


Abstract
Background: Since its first description by Marx in 2003, the etiology of bisphosphonate-related osteonecrosis of the jaw (BRONJ) is the subject of numerous scientific discussions for oral and maxillofacial surgeons. Many retrospective studies on its etiology and pathogenesis have been carried out to explain pathological mechanisms; most of them just take a close look at the issue of dosage and application. Recently, attempts have been made, to identify co-factors which might promote the development of BRONJ. Patients and Methods: The present study is based on data of 169 patients with osseous metastatic malignancies. All patients received intravenous bisphosphonate therapy. On the basis of medical history, malignancy, and primary treatment, the modality of bisphosphonate therapy, and existing comorbidities and medication were analyzed. The role of immunosuppressive drugs, influence of underlying diseases, and general factors such as age and gender were examined. The predictability of necrotic involvement, influenced by the underlying malignancy and its specific therapy, e.g. radiation and cytostatic therapy were analyzed and statistically evaluated. Results: A total of 8.9% (n=15) of patients developed BRONJ. The average time between diagnosis of malignancy and BRONJ was 80 months. Nine patients suffered from breast cancer, five had prostate cancer and one renal cancer. Separation into stage and histological subtype did not show any significant correlation, nor did age or gender, to the occurrence of BRONJ. However statistical analysis did show a significant correlation concerning monocytostatic (p=0.0215) and triple-cytostatic therapy (p=0.0137). The majority of patients with BRONJ (60%) received a bisphosphonate therapy including zoledronate. Single application with one bisphosphonate was administered in 28 cases; 44 patients had a medical history of different use of bisphosphonate. Concomitant medication did not suggest possible correlation, nor did accompanying diseases, arterial hypertension (33.33%) or arterial microcirculatory disturbances (20%). Conclusion: The evaluation of our results is pioneering. The influence of cytostatics and combined therapy of cytotoxic drugs on the pathogenesis of BRONJ is demonstrated here statistically. We confirmed a drug- and dose-dependent occurrence of BRONJ. Further prospective studies should be performed to elucidate the role of tissue perfusion and oxygen saturation, and the influence of immunosuppressive drugs in relation to the occurrence of BRONJ, as well as on wound healing of initial lesions.
Currently, non-neoplastic diseases, such as osteoporosis (1, 2), osteitis deformans (Paget's disease) (1, 3) and arthritis (4) are treated by bisphosphonates, as are neoplastic diseases, such as tumor-associated hypercalcemia (1, 4-6), multiple myeloma and skeletally metastatic carcinomas (1, 5, 7, 8), e.g. breast cancer. In 2003, more than 20 million oral applications of bisphosphonates and, in 2005 about 2.9 million intravenous applications of bisphosphonates were recorded (9). Most frequently used bisphosphonates are zoledronate, pamidronate and ibandronate. Zoledronate is considered to be the most effective antiresorptive bisphosphonate (5, 10) and is used in therapy of tumor-induced hypercalcemia since 2001, osteolytic processes since 2002 (9, 10) and postmenopausal osteoporosis since 2007 (11). Pamidronate was firstly permitted for treatment of tumor-induced hypercalcemia in 1991, later for osteolytic lesions in multiple myelomas in 1995, and osteolytic bone metastases of solid tumors (9) and Paget's disease in 1996 (12). Ibandronate was firstly permitted in 1996 for treatment of tumor-induced hypercalcemia, skeletal metastatic carcinomas and postmenopausal osteoporosis. A prophylactic and analgesic effect of bisphosphonates has been reported, thus increasing the quality of life (13). In patients with breast cancer, a strong osteoclast-induced resorption is detectable, which is why bisphosphonates can reduce osteolytic lesions (14). However, osseous metastases of prostate cancer mainly occur as osteoblastic lesions, which is why there was no positive effect after application of pamidronate in 643 patients (15).
