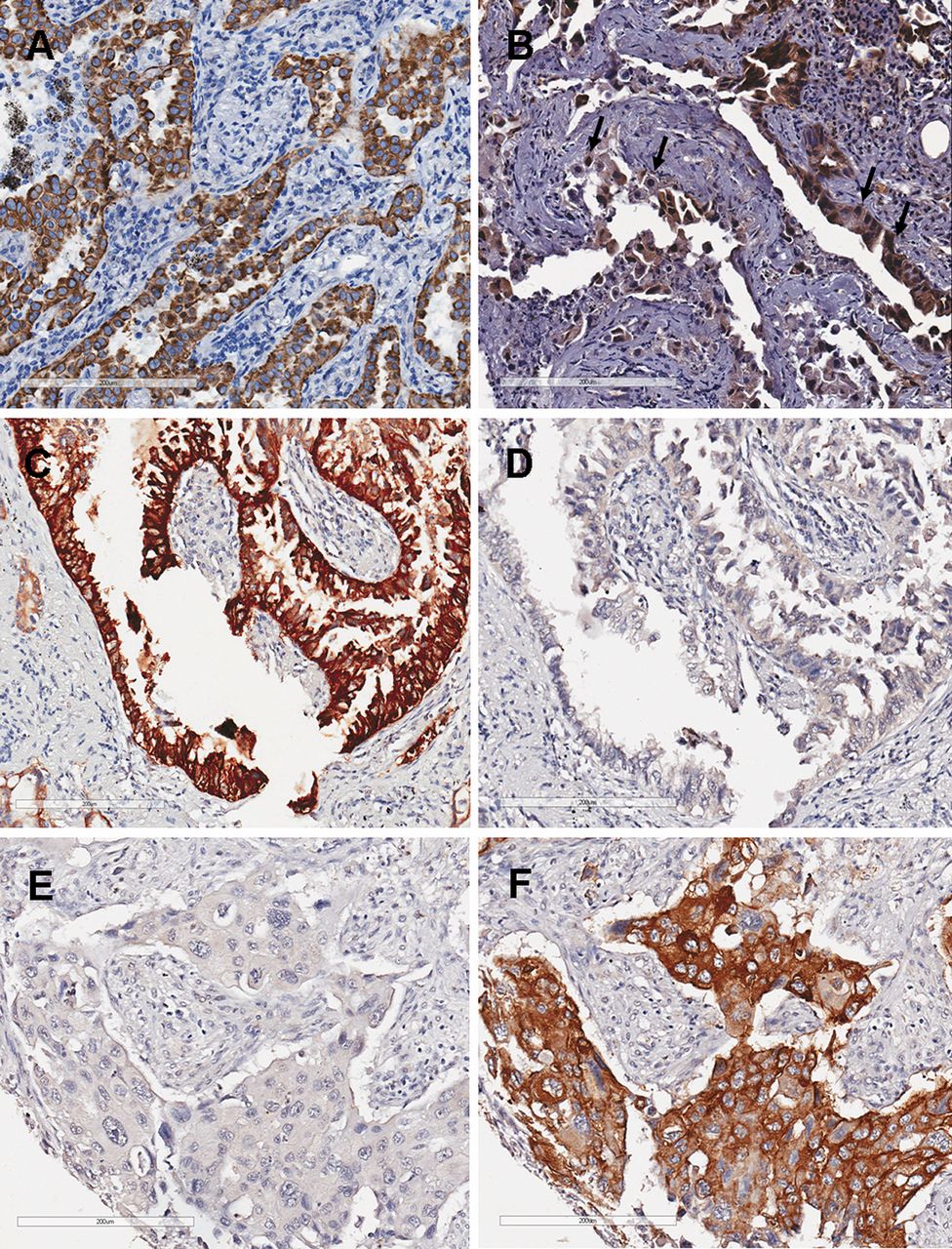
Immunohistochemistry for aryl hydrocarbon receptor (AhR), epidermal growth factor receptor (EGFR) L858R mutation, and EGFR E746-750A deletion in non-small cell lung cancer. A: Adenocarcinoma cells exhibit diffuse high AhR expression in the cytoplasm, but not in the nuclei. B: Adenocarcinoma cells exhibit strong AhR expression in the nuclei (arrow) and low AhR expression in the cytoplasm. C: Adenocarcinoma cells exhibit strong immunoreactivity in the cytoplasm for the EGFR L858R mutation. D: For the same case as shown in C, this adenocarcinoma cells exhibit negativity for the EGFR L858R mutation. E: Squamous cell carcinoma cells with negative immunoreactivity for the EGFR E746-750A deletion. F: For the same case as shown in E, this squamous cell carcinoma cells exhibit strong immunoreactivity in the cytoplasm for the EGFR E746-750A deletion. Bar=200 μm.
