


Abstract
Uric acid in serum (S-UA) is produced by the breakdown of the cellular nucleic acids of leukemia cells, and may be a marker of disease aggressiveness. S-UA levels were examined for association with clinical outcomes in patients with acute myeloid leukemia (AML). Fifty-six patients with AML admitted to our Institution were evaluated retrospectively. The median S-UA level at diagnosis was 5.0 mg/dl (range 2-13.8 mg/dl). The S-UA levels did not correlate with peripheral lactate dehydrogenase, peripheral white blood cell counts, or peripheral blast counts, and were not proportional to bone marrow blast counts or marrow cellularity. The S-UA levels in the patients who achieved complete remission were slightly lower than those in those who did not. S-UA levels less than, or equal to the median (5.0 mg/dl) were significantly associated with better prognoses, compared with S-UA levels greater than 5.0 mg/dl. Thus, the S-UA level may predict the prognosis of AML, and is a versatile and cost-effective test for such a purpose.
A high rate of proliferation and a high tumor burden cause the rapid lysis of cancer cells (1-3). Cell lysis leads to the release of intracellular contents, which include electrolytes, proteins, and nucleic acids into the bloodstream (1-3). Because purine nucleic acids are subsequently catabolized to uric acid (UA), the serum UA (S-UA) concentration reflects the breakdown of cancer cells, and is a marker of increased cellular turnover (1-4).
Acute myeloid leukemia (AML) is a cancer of myeloid cells, characterized by the rapid proliferation of leukemic blasts that accumulate in the bone marrow and infiltrate the entire body. The standard induction chemotherapy regimen achieves complete remission (CR) rates of over 70% in young adult patients with AML (5-7). However, the remission is not durable, and long-term survivors account for only 40% of young adult patients with AML. Thus, it is important to predict the therapeutic outcome, which will then allow the individualization of the treatment modality.
Parameters that can predict the prognosis of AML have been widely investigated (8-11). Karyotypic and genetic analyses are most important, because they are closely associated with leukemogenesis. The detection of minimal residual disease using fusion genes, such as PML-RARA, RUNX1-RUNX1T1, and CBFB-MYH11, and the less specific WT1 may predict for disease relapse. Multiparameter flow cytometry may also be useful in detecting minimal residual disease. However, more versatile markers may be more cost-effective and easier to implement in the clinic. Based on the rapidly proliferating nature of AML, S-UA may be a candidate marker of the aggressiveness of the disease, and thus may be a predictor of prognosis.
The present retrospective study focused on the S-UA levels in patients who were newly-diagnosed with AML and received remission induction chemotherapy. The S-UA levels were evaluated in association with other parameters and, ultimately, with the prognosis of the disease.
Patients and Methods
Patients. Patients who were admitted to the University of Fukui Hospital between January 2005 and May 2011 were considered for this study. This retrospective study was approved by the Ethics Committee of the University of Fukui Hospital (#686). The patients were all newly diagnosed with AML (those with acute promyelocytic leukemia were excluded) and received remission induction chemotherapy. To obtain the diagnosis, bone marrow samples were aspirated and evaluated using standard techniques, including hemograms, cell surface marker detection, and karyotyping. The classification of AML was made according to the French–American–British criteria (12). Patients of 65 years old or younger received standard “3+7” induction chemotherapy, including a continuous intravenous infusion of 100 mg/m2 cytarabine on days 1-7 and 30-minute intravenous infusion of 12 mg/m2 idarubicin on days 1-3. These patients received 3-4 courses of postinduction chemotherapy when they achieved CR. Patients older than 65 years received reduced doses of the “3+7”, a low-dose cytarabine-based regimen, or barasertib in a phase I study (13) according to the physicians' choice. CR was defined as the normalization of the blood and bone marrow, including the disappearance of blasts, a granulocyte count >1,000/μl, and a platelet count >100,000/μl in the peripheral blood, as well as normocellularity with ≤5% blasts in the bone marrow (14). Other responses were considered failures.
Measurement of S-UA levels. Peripheral blood samples were drawn from the patients at diagnosis and were analyzed for UA levels in-house using a TBA-c16000 automatic analyzer (Toshiba, Tochigi, Japan). The normal range was 3.4-7.0 mg/dl.
Statistical analyses. All of the statistical analyses were performed using Microsoft Excel 2007 software (Microsoft, Redmond, WA, USA). All of the graphs were generated using GraphPad Prism software (version 5.0) (GraphPad Software, Inc. San Diego, CA, USA). Each comparison was evaluated by the Mann-Whitney two-tailed test. Values of p≤0.05 were considered statistically significant.