Zoledronate was found to be the only bisphosphonate that exhibits an analgesic effect as well as a reduction of skeletal complications in patients with prostate cancer. Additionally, zoledronate interacts with malignant plasma cells of multiple myeloma by causing a disturbance of the interaction between connective tissue cells and plasma cells in the bone marrow (10). In addition zoledronate has an analgesic effect and prevents fractures in patients with non-small cell lung cancer (16).
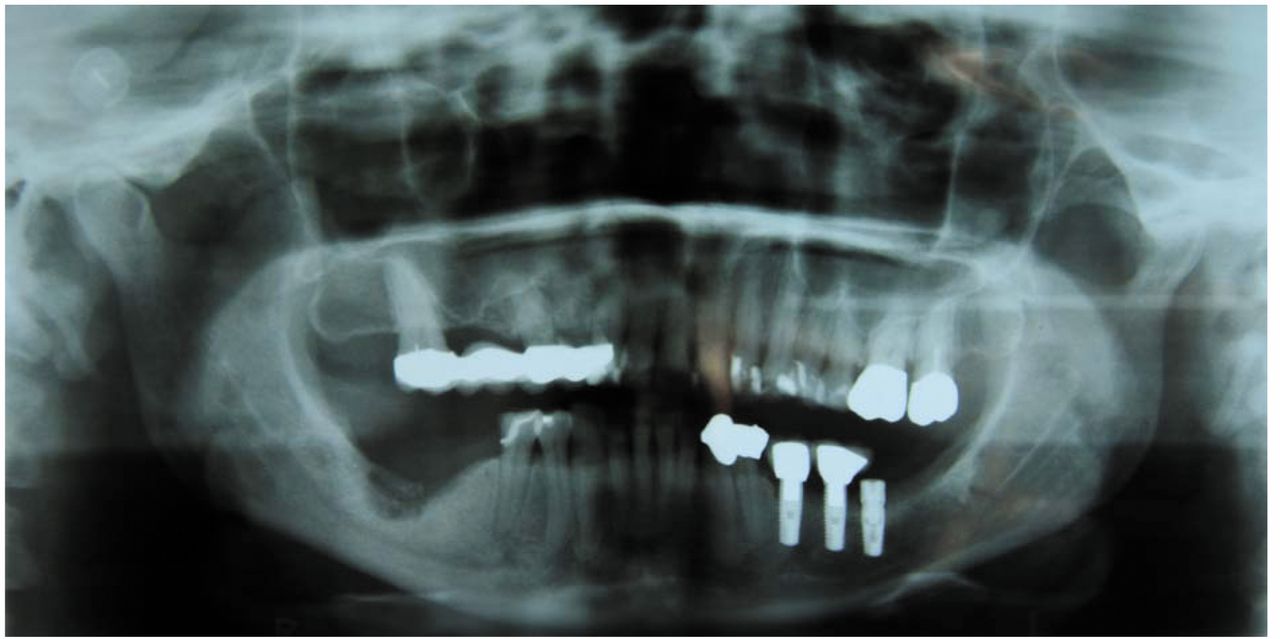
Typical features of patients suffering from BRONJ are exposed necrotic bone areas in the maxilla (Figure 1) or mandibula (Figure 2). Initial diagnostics include a panoramic view (Figure 3), cone beam computed tomography, computed tomography scans, magnetic resonance imaging and scintigraphy. Next to intraoral affections of exposed necrotic areas, extraoral fistulas, resulting from necrotic bone lesions can be found (Figure 4).
The clinical presentation and the course of BRONJ is similar to the one of osteoradionecrosis (ORN) (17-19). The risk of developing intraoral radiogenically-induced mucositis or osteitis of the jaw is mentioned only for the radiation field of head and neck tumors (5, 20). Radiation therapy in the head and neck area causes avascular osteonecrosis followed by high linear energy impacting on osteoblasts, osteoclasts, osteoprogenitor cells, and endothelial cells (21, 22). Radiation therapy hypoxia causes hypovascularity and hypocellularity, which result in the clinical image of a non-healing wound (17).
