


Abstract
Background: Fatigue is a serious problem for the majority of patients with cancer. In this context, several studies have shown benefits of physical activity during and following treatment. However, uncertainties remain regarding the optimal type and duration of physical activity. Therefore, this study examined the relationship between cancer-related fatigue and physical activity in the course of inpatient rehabilitation. Patients and Methods: Fatigue (Multidimensional Fatigue Inventory) and physical activity (Freiburg Questionnaire of Physical Activity) were assessed in a consecutive series of 35 patients with cancer attending oncological inpatient rehabilitation during a six-month study period. The three-week rehabilitation program included daily exercise therapy consisting of aerobic endurance training, moderate resistance training, coordination exercises, relaxation training and individual physiotherapy. Results: At discharge, a significant improvement in each dimension of cancer-related fatigue (p=0.001-0.003) and a significant increase of physical activity levels (p=0.001) were observed. A small, but significant negative correlation was found between cancer-related fatigue and the level of physical activity (R=−0.438, p=0.004). The largest effects were associated with a weekly energy expenditure of 3000 kcal through physical activity. Conclusion: The results support a non-linear dose-response relationship between cancer-related fatigue and physical activity. Since this is the first study providing specific exercise recommendations for an effective treatment of cancer-related fatigue in the context of inpatient rehabilitation, further research is required to validate the observed trends.
Cancer-related fatigue is a serious problem that affects the majority of patients with cancer in the course of their disease and may even persist for years after successful completion of treatment (1-3). In contrast to the rhythmically occurring tiredness in healthy people, which serves as a protective factor, cancer-related fatigue is associated with a significant loss of physical function and quality of life (3, 4). Therefore, the detection and treatment of cancer-related fatigue plays an important role in social and professional reintegration of such patients.
To date, the only intervention supported by a body of evidence and recommended for practice is exercise (5). In particular, aerobic endurance training and moderate resistance training showed predominantly positive effects on patients suffering from cancer-related fatigue by a significant improvement of physical performance and a reduction of fatigue compared to the respective control group (6-9). Consistent with these findings, the current clinical practice guidelines of the National Comprehensive Cancer Network (NCCN) recommend both endurance and resistance exercise as essential components in treatment interventions for cancer-related fatigue (10). While numerous studies have shown the positive effects of physical activity during primary cancer treatment, there is a lack of studies regarding the early period after acute treatment, such as inpatient rehabilitation (11). Furthermore, uncertainties remain regarding the optimal type and dose of physical activity (6, 7, 12-14). Based on the current state of knowledge, the cancer-specific dose-response relationship between physical activity and symptoms such as fatigue remains unclear and there is a lack of evidence-based exercise recommendations and specific guidelines for an effective treatment (12-15). It is also not known to what extent exercise prescriptions should vary depending on the type of cancer, cancer stage, treatment-related factors or the age of the patient (13, 15).
Therefore, the aim of this study was to investigate the relationship between cancer-related fatigue and the level of physical activity in the course of a multidisciplinary oncological inpatient rehabilitation program.
Patients and Methods
Patient selection. A consecutive series of patients attending oncological inpatient rehabilitation at the Zurich Alpine Clinic Davos in Switzerland were recruited for participation in the study between November 2010 and May 2011. Inclusion criteria were neoplastic disease, admission to inpatient oncological rehabilitation, age between 18 and 79 years, and the ability to understand German in speech and writing. Exclusion criteria were serious and acute cardiovascular and metabolic diseases which could be exacerbated by exercise or might lead to complications, general contraindications precluding participation in exercise testing or physical training (platelet count <10/nl, severe pain, dizziness, nausea or vomiting, hemoglobin <8 g/dl, infection and fever, cardio- or nephrotoxic chemotherapeutics), terminal disease with palliative care and communication problems due to cognitive impairments. A total of 32 patients did not fulfill these criteria or refused to participate. Another four patients dropped out of the study because they had to be transferred due to a deteriotation in health status, which was not related to the performed physical activity. Each of these patients later took part in the study when re-entering rehabilitation. Finally, a total of 35 eligible patients were enrolled in the study after providing informed consent in adherence to ethical guidelines (Table I). The majority of these patients entered rehabilitation after surgical resection of the tumor (85.7%), with a postoperative period of 24±16 days. All procedures of the study were conducted according to standard ethical guidelines of the Committee on Human Experimentation.
Rehabilitation program. The patients received a progressive and individualized multidisciplinary three-week rehabilitation program, which focused on increasing physical activity and psycho-physical reconditioning. The daily exercise therapy consisted of aerobic endurance training, moderate resistance training, coordination exercises, relaxation training and individual physiotherapy. The endurance training was conducted three to six times a week for up to 30 minutes using the treadmill, arm- or bicycle ergometer. Where possible the aerobic exercise was carried out by continuous training, or, if this was not tolerated for at least ten minutes, by interval exercise. The patients were monitored by evaluating heart rate, blood pressure, oxygen saturation and subjective exertion. The progressive resistance and coordination training was carried out two to three times a week for 45-60 minutes and consisted of a series of exercises for the major muscle groups using one's own body weight, thera bands, light weights, and balance pads. Further individual and group exercise units were carried out depending on physical function and health status of the patients. Additionally, the patients could use their free time between therapy units to go for a walk or do other voluntary physical activities. Despite the individualisation due to the patients differences in health status and physical function, endurance, resistance and coordination training were of approximately similar proportion regarding the total amount of physical activity. A standardized six-minute walk test was carried out once a week to document the progress of the patients' physical function.