Results
Patients' characteristics. Between January 2005 and May 2011, 58 patients with AML received remission induction chemotherapy. Out of these patients, two who had already been treated for their hyperuricemia with allopurinol were excluded. The characteristics of the remaining 56 patients are shown in Table I.
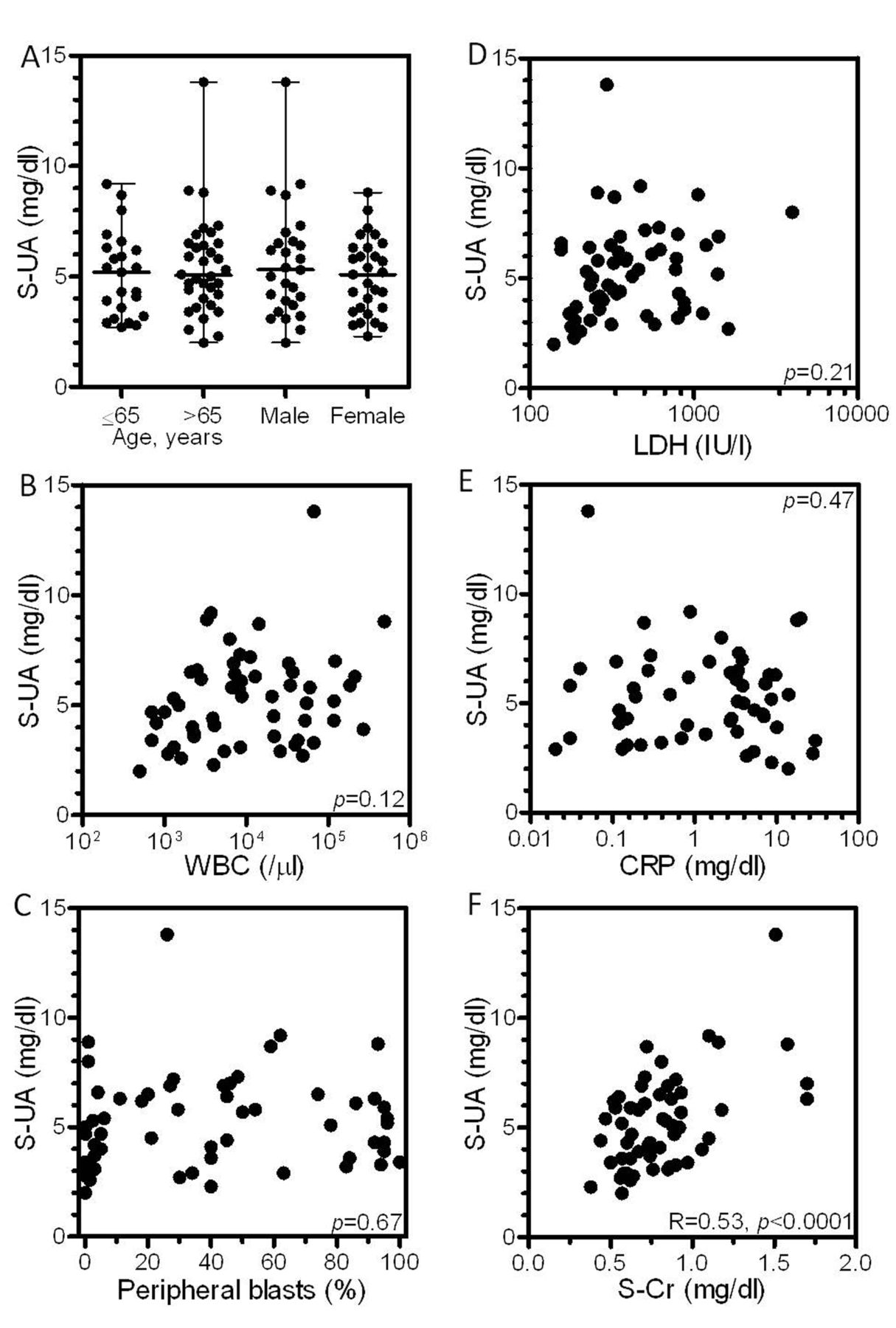
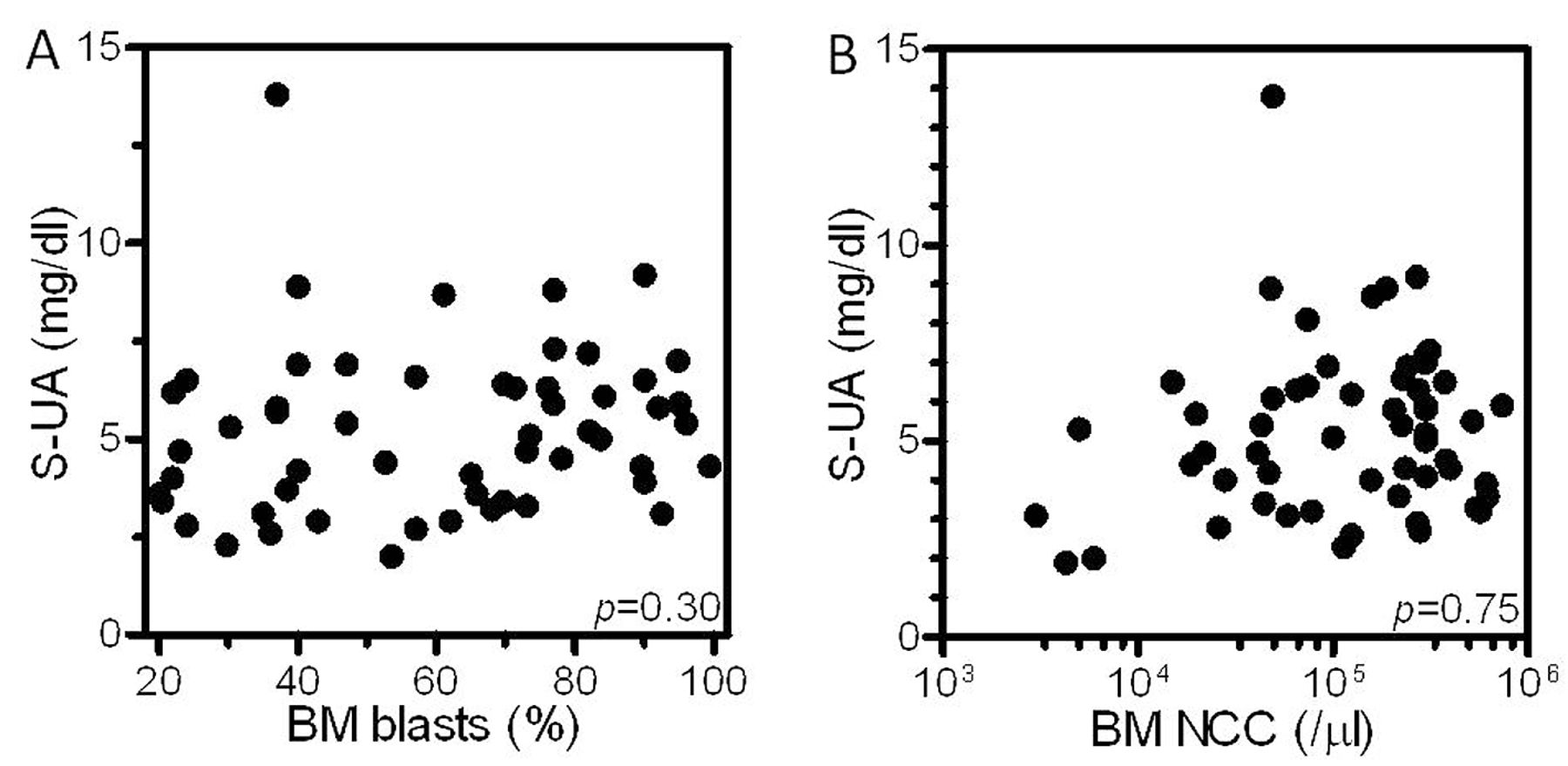
S-UA levels and leukemia parameters. The median S-UA level at diagnosis was 5.0 mg/dl with a range between 2 and 13.8 mg/dl, suggesting a wide variability among patients. Eight patients (14.3%) had hyperuricemia (>7.0 mg/dl) at diagnosis (Figure 1). The S-UA levels were not associated with the patients' age or gender (Figure 1A). The S-UA levels were not correlated with peripheral white blood cell counts, peripheral blast counts, lactate dehydrogenase levels, or C-reactive protein levels (Figures 1B-E). Correlation was only found between the S-UA and serum creatinine concentrations (Figure 1F), which suggests that the increase in S-UA was caused by under-excretion due to renal dysfunction in some patients. The S-UA levels were not proportional to bone marrow parameters, including marrow blast counts and marrow cellularity (Figure 2).
S-UA levels and the outcomes of induction treatments. Thirty-five out of 56 patients (62.5%) achieved CR. The median S-UA in the patients who achieved CR was 4.7 mg/dl, while the value was 5.8 mg/dl in the patients who did not (Figure 3A), although the difference was not significant. The median serum creatinine in the patients who achieved CR was 0.76 mg/dl, while the value was 0.73 mg/dl for those who did not (Figure 3B). When the median S-UA concentration (5.0 mg/dl) was used as a cut-off, S-UA ≤5.0 mg/dl was significantly associated with a better survival rate, compared to the group with S-UA >5.0 mg/dl (Figure 3C). In contrast, when the median serum creatinine concentration (0.73 mg/dl) was used as a cut-off, the prognosis did not differ by the serum creatinine concentration (Figure 3D), suggesting little contribution of renal function to the therapeutic efficacy.