BRONJ is related to the presence of a high number of osteoclasts with active re-absorbed bone. This accumulation seems to simulate a healing process. A similarly high number of osteoclasts are also seen in ORN but in this case, accumulation is defined by sequestration and resolution (17). Both for ORN and BRONJ, obliteration of blood vessels of the jaw has been demonstrated; however, in patients with BRONJ this occurred only in very few samples (20).
The etiology of BRONJ is considered to be multifactorial. Several prospective and retrospective studies have reported the frequency of occurrence of BRONJ to be 6.7-28% (1, 24-26). Zoledronate and pamidronate use represent the highest risk factors for the occurrence of BRONJ (12). The length of duration of therapy seems to be decisive for the development of BRONJ; the average period ranges from 25 to 40 months after intravenous application (1, 5, 24, 26). Co-factors for the development of BRONJ are traumata of the oral mucosa, e.g. prosthesis pressure marks, and iatrogenic lesions after dental treatment or extraction wounds (12). Furthermore, there seems to be a relation between BRONJ and high expression of nuclear factor K-B ligands (RANKL) in human gingival fibroblasts (HGF) and human periodontal ligament cells (HPDL), which can be found in the periodontal tissue (27-29). However, spontaneous cases of BRONJ have been described (1), according to Katz, particularly in the posterior lingual mandible (30). Marx reported BRONJ to occur spontaneously in 22.3% of cases, and Ruggiero et al. in 14% of cases (31, 32). As a pathophysiological mechanism of

Exposed necrotic bone in the right maxilla in a patient who received zoledronate therapy over a period of 23 months. Exposed bone initiated by teeth removal.

Exposed necrotic bone in the mandible in a patient who was treated with zoledronate. Exposed bone occurred spontaneously.
BRONJ, a lack of repair stimuli of osteocytes and osteoclasts arises. This should lead to a summation of microfractures (33, 34). Other authors support the theory of the angiogenic effect of bisphosphonates (30, 35-38), e.g. lower capillary formation, inhibition of endothelial growth factor and of endothelial cell function (39). The findings of Allegra et al. support the theory of suppressive angiogenic activity by bisphosphonates on circulating endothelial cells in patients with BRONJ (36). In addition, in vitro studies showed an inhibition of vascular endothelial growth factor after zoledronate and pamidronate therapy, thus inducing a reduction of vascular sprouting (40, 41). Nevertheless, there is no clinical study to prove that the bisphosphonate-related inhibition of angiogenic activity causes osteonecrosis of the jaw (40, 42), which is why this theory is still controversially discussed (43, 44). Migliorati suspected that genetic disposition could be a co-factor for the development of BRONJ, as some patients were affected and others not (45).

Preoperative orthopantomographic image showing a typical osteolytic lesion in the right mandibule after bisphosphonate therapy with zoledronate.
The aim of this study was to investigate retrospective the incidence of BRONJ in patients treated for osseous lesions induced by cancer or metastases, taking into account further underlying diseases and concomitant therapies, which can lead to wound-healing disorders and associated hypoperfusion of maxillofacial tissues.
Patients and Methods
The evaluation of clinical data of this retrospective cohort study was carried out through the investigation and data analysis of patients who underwent adjuvant therapy with aminobisphosphonates due to a primary osseous metastatic malignancy. This data collection took place over a period between February 2006 and April 2008.