Assessments. Fatigue: The evaluation of cancer-related fatigue was carried out immediately after recruitment and additionally one day prior to discharge by a German version of the Multidimensional Fatigue Inventory (MFI-20) (16). This 20-item self-report questionnaire measures the severity of fatigue in five dimensions: general fatigue, physical fatigue, mental fatigue, reduced motivation and reduced activity. The psychometric properties of this instrument have been tested in several studies with different groups of patients with cancer showing good results regarding its validity (16-22). In addition, age- and sex-matched reference values are available for the general German population, which were used to describe prevalence rates in the present study (21). In this process, we defined cut-off points based on the 75th percentile for moderate forms of fatigue and the 90th percentile for severe forms of fatigue as shown by Kuhnt and colleagues (22).
Baseline sample characteristics (n=35).
Physical activity: Physical activity levels were assessed at baseline and then weekly until the final evaluation one day prior to discharge. For this purpose we used the Freiburg Questionnaire of Physical Activity (FQPA), a valid self-report instrument which covers the overall health-effective physical activity (consisting of everyday, leisure and sporting activity) throughout the previous week and allows a differentiated estimation of energy expenditure (23). In order to minimize recall bias, which occurs especially in elderly people, we combined the questionnaire with a physical activity diary for the purpose of helping the patients record their performed physical activities during the week (24). The weekly energy expenditure is commonly used to describe dose response relationships in terms of health-related effects of physical activity (25-27). Therefore it represents the overall amount of physical activity in the present study. It was derived by multiplying the measured quantitative parameters (frequency, duration and intensity) of physical activity with the patient's body weight as described by Kriska and Caspersen (25). The average intensity of a specific physical activity was expressed by its metabolic equivalent or MET score, which was taken from the current Compendium of Physical Activities (26).
MFI-20 scores for cancer-related fatigue in the course of rehabilitation (n=35).
Statistical analysis. Data on sample characteristics are reported using descriptive statistics to show frequencies, mean values and distribution. As a precondition for the selection of further test procedures, the interval-scaled data were analyzed for normal distribution by the Kolmogorov-Smirnov test. Baseline characteristics of the sample were compared with those of the patients who did not participate in the study using the Mann Whitney test or the test for independent samples as indicated by whether or not a normal distribution occurred. A chi-square test was used for the comparison of nominal variables.
To evaluate the improvement of fatigue levels, the paired Wilcoxon sign rank test was used for each dimension of the MFI-20, since no normal distribution occurred for these parameters. Differences between the measurement points of physical activity in the course of rehabilitation were analyzed using the Friedman test and the Wilcoxon sign rank test as indicated. Because of unequal sample sizes at the different measurement points, values for only 21 participants could be used for a comparison with week 2.
A correlation analysis of fatigue improvement and physical activity level was carried out using Spearman's rank correlation coefficient as indicated. The improvement of fatigue in the course of rehabilitation was determined by calculating the difference in fatigue scores between discharge and admission. A simple regression was then carried out to determine the best fitting model for the observed data to explain the relationship between the two parameters. The coefficient of determination R2 indicates the suitability of each model for the analyzed data as a percentage (28). To examine the influence of sociodemographic, disease-related, and treatment-specific factors on the improvement of cancer-related fatigue in the course of inpatient rehabilitation, a single factor analysis of variance (ANOVA) was performed. Statistical tests were two-tailed and a value of 0.05 was considered to be statistically significant (28). The entire statistical analysis was performed using IBM SPSS Statistics (version 19, IBM, Ehningen, Germany).
Results
All 35 participants were able to complete their prescribed exercise therapy program including the questionnaires and there were no dropouts. During the study no adverse events or complications related to the performed physical activity were registered.
Cancer-related fatigue. The average prevalence of clinically significant cancer-related fatigue at admission to rehabilitation was 63.89%. Moderate forms of fatigue were represented at an average of 14.84%, while 49.14% of the patients were suffering from severe fatigue. Symptoms of fatigue were more pronounced in the dimensions of general fatigue, physical fatigue and reduced activity than in the dimensions reduced motivation and mental fatigue. In the course of rehabilitation, a significant reduction in the level of cancer-related fatigue was recorded in each dimension of the MFI-20 (Table II).