Patients' characteristics.
Discussion
The majority of patients with AML experience disease relapse, despite high remission rates after induction treatment (5,6). Risk classification and monitoring for minimal residual disease are crucial to the optimization of post-remission treatment. Death of proliferating leukemia cells leads to the overloading of purine nucleic acids in the blood of the patients. These purine nucleotides are subsequently catabolized to hypoxanthine, xanthine, and, finally, UA by xanthine oxidase (15, 16). The present study investigated S-UA as a marker of aggressiveness of AML by examining its association with therapeutic outcomes.
The levels of UA, adenosine deaminase, and C-reactive protein in serum were found to be significantly higher in patients with head and neck cancer compared with the levels in controls (p<0.001) (4). The UA level was also observed to rise with staging (4). The estimation of the UA level may facilitate diagnosis and assessment of the severity of the disease in patients with head and neck carcinoma (4). In AML, Tsimberidou et al. evaluated the prognostic significance of several parameters, including UA, in 1,180 patients with AML (17). In their multivariate analysis, a performance status >1, β2 microglobulin >3 mg/dl, UA greater than the upper limit of normal, and lactate dehydrogenase >1.5-times the upper limit of normal, were the top five adverse independent factors predicting poorer survival in patients >60 years (17).

Serum uric acid (S-UA) levels according to patients' characteristics. S-UA levels and other peripheral parameters were tested for correlation. A: S-UA levels and age or gender. Lines represent the median values and the bars the range values. B: S-UA levels and white blood cell counts. C: S-UA levels and peripheral leukemic blast counts. D: S-UA levels and lactate dehydrogenase (LDH) levels. E: S-UA levels and C-reactive protein (CRP) levels. F: S-UA levels and serum creatinine levels.

Serum uric acid (S-UA) levels according to patients' characteristics. S-UA levels and bone marrow parameters were tested for correlation. A: S-UA levels and bone marrow leukemic blast counts (BM blast). B: S-UA levels and bone marrow nucleated cell counts (BM NCC).

Serum uric acid (S-UA) levels and therapeutic efficacy. S-UA levels and therapeutic outcomes were tested for correlation. A: S-UA levels and the outcomes of remission induction therapy. B: Serum creatinine (Cr) levels and the outcomes of remission induction therapy. Lines represent the median values and the bars the range values. C: S-UA levels and overall survival determined using the Kaplan–Meier method. D: Serum Cr levels and overall survival determined using the Kaplan–Meier method.
In the present study, we demonstrated that high UA levels were associated with a poor prognosis in AML. This result is consistent with the findings reported by Tsimberidou et al. (17). Only 14.3% of the patients had hyperuricemia, although the UA should reflect the burden of AML blasts or proliferating potential. In our previous report, the S-UA levels of 195 patients with hematological malignancies were studied (18). Hyperuricemia was found in 30.2% of patients with hematological malignancies, including AML, acute lymphoblastic leukemia, chronic myeloid leukemia, myelodysplastic syndrome, myeloproliferative diseases, and chronic lymphocytic leukemia (18). Among them, only 20% of patients with AML presented with hyperuricemia at diagnosis (S-UA level >7.0 mg/dl), a rate that was quite comparable with our result here. Several complications may cause hyperuricemia in the clinical course, which include tumor lysis syndrome, adverse reactions to medications, and renal dysfunction. Figure 1F clearly indicates the correlation between the S-UA and serum creatinine, suggesting that the increased S-UA was partly due to renal dysfunction. Nevertheless, serum creatinine concentrations did not affect the therapeutic efficacy (Figures 3B-D), suggesting that the S-UA level affected the clinical outcomes of patients with AML regardless of renal function.
In conclusion, a high S-UA level was associated with a poor prognosis in AML. The determination of the S-UA level is versatile and cost-effective and therefore widely applicable to the clinic, which may enable the individualization of treatment for patients with AML.
Footnotes
-
Disclosure Statement
The Authors have no conflicts of interest regarding the present work.
- Received June 18, 2013.
- Revision received June 29, 2013.
- Accepted July 3, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Cytokine response of acute myeloid leukemia cells has impact on patient prognosis: Insights from mathematical modeling
- Acute Myeloid Leukemia, Version 3.2017, NCCN Clinical Practice Guidelines in Oncology
- Febuxostat for Management of Tumor Lysis Syndrome Including its Effects on Levels of Purine Metabolites in Patients with Hematological Malignancies - A Single Institution's, Pharmacokinetic and Pilot Prospective Study