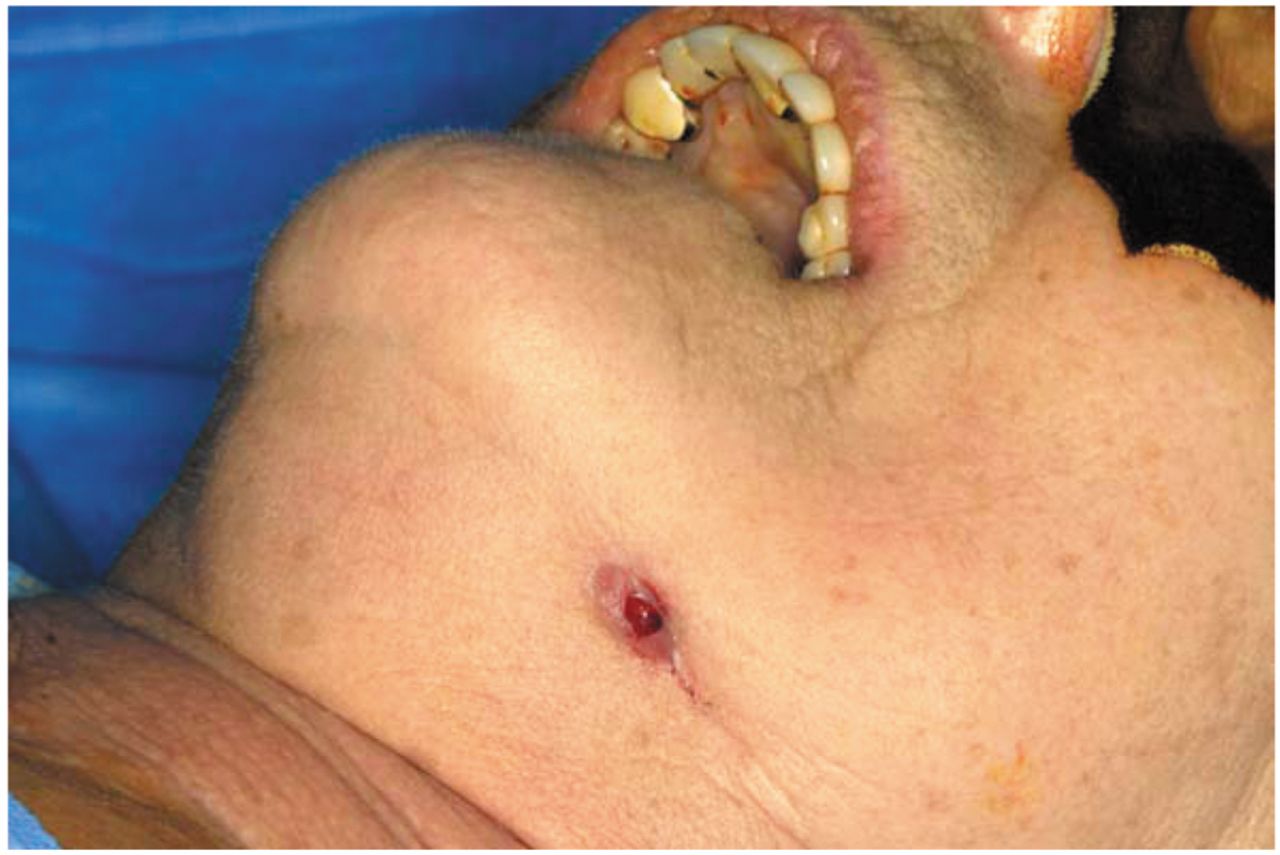
Extraoral fistula resulting from a necrotic bone lesion of the left mandible in a patient who received pamidronate (Aredia) therapy over a period of 19 months.
Patients' data were collected at the Department of Oral and Maxillofacial Surgery at the University Hospital of Aachen. Data collection included retrospective evaluation of the patients' medical history and dental examination during outpatient cytostatic therapy or intravenous bisphosphonate therapy. Inclusion criteria for this study were intravenous administration of a bisphosphonate due to a primary or secondary bone malignancy.
Evaluation of the patient data took place regarding previous bisphosphonate therapies (preparation, application time and dosage), the malignancy of primary diagnosis; present tumor stage according to classification of the Union Internationale de Cancer (UICC); histopathological results; the aubsequent cytostatic therapy, including the initial cytostatic subclassifications and special treatment regimens; and any further resulting mono- or polycytostatic therapy, as well as local or distant radiation therapy; concomitant medications according to their mechanism of action, and the prevailing comorbidities. Due to the large number of different application schemes of cytostatic substance classes, the statistical analysis was limited to the calculation enclosing mono- and polycytostatics, as well as their combinations. Radiation therapy was categorized in head-local and head-distant treatment, with appropriate classification of applied radiation dose and frequency of radiation.
