


Abstract
Background: Gallbladder carcinoma (GBC) is a cancer of the digestive tract with poor prognosis, for which surgical resection is the only potentially curative therapy. The prognostic value of postoperative peripheral blood leukocyte subset count in patients with cancer has not been fully investigated. Therefore, we retrospectively investigated the relation-ship between postoperative peripheral blood lymphocyte count and disease-free as well as overall survival after radical resection of GBC. Patients and Methods: The study subjects were 34 patients who underwent radical resection for GBC between January 2005 and April 2010. We retrospectively investigated the relation-ship between clinicopathological variables, including postoperative peripheral blood lymphocyte count, and disease-free as well as overall survival. Results: In univariate analysis, disease-free survival was worse in patients with intraoperative blood transfusion (p=0.0285), tumor node metastasis (TNM) stage ≥II (p<0.0001), and lymphocyte count of less than 1,000/μl (p=0.0002). Overall survival was worse in patients with TNM stage ≥II (p=0.0002) and lymphocyte count of less than 1,000/μl (p=0.0151). In multivariate analysis, TNM stage ≥II (p<0.0089) and peripheral blood lymphocyte count of less than 1,000/μl (p=0.0365) were independent predictors of poor disease-free survival. For overall survival, TNM stage ≥II (p=0.0230) was the only independent predictor. Moreover, lymphocyte counts of less than 1,000/μl correlated significantly with TNM stage ≥II, duration of operation, greater blood loss, and presence of intraoperative blood transfusion. Conclusion: Postoperative peripheral blood lymphocyte count correlates with outcome of patients with GBC treated by radical resection.
Gallbladder carcinoma (GBC) is a cancer of the digestive tract with poor prognosis and is the most common cancer of the biliary tract. The prognosis of GBC remains dismal even with recent advances in diagnostic modalities and surgical techniques (1-3). It is well-known that surgical resection is the only treatment which can achieve long-term survival in patients with GBC. The prognosis for patients with early GBC is associated with a 5-year survival rate ranging from 90% to 100% (4-6). On the other hand, advanced GBC is characterized by a very poor prognosis, with the 5-year survival rate below 30%. Therefore, assessment of prognostic predictors is important for the management of patients with GBC.
Recent studies reported that perioperative immunological and inflammatory response findings correlate with tumor recurrence and prognosis in various types of malignant tumors, including GBC. Decreased preoperative lymphocyte count, increased preoperative monocyte count, and elevated preoperative neutrophil-to-lymphocyte ratio (NLR) are related to poor prognosis in patients with cancer (9-12). Several investigators reported that perioperative changes in immune response are one of the predictors of therapeutic outcome after curative resection for digestive-tract cancer (13, 14). Lymphocytes play an important role in antitumor immune responses, through tumor recognition and immunological elimination of local and metastatic tumor cells (15-17). Therefore, we hypothesized that the postoperative peripheral blood lymphocyte count might be related to prognosis after radical resection for GBC. In this study, we retrospectively investigated the relation between postoperative peripheral blood lymphocyte count and disease-free, as well as overall, survival in patients with GBC after radical resection.
Patients and Methods
Between January 2004 and December 2010, 39 patients underwent radical resection for GBC at the Department of Surgery, Jikei University Hospital, Tokyo, Japan. Out of these, five patients were excluded: one patient due to insufficient data, and four patients who were lost to follow-up, leaving the remaining 34 (15 male and 19 female; mean age=67.0 years, range=38-88 years) patients for this study. All patients underwent macroscopically curative resection for GBC. Hemogram and chemistry profile were routinely measured for each patient preoperatively and on postoperative day (POD) 1. Absolute white blood cell (WBC) count, lymphocyte, monocyte, and each subset were routinely determined in peripheral venous samples.
First, we investigated the relation between clinicopathological variables and disease-free and overall survival after radical resection for GBC by univariate and multivariate analyses. These consisted of the following 10 factors: age, gender, duration of operation, intraoperative blood loss, presence or absence of intraoperative blood transfusion, presence or absence of gallstones, tumor stage based on tumor pathology, and postoperative neutrophil, lymphocyte, and monocyte counts on POD 1. Clinicopathological continuous variables were classified into two groups for the log-rank test and the Cox proportional hazard regression model as follows: age <60 or ≥60 years, duration of operation <300 or ≥300 min, and blood loss <1,000 or ≥1,000 g. Tumor staging was performed according to the pathological tumor node metastasis (pTNM) classification based on the guidelines of the TNM Classification of Malignant Tumors 6th edition in 2002 (18) and TNM stage was classified into two groups: stage ≤I or ≥II. The postoperative WBC subsets counts were classified as follows: neutrophil count <10,000 or ≥10,000/μl, lymphocyte count <1,000 or ≥1,000/μl, and monocyte count <300 or ≥300/μl, according to previous reports (19, 20).