For the cAhR staining, when the mean staining intensity of the tumor cells was stronger than that most bronchiolar epithelium (basal level of AhR) (12), the tumor was defined as a cytoplasmic AhR-overexpressing (cAhR+) tumor. For nuclear AhR staining, when the tumor contained more than 10% of tumor cells with nuclear staining intensity stronger than that of the stroma, the tumor was defined as a nuclear AhR-positive (nAhR+) tumor. Conversely, tumors with mean staining intensity less than that of the bronchiolar cells or with fewer than 10% nAhR+ cells were recorded as cAhR− or nAhR− tumors. For CYP1B1 staining, when the mean staining intensity of the cytoplasm of the tumor cells was stronger than that of the vascular wall (basal level of CYP1B1) (37), the tumor was defined as CYP1B1-overexpressing (CYP1B1+). For immunostaining to detect EGFR L858R and EGFR E746-750A deletions, when the mean cytoplasmic intensity of the tumor cells was stronger than that of the stroma (negative for EGFR mutations), the tumor was defined as an EGFR-mutation-positive (L858R+ or E746-750A del+) tumor. The mean cytoplasmic intensities of AhR, CYP1B1, EGFR L858R, and EGFR E746-750A deletions were quantified using MetaMorph imaging software (Molecular Devices Corp., Downington, PA, USA).
Biomarkers associated with clinical features.
Statistical analysis. At the time of our analysis in October 2012, out of the 251 patients with NSCLC, 172 had died. The follow-up period (mean=25.2 months) was defined as the time from cancer diagnosis to the patient's death or our last contact. Descriptive statistics were used to calculate the frequencies of all the clinical features, including age, gender, performance score, smoking history, tumor histology, chemotherapy of TKIs, and TNM cancer stage at diagnosis. Fisher's exact test and the chi-square test were performed to examine the associations between AhR or EGFR mutation types and the clinical features. The Kaplan–Meier plot and log-rank test were used to compare the expression patterns of AhR, level of CYP1B1, and clinical variables, and to determine the cumulative survival rates and median survival time. Multivariate Cox regression testing was used to identify the independent prognostic factors. A two-sided p-value of <0.05 was considered significant. All the statistical operations were performed using the SPSS (version 14.0) statistical software package (SPSS, Inc., Chicago, IL, USA).
Results
The relationships between clinical features and biomarker detections for the 178 patients with NSCLC are shown in Table I. There were 112 cases of AD and 66 cases of SQ. Most patients at diagnosis were healthy or symptomatic but completely ambulatory (ECOG performance scores 0-1). Male patients, the elderly, smokers, and cases with advanced cancer stages were predominant.