Statistical analysis was performed in collaboration with the Institute of Medical Statistics at the University Aachen (RWTH) using Fisher's exact test and Wilcoxon test. For statistical analysis SAS 9.1 (SAS Institute Inc., Cary, USA) was used.
Results
The study cohort included 169 patients treated with bisphosphonates, 121 women (71.6%) and 48 men (28.4%). The prevalence of BRONJ in this study group was 8.9% (n=15 patients), consisting of 9 female (60%) and 6 male patients (40%); 154 patients did not show any signs of BRONJ (91.1%), in total, 112 females (72.73%) and 42 males (27.27%). The mean age at the BRONJ-group was 62 years (51 to 76 years), and that in the group without BRONJ 65 years (37 to 81 years). According to Fisher's exact test, there is no statistically significant relationship between sex (p=0.3682), or age of patients (p=0.3974) and the occurrence of BRONJ.
The median time for the development of BRONJ was 80 months; the earliest diagnosis of BRONJ was 11 months and the latest 157 months after the initial diagnosis of malignancy. The median ranged from 61.25 to 140.75 months after the initial diagnosis of malignancy. The study cohort of 169 patients consisted of 95 female patients with breast cancer (56.2%), 42 patients with multiple myeloma (24.3%), nine males with prostate cancer (5.3%), four patients with rectal cancer (2.4%), four with renal cancer (2.4%), three with lung cancer (1.8%), and 13 with miscellaneous malignancies, e.g. thyroid cancer or sarcomas (7.6%). Among the 15 patients with BRONJ, the most common malignancy was breast cancer (n=9; 60%), followed by multiple myeloma (n=5; 33.33%) and renal cancer (n=1; 6.67%). All patients related to this study were suffering from malignancies with bone metastasis. Twenty patients (13%) out of the initial study group and none of the 15 patients with BRONJ developed secondary malignancies. There is no statistical relationship between the incidence of a secondary malignancy and BRONJ (p=0.2209).
The bisphosphonates applied in this study cohort were pamidronate in 49 patients (29%), ibandronate in 49 (29%), zoledronate in 49 (29%), combined therapy including zoledronate and ibandronate in 19 (11.2%), and combined therapy of pamidronate and ibandronate in three patients (1.8%). Patients suffering from BRONJ were most often treated with zoledronate or combined zoledronate therapies (n=10; 66.67%), ibandronate (n=3; 20%) or pamidronate (n=2; 13.33%). In all 147 patients (87%) treated by monotherapy (p=0.7795), and all 22 patients (13%) treated by combined therapy, no statistical significance regarding the occurrence of BRONJ was found (p=0.5352).
In patients without BRONJ, the median number of administrations was 13, in those with BRONJ, the median was 28. In patients without BRONJ, the interquartile range (IQR) was five to 28 administrations (minimum one, maximum 99). In the group of patients with BRONJ, the frequency of administrations was higher, with IQR of 9.5 to 45.5 (minimum 2, maximum 70), without statistical significance (p=0.8353).
In the group without BRONJ treated with alternating bisphosphonates, the IQR of single applications was 21.5 and 52.25 (median=34.5), and for patients with BRONJ it was 26 to 67.25 applications (median=44). The minimum number of administrations was two in patients without BRONJ, and 17 in those with BRONJ, with maximums of 88 and 92, respectively. There was no statistical significance correlated to the sum of single applications with bisphosphonate-changing therapy and the occurrence of BRONJ (p=0.2685).
Fifty-nine patients without BRONJ received corticosteroids as concomitant therapy. Cortisone was applied in 14 patients (9.1%), prednisone in 12 (7.8%), and dexamethasone in 33 (21.4%). Four patients with BRONJ received dexamethasone (26.7%), one cortisone (6.7%), and one prednisone (6.7%). There was no statistical significance between very short impact of corticosteroid therapy and the occurrence of BRONJ (p=0.1214), nor after short impact (p=1), or long impact (p=0.2410). Furthermore, there was no statistical significance between other concomitant medications such as beta blockers or calcium channel blockers, and the occurrence of BRONJ (p=0.1701).