Next, to assess the risk factor for decrement of postoperative peripheral blood lymphocyte count on POD 1, we analyzed the relation between patient characteristics and postoperative peripheral blood lymphocyte count, using the following nine factors: age, gender, duration of operation, intraoperative blood loss, intraoperative blood transfusion, presence of gallstones, TNM stage, and postoperative neutrophil and monocyte counts on POD 1.
Recurrence of GBC was defined as newly-detected abdominal or extra-abdominal tumors by computed tomography, magnetic resonance image, with or without an increase in serum carcinoembryonic antigen (CEA), or carbohydrate antigen 19-9 (CA19-9). For recurrence of GBC, chemotherapies or conversion to other chemotherapy were given based on performance status. For patients with poor performance status or refusal, best supportive care was given.
This retrospective study was approved by the Ethics Committee of the Jikei University School of Medicine (#21-121).
Statistical analysis. Data are expressed as the mean±standard deviation (SD). Univariate analysis was performed using non-paired Student's t-test and Chi-square test. Analysis of disease-free and overall survival was performed using the log-rank test. Factors that significantly influenced disease-free or overall survival were then used in the Cox proportional regression model for multivariate analysis. All p-values were considered statistically significant when the associated probability was less than 0.05.
Results
Patients' characteristics and clinicopathological variables. Patients' characteristics and clinicopathological variables are outlined in Table I. Among the study population, the mean age was 67.0, with a range from 38 to 88 years, and fifteen patients were male. Twenty-two out of 34 patients had TMN stage ≤I disease on tumor pathology. In this study, the five-year disease-free and overall survival rates after elective resection for gallbladder carcinoma were 45.4% (Figure 1A) and 74.3% (Figure 1B), respectively.
Patients' characteristics.
Comparison of clinical variables in relation to disease-free survival after radical resection for gallbladder carcinoma. Table II lists the relationship between the clinicopathological variables and disease-free survival after resection. In univariate analysis, disease-free survival was worse in patients with TNM stage ≥II (p<0.0001), intraoperative blood transfusion (p=0.0285), and postoperative lymphocyte count of less than 1,000/μl (p=0.0002). In multivariate analysis, TNM stage ≥II (p<0.0089) and postoperative lymphocyte count of less than 1,000/μl (p=0.0365) were independent and significant predictors of poorer disease-free survival.
Comparison of clinical variables in relation to overall survival after radical resection for gallbladder carcinoma. Table III lists the relationship between the clinicopathological variables and overall survival after resection. In univariate analysis, overall survival was worse in patients with TNM stage ≥II (p=0.0002) and lymphocyte count of less than 1,000/μl (p=0.0151). In multivariate analysis, TNM stage ≥II (p=0.0230) was the only independent and significant predictor of poor survival. Patients with a postoperative lymphocyte count of less than 1,000/μl tended to have worse overall survival than those with more than 1,000/μl postoperative lymphocyte count, which however did not achieve statistical significance (p=0.2995).
Univariate analysis of clinicopathological variables in relation to postoperative lymphocyte count after radical resection for gallbladder carcinoma. Table IV lists the relationship between clinicopathological variables and postoperative lymphocyte count. In univariate analysis, duration of operation (p=0.0025), intraoperative blood loss (p=0.0120), intraoperative blood transfusion (p=0.0139), and TNM stage ≥II (p=0.0011) negatively correlated with postoperative peripheral blood lymphocyte count.