Expression patterns of AhR, levels of CYP1B1, and mutation types of EGFR associated with clinical features. Out of 178 patients with NSCLC, the cAhR+ rate was 44.9% and the nAhR+ rate was 46.1%. The EGFR mutation rate was 39.9%, including 28 cases of L858R mutation, 46 cases of E746-A750 deletion, and three cases of both L858R mutation and E746-A750 deletion; and the remaining patients had wild-type EGFR (Table I). Nuclear AhR expression and detection of EGFR mutations predominated in women. Cytoplasmic expression of AhR showed no gender difference. The AhR expression status was associated with smoking history or tumor type; in other words, nuclear AhR expression was commonly present in patients who never smoked or had AD type NSCLC (Table I). As stratified by EGFR mutation type, the EGFR L858R mutation, but not E746-A750 deletion, was associated with AD tumor histology and smoking history. In this cohort, the EGFR E746-A750 deletion was frequently detected in stage I/II cancer (Table I).
Aryl hydrocarbon receptor (AhR) expression status and epidermal growth factor receptor (EGFR) mutation type by tumor histology.
Associations among AhR, CYP1B1, and EGFR mutations. We previously demonstrated the association between cytoplasmic AhR expression and EGFR expression in NSCLC (34). In the present study, cAhR+, nAhR+, and EGFR-L858R-mutated cases had similar clinical features (Table I). Therefore, we investigated the associations between AhR expression status and EGFR mutation types. As shown in Table II, high cytoplamic AhR and nuclear AhR expression were associated with the E746-750A deletion type of EGFR mutation, but not the L858R mutation, in NSCLC. In addition, nuclear AhR expression was associated with cytoplasmic AhR and CYP1B1 overexpression, supporting the status of AhR activation (data not shown). Therefore, these results suggest that AhR activation was associated with the E746-750A deletion type of EGFR mutation in NSCLC.
Biomarkers associated with overall survival of patients with NSCLC. In order to enhance the power of statistics, the case number was increased to 251 cases for assessing the potential survival effect on patients with AhR- and/or CYP1B1-expressing tumors. Out of the 251 patients with NSCLC, the median overall survival time was 20.4 months (Table III). The log-rank analysis showed negative effects for patients with ECOG performance scores of 2 to 4 (p=0.029), SQ type NSCLC (p=0.044), and advanced cancer stage (p<0.001). The level of CYP1B1 expression showed no effect on patient survival. When stratified by tumor type, nuclear AhR expression had a negative effect on survival of patients with SQ (Figure 2A), but not in those with AD (Figure 2B).
Nuclear AhR expression as a hazard factor for death of patients with NSCLC. Multivariate Cox regression testing was used to identify the prognostic value of several factors for NSCLC patients. When adjusted for covariables, only cancer stage was an independent prognostic factor in this cohort. When stratified by tumor type, nuclear AhR expression had a hazard ratio of 3.714 (p<0.001) for cancer death in cases with SQ (Table IV). In other words, only cancer stage was an independent prognostic factor for AD; in contrast, nuclear AhR expression and cancer stage were independent prognostic factors for SQ (Table IV).
Discussion
This study focused on the association between AhR expression and survival of patients with NSCLC. After adjustment for covariables, cancer stage was still the most powerfully independent predictor of prognosis in this cohort. Nonetheless, the data shows that patients with nAhR+ lung SQ had shorter survival time and poorer disease prognoses in contrast to patients with lung AD, for which nuclear AhR showed no survival effect. CYP1B1 was not associated with patient survival or disease prognosis. Our results for overall survival were similar to those reported in other epidemiological studies in Taiwan, showing that survival times ranged from 365 days to 624 days (38, 39). In Taiwan, lung tumor histology is associated with patients' smoking history, with SQ commonly occurring in smokers and AD in non-smokers (34). Cigarette smoke, one of the major etiologies of lung cancer, is composed of many kinds of mitogens, cancer promoters, and carcinogens; some of them are involved in lung toxicity and carcinogenesis via metabolic activation by CYP induced by liganded AhR (40, 41). The data also showed that nuclear AhR expression was associated with cytoplasmic AhR and CYP1B1 overexpression, supporting the status of AhR activation. The functions of activated AhR have proven to be directly or indirectly involved in cell proliferation, cell-cycle arrest, and apoptosis during the process of tumorigenesis (42). Oyama et al. further demonstrated that increased CYP (CYP1A1, CYP2A6, CYP2E1) and AhR expression in the bronchial epithelium of patients with NSCLC who had smoked heavily were biomarkers for poor survival in those with stage I disease, particularly for those with SQ type NSCLC (21). In contrast, AhR overexpression had a protective effect on lung AD cells and reduced oxidative stress induced by cigarette smoke and increased G0/G1 cell cycle-arrest via the p53-p21-Rb1 signaling pathway (43). This evidence supports the present findings that nuclear translocation of AhR is associated with a poor prognosis in SQ type, but not in AD type NSCLC.