The prevalence of concomitant diseases, such as arterial hypertension, diabetes mellitus, lung diseases or adiposity was high (n=129), but did not show any statistical significance for the occurrence of BRONJ (p=0.05).
Another group of 123 patients received concomitant radiotherapy, 108 patients were without BRONJ (71%), and all 15 patients (100%) who suffered from BRONJ. Twenty-five patients received head-near radiotherapy (20.3%) (p=0.2936), and 98 patients head-distant radiotherapy (79.7%) (p=0.5776), without any statistical correlation to the occurrence of BRONJ for either group. Both groups that received head-distant radiotherapy were treated with a median dose of 40 Gy. No statistical significance was detected in the group without BRONJ (IQR 19-72 Gy) (p=0.3498), nor in the group with BRONJ (IQR 30-50.4 Gy) (p=0.5436).
A total of 56 patients without BRONJ (36.4%) and nine patients with BRONJ (60%) received cytostatic monotherapy with a frequency of five administrations. Statistical evaluation points to a significant correlation between the number of monocytostatic applications (p=0.0215) and the occurrence of BRONJ. Polycytostatic applications including two different cytostatics were given to 73 patients without BRONJ (47.4%) and in none of the patients with BRONJ, with a frequency of one to three applications, and was not statistically significantly correlated to the occurrence of BRONJ (p=0.4771). Application of three cytostatics, with a frequency of one or two administrations, took place for 25 patients (16.2%) without BRONJ and six patients (40%) with BRONJ. Similar to the statistical results for monocytostatic use, a significant correlation with the occurrence of BRONJ was found (p=0.0137).
Finally, the relationship between tumor stage, histopathological classifications of each malignant disease and occurrence of BRONJ was evaluated. As an example, patients with breast cancer (n=95) were divided into four subgroups: 47 patients without BRONJ (49.5%) and five patients with BRONJ (5.3%) had an invasive ductal carcinoma. Invasive lobular carcinoma was found in 10 women (10.5%) without BRONJ, but in no women with BRONJ. Likewise a mixed form of breast cancer was found in only one woman (1.05%) without BRONJ. The final group had tunor of an uncertain histology: 28 women (29.5%) without BRONJ and four women (4.2%) with BRONJ. No statistical correlation was found between the different histological types of breast cancer and the occurrence of BRONJ (p=0.9112) in any of the groups. Even the staging (UICC) of all patients with breast cancer (with and without BRONJ) did not show any statistically significant correlation (p=0.2037). In all other groups with malignancies, e.g. prostate cancer (p=0.4429), multiple myeloma (p=0.4782), and lung cancer (p=0.4429), no statistical significance concerning the occurrence of BRONJ was found.
Discussion
The aim of this retrospective cohort study was to determine possible correlations between patient-related examination parameters and the occurrence of BRONJ. Most publications concerning BRONJ are retrospective studies or case reports. Only few prospective studies are reported related to possible pathogenesis of BRONJ by means of selected generic parameters, e.g. different application forms of bisphosphonates, underlying malignancies, cytostatics, and age and sex of patients (1, 24). Several concomitant diseases and medications have been discussed as influencing factors for the occurrence of BRONJ, however, without proven statistical connections (17, 42, 46). In addition, tumor-specific therapies have been described, such as cytostatic or radiation therapy of the head and neck region with undesirable immunosuppressive side-effects, associated with the occurrence of BRONJ (12, 46). There is no prospective study with a closed group of patients in regard to the prevalence of all possible relevant factors that may be related to the occurrence of BRONJ.
The small sample size of 169 cancer patients, with only 15 patients (8.9%) with BRONJ, provides only limited information. This prevalence confirms the results of Bamias et al. with prevalence of 6.7% of BRONJ in their study group (24). In contrast, Boonyapakorn et al. presented a four-fold higher prevalence of 28%, which may be due to the fact that 46% suffered from multiple myeloma with highly-dosed cytostatics and corticosteroids, and 82% of all patients with BRONJ received bisphosphonate therapy containing zoledronate (1).