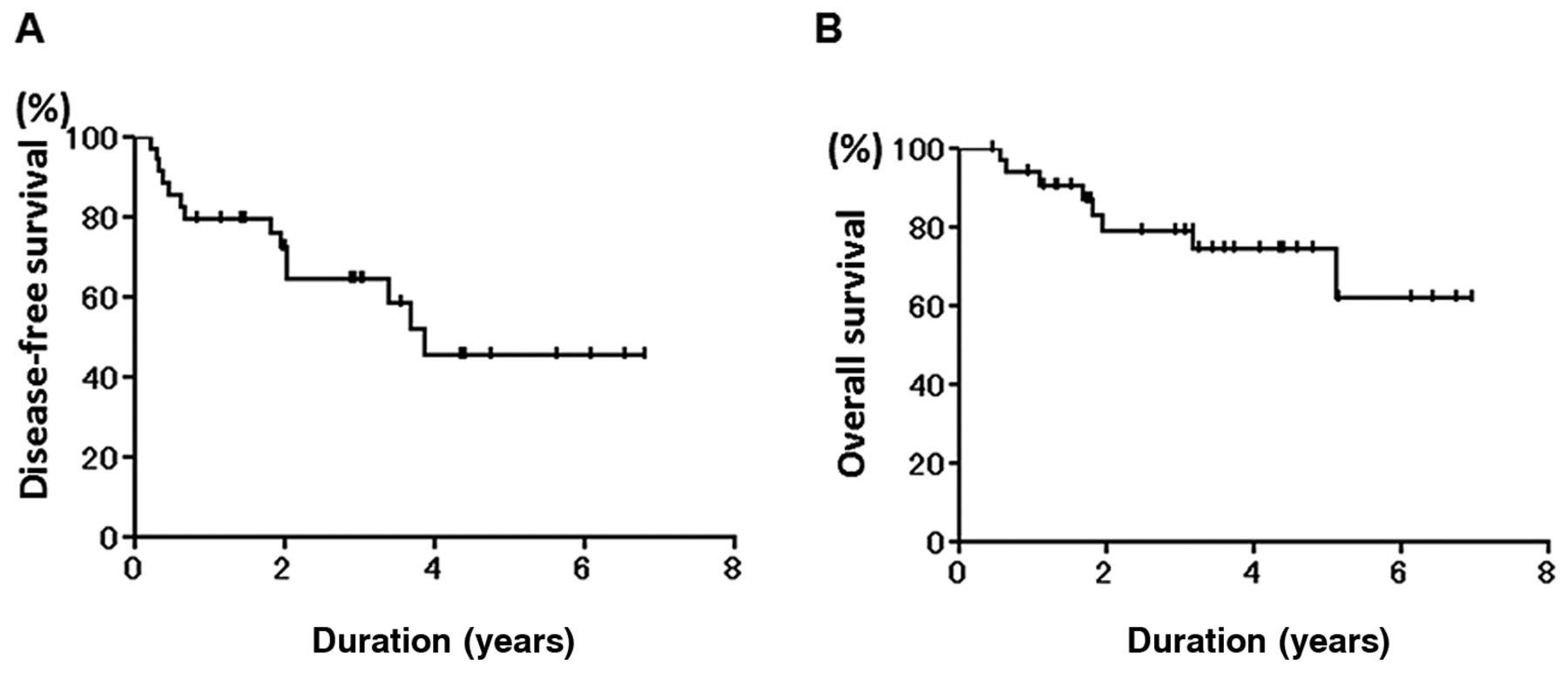
The five-year disease-free and overall survival rates for the patient group overall were 45.4% (A) and 74.3% (B), respectively.

Patients with a postoperative lymphocyte count of less than 1,000/μl had significantly worse disease-free (p=0.0002) (A) and overall (p=0.0151) (B) survival.
Discussion
Recently, reported prognostic factors for patients with GBC included early TNM stage, extent of surgical resection, microscopic curative resection, negative perineural invasion, well-differentiated tumor, adenocarcinoma, younger age, and female gender (21-24). Preoperative immunological factors have also been reported as predictors of prognosis in patients with GBC after cholecystectomy (12, 21). Ong et al. indicated that elevated preoperative NLR is a predictor of survival for curative resection in GBC (12).
Lymphocytes play an important role in antitumor immune responses and a persistent immunosuppressive state is associated with a high probability of recurrence and poor prognosis (15-17, 25, 26). A single malignant cell may have multiple tumor-specific antigens (27, 28). Cluster of differentiation-4 (CD4)+ and CD8+ T-cells have antitumor effect via recognizing these tumor-specific antigens. Activation of both types of T-cells requires the presentation of antigenic peptides on professional antigen-presenting cells (APCs). Dendritic cells (DCs) are the most potent APCs and play a central role in antitumor immunity by engulfing tumor antigens to facilitate the stimulation of antigen-specific T-cells (29-32). Actually, Nakakubo et al. indicated that a low presence CD4+ and CD8+ T-cells and DC infiltration in the tumor correlate with poor prognosis after surgery for GBC (33). Such infiltration and immune response could be considered to reflect a preoperative immunological and inflammatory status in patients with GBC.
In the present study, the postoperative peripheral lymphocyte count was shown to be a significant and an independent factor of disease-free survival and a significant prognostic factor of overall survival. Moreover, the postoperative lymphocyte count had a negative association with intraoperative blood loss and blood transfusion. Sugita et al. reported that the absolute count of the peripheral blood lymphocyte in the early postoperative period was significantly decreased in patients who underwent intraoperative blood transfusion as compared to that in those who did not (34). Dietz et al. have shown that depression of the lymphocyte count after surgery correlates with the duration of operation and the volume of intraoperative blood loss (35). Postoperative immunosuppression can be exacerbated by blood transfusion, which can induce a shift toward a Th2 phenotype associated with a fall in lymphocyte count and down-regulation of APCs (36). Reduction of intraoperative blood transfusion may maintain postoperative immune response and improve therapeutic outcome after radical resection for GBC.
Comparison of clinical variables in relation to disease-free survival after radical resection for gallbladder carcinoma.
Conclusion
The postoperative peripheral blood lymphocyte count positively correlates with tumor recurrence and survival in patients with GBC after resection. Measurement of the postoperative peripheral blood lymphocyte count may help risk stratification and decision making in the postoperative management of patients with GBC after resection.
Comparison of clinical variables in relation to overall survival after radical resection for gallbladder carcinoma.
Univariate analysis of clinicopathological variables in relation to postoperative lymphocyte count after radical resection for gallbladder carcinoma.
Acknowledgements
None declared.
- Received May 17, 2013.
- Revision received June 26, 2013.
- Accepted June 28, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}