Clinical features and nuclear aryl hydrocarbon receptor (AhR) expression associated with patient overall survival.
Nuclear aryl hydrocarbon receptor (AhR) expression associated with the prognosis for non-small cell lung cancer (NSCLC)

Overall survival according to aryl hydrocarbon receptor (AhR) expression status and tumor histology. Nuclear AhR (nAhR+) expression is significantly associated with cancer death in patients with squamous cell carcinoma of the lung (A), but not in those with adenocarcinoma (B).
Mutant EGFR induces oncogenic effects mediated mostly by signal transducer and activator of transcript (STAT) proteins and interleukin-6 (IL-6), leading to anti-apoptosis and cell proliferation (44, 45). Additionally, the nuclear AhR-RELA complex activates NFκB promoter, which subsequently up-regulates IL-6 expression (43). Gao et al. demonstrated that mutant EGFR, but not wild-type EGFR, had this effect on cell growth mediated by STAT activation and IL-6 up-regulation in human lung AD cells (44). Furthermore, patients with NSCLC with EGFR-mutated AD had good responses to EGFR TKIs (5, 23). Cancer cells with mutant EGFR sensitive to TKIs, such as gefitinib and erlotinib, are targets for mutant EGFR for degradation, which could be mediated by heat-shock protein 90 (46). Li et al. demonstrated that TKIs are metabolized by CYP3A and CYP1A1, but not by CYP1B1, in human liver and non-hepatic tissues (47). Hughes et al. showed that CTP1A1/1A2-mediated metabolism was induced by increasing erlotinib dosing in patients with AD type NSCLC who were current smokers (48). These findings suggest that EGFR mutations affect not only EGFR signaling pathways, but also AhR signal transduction.
Cisplatin-based drugs are used in the treatments of NSCLC. The ATP-binding cassette sub-family G member 2 (ABCG2) protein, a kind of transporter, is associated with the removal of some anticancer drugs (e.g. doxorubicin, mitoxantrone) from cancer cells (49). In cisplatin-resistant esophageal SQ cells, AhR activation leads to induction of ABCG2 and concomitant resistance of 5-fluorouracil and irinotecan (50). These findings indicate that the AhR expression or activation is related to the effects of some anticancer drugs on SQ cells. The relationship between AhR expression status and drug sensitivity remains to be investigated.
In NSCLC, both nuclear and cytoplasmic AhR expression was associated with CYP1B1 expression. Nuclear AhR expression was a negative factor for survival in patients with SQ. This observation implies that AhR antagonists are more appropriate for patients with SQ and TKIs for those with AD, to improve survival of patients with NSCLC. Thus, it should be possible to predict the risk of cancer formation accurately and design plans for the prevention and treatment of lung cancer depending on tumor histology.
Acknowledgements
This work was supported by research grant NSC 96-2320-B-040-016-MY3 from the National Science Council, Taiwan, R.O.C. We thank Pi-Chen Huang for technical support.
Footnotes
-
Conflicts of Interest
No financial or personal relationship disclosures are required for any of the Authors.
- Received June 12, 2013.
- Revision received July 4, 2013.
- Accepted July 8, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}