In most study groups, the majority of patients with BRONJ have breast cancer or multiple myeloma (7, 18, 32). A possible correlation between the frequency distribution with BRONJ and patients with breast cancer may be seen in the high prevalence of this malignancy within the female population. In addition, patients with breast cancer receive immunosuppressive cytostatic therapies, which may be risk factors for the development of BRONJ. The incidence of multiple myelomas is lower, but primary manifestation of numerous neoplastic proliferations, introduced by plasma cells, requires early bisphosphonate therapy. Furthermore, there is a prothrombotic effect of malignant diseases, which is additionally treated by high-risk therapies, such as corticosteroids and high-dose cytostatics.
Over a period of 60 to 141 months, our patients were treated, according to their malignancy, by several tumor-specific therapies, e.g. cytostatic or radiation therapy combined with concomitant therapies, such as corticosteroids. In every therapeutic cycle, patients are repeatedly exposed to immunocompromising systemic and local factors (neutropenia, oral mucositis), which enhance the probability of BRONJ occurrence (17, 36).
Zoledronate is currently the most potent and effective of all bisphosphonates (5, 10). In our study, 46.6% of patients that received zoledronate as single medication developed BRONJ; 66.7% received zoledronate in combined therapy. This high percentage supports the conclusion of a correlation between the use of zoledronate and the occurrence of BRONJ. In the literature we found many results that are similar to ours, with 41.2-64% of patients with BRONJ being treated by single administration of zoledronate and 22.7-58.8% in combined therapy (1, 24, 25, 35). A significant correlation between the occurrence of BRONJ and the application of zoledronate was found. Similar to our findings (13.33%), only 14% of patients with BRONJ in the study of Boonyapakorn et al. received pamidronate (1). In contrast to the studies of Bamias et al. and Boonyapakorn et al., in which no patient that was treated with ibandronate developed BRONJ, in our study group, three patients receiving ibandronate (20%) suffered from BRONJ (1, 24).
The question as to whether there is a significant influence concerning the means of treatment for the purposes of mono- or polycytostatic therapy and the occurrence of BRONJ cannot be answered on the basis of the available data. The fact that there were also patients who developed BRONJ following low-dose therapy supports the assumption of a multi-causal event.
Patients of our study group were treated monthly with intravenous application of bisphosphonates. The average duration of administrations in our study group was 36 months; this was close to that of other studies who describe 25-39 months (1, 5, 26).
Increased incidence of BRONJ at an advanced age is marked by the prevalence of treatment-indicated malignancies between the sixth and eighth decade of life (48); this becomes apparent in the results of multiple studies (1, 4, 24, 25).
As also presented in our study, most patients with BRONJ suffer from breast cancer (60%) at an average of 62-63 years (48). An existing relationship between the age of patients and malignant disease is strengthened by the results of Vahtsevanos et al., who presented a significant correlation in a study group of 1621 patients (49).
Sixty percent of patients who suffer from BRONJ are females. This reflects to the fact that 56.2% of all patients had breast cancer, which is similar to the results of O'Ryan et al., who reported 57.6% of female patients with BRONJ, with 44.1% patients with breast cancer (50). The results of Boonyapakorn et al. and Bamias et al. revealed a higher fraction of male patients with BRONJ (58.8-64%), whereas in their study groups, patients suffered from prostate cancer, and multiple myeloma, which is 1.5-times more frequently found in males (1, 24). The retrospective study results presented in the literature demonstrate that occurrence of BRONJ is not gender-specific, but depends on malignancies included in the study and their gender-specific prevalence.
As part of a multifactorial cause complex, concomitant medications are discussed; above all immunosuppressant corticosteroids (17, 40, 43, 47). The similar distribution in our two populations (26.6% with and 21.43% without BRONJ) show, similarly to the results of Boonyapakorn et al., that the duration of corticosteroid action is apparently not a predisposing factor for the development of BRONJ (1); even the statistical analysis did not show a significant correlation.
Numerous publications discuss the risk of increasing the occurrence of BRONJ by concomitant diseases, such as diabetes mellitus, peripheral vascular diseases (17, 43, 51), hypertension (52) and hypercholesterolemia (38). Local predisposing factors are seen in the context of orally manifesting complications, e.g. mucositis, gingivitis and periodontitis (17). In our study, hypertension was the complaint with the highest prevalence, both in patients with BRONJ (33.33%) and those without BRONJ (20.78%). Nevertheless, statistical evaluation did not prove a significant correlation for the occurrence of BRONJ.
Marx discussed a negative effect on local wound healing after radiation therapy (31). The clinical features of BRONJ seem to be similar to the ones of ORN, characterized by tissue hypoxia, hypovascularization, and hypocellularity (17, 21, 22). Both BRONJ and ORN appear predominantly after months to years; differently from the effect of bisphosphonates, radiation therapy impairs stem cells of late-reacting tissues, fibroblasts, and vessels (18, 20, 47). The current study did not show any correlation between direct or indirect head distant radiation therapy and the occurrence of BRONJ. The applied radiation dose, divided into low-, medium-, and high-dosage groups, did not confirm any significant correlation, similarly to the results of other studies (4, 5, 12, 21, 53).
Cytostatic therapy is discussed as a co-factor for the development of BRONJ (10). A possible etiology could be cytostatic-associated myelosuppression (17) and the resulting immunosuppression (36). Attributable to the cytotoxicity of cytostatics, local occurrence of oral mucositis is probable, thus allowing gateways for bacteria through epithelial lesions, supporting local infection and reducing immunotolerance. The dose of cytostatics and their combinations have an additive effect on the incidence of unsolicited effects (47). Statistical calculation showed a correlation of the occurrence of BRONJ and the frequency of monocytostatic therapy (p=0.0215). In patients treated by polycytostatic therapy with two substances, a significance was not found; however, in patients receiving three or more cytostatics, a statistical correlation was found (p=0.0137). Based on our results, we confirm the opinion that the risk of adverse reactions increases with accelerated individual application rates of cytostatics (47). Many authors grade cytostatic therapy as a possible correlating risk factor of BRONJ (5, 12, 31, 53). Similar to the studies of Ficarra et al. and Capalbo et al., most of our patients with BRONJ have been treated with alkylants (18, 54). Some cases, as also reported by Migliorati et al., were treated with cytostatics from the antibiotic group (5). Due to the small amount of data and a high variation in cytostatic regimens, a possible correlation cannot be considered. Larger prospective cohort studies are necessary to prove any correlation between the different cytostatic substances and the occurrence of BRONJ.
Conclusion
The available data set in this study group was not sufficient to address all our questions regarding finding significant correlations for the occurrence of BRONJ. Further questions remain concerning start and stop therapy with bisphosphonates, correlation in the occurrence of BRONJ, surgical treatment of patients with BRONJ at convenient time or most effective conservative and surgical treatment depending on the stage of BRONJ and associated diseases. Thus, further investigations and studies on bisphosphonates and BRONJ are necessary. In conclusion, the challenging management of this disease should make physicians and dentists reconsider the deliberate use of bisphosphonate therapy in BRONJ patients.
Acknowledgements
We would like to thank Mrs. Christina Fitzner (Dipl.-Stat.) from the Institute of Medical Statistics at the University Hospital of Aachen (RWTH).
Footnotes
-
↵Conflicts of Interest
The Authors confirm that they have no conflicts of interest with regard to this study.
- Received June 11, 2013.
- Revision received July 1, 2013.
- Accepted July 3, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Consolidation of Tumorous Mandibular Ramus Defect During Denosumab Treatment for Rapidly Progressive Metastatic Breast Cancer
- ACE Gene Variant Causing High Blood Pressure May Be Associated With Medication-related Jaw Osteonecrosis
- Unilateral Creeping Destruction of Deformed Mandibular Ramus and Angle Associated with Extensive Facial Plexiform Neurofibroma in Neurofibromatosis Type 1: A Case Report with Analysis of the Literature for Diagnosing Osteolytic Events of the Mandible in Tumor-suppressor Gene Syndrome