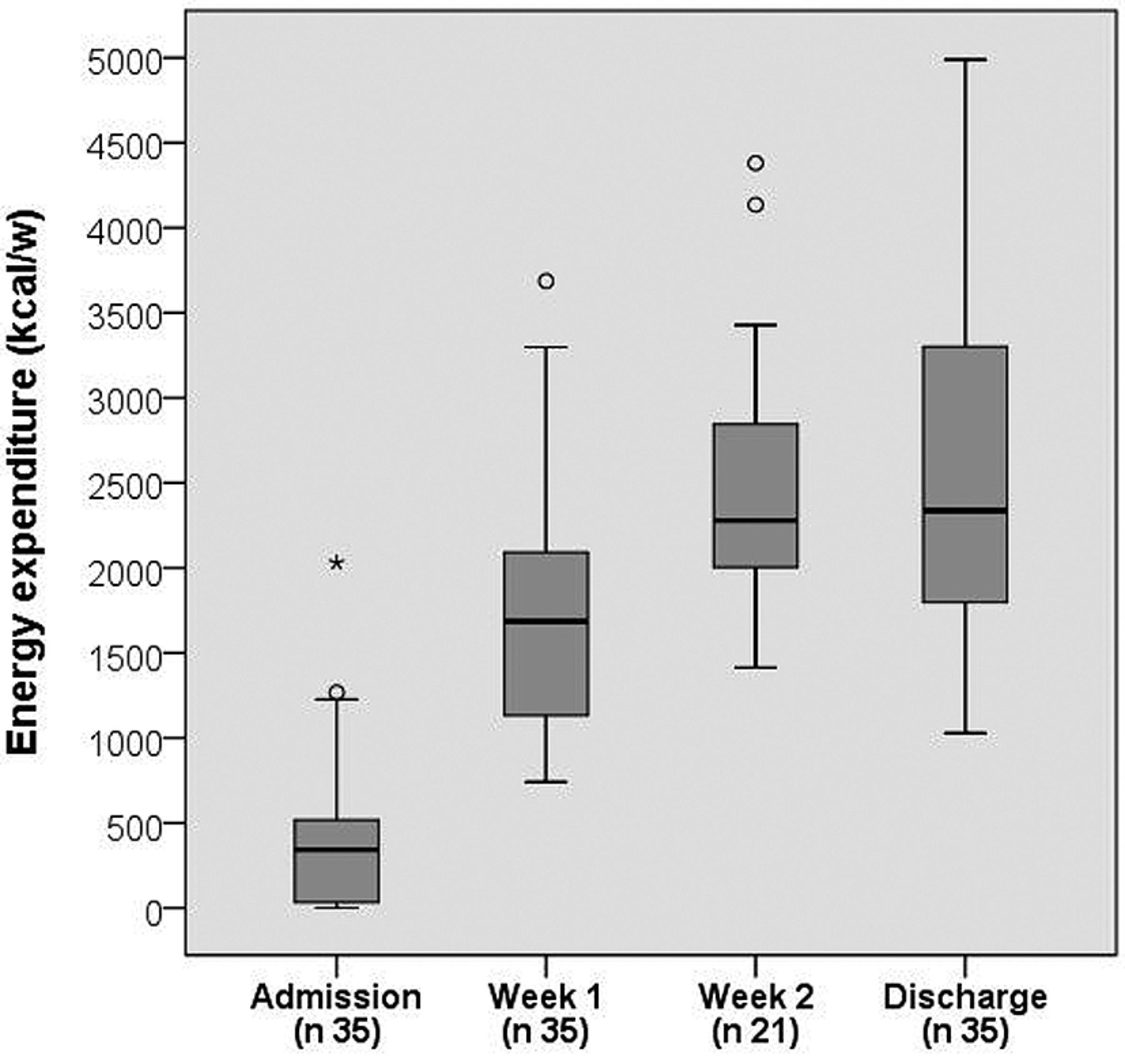
Physical activity. The physical activity levels of the patients showed a significant increase throughout the three-week rehabilitation program (Figure 1). There was a significant difference between the baseline evaluation, which refers to the week before admission, and the first week of rehabilitation. This trend was maintained until week 2 of rehabilitation. However, the increase between week 2 and the final evaluation at discharge was not statistically significant.
Correlation analysis. There was a weak, but significant negative correlation between physical activity level of the patients and the improvement in cancer-related fatigue in the course of rehabilitation (Table III). This also applies to the individual MFI-20 dimensions of general fatigue, physical fatigue and reduced activity. However, no correlation was found regarding the dimensions of mental fatigue and reduced motivation.
The relationship between the level of physical activity and the improvement of cancer-related fatigue in the course of inpatient rehabilitation is illustrated in Figure 2, by the total score of the MFI-20. Besides the underlying linear model of the correlation analysis, two additional non-linear explanatory models are presented. According to the best fitting cubic model, the greatest effects in terms of an improvement in fatigue symptoms were associated with a weekly energy expenditure of approximately 3,000 kcal (Figure 2). Positive effects can also be expected below this amount of physical activity. However, no substantial benefits in terms of a reduction of cancer-related fatigue would be expected above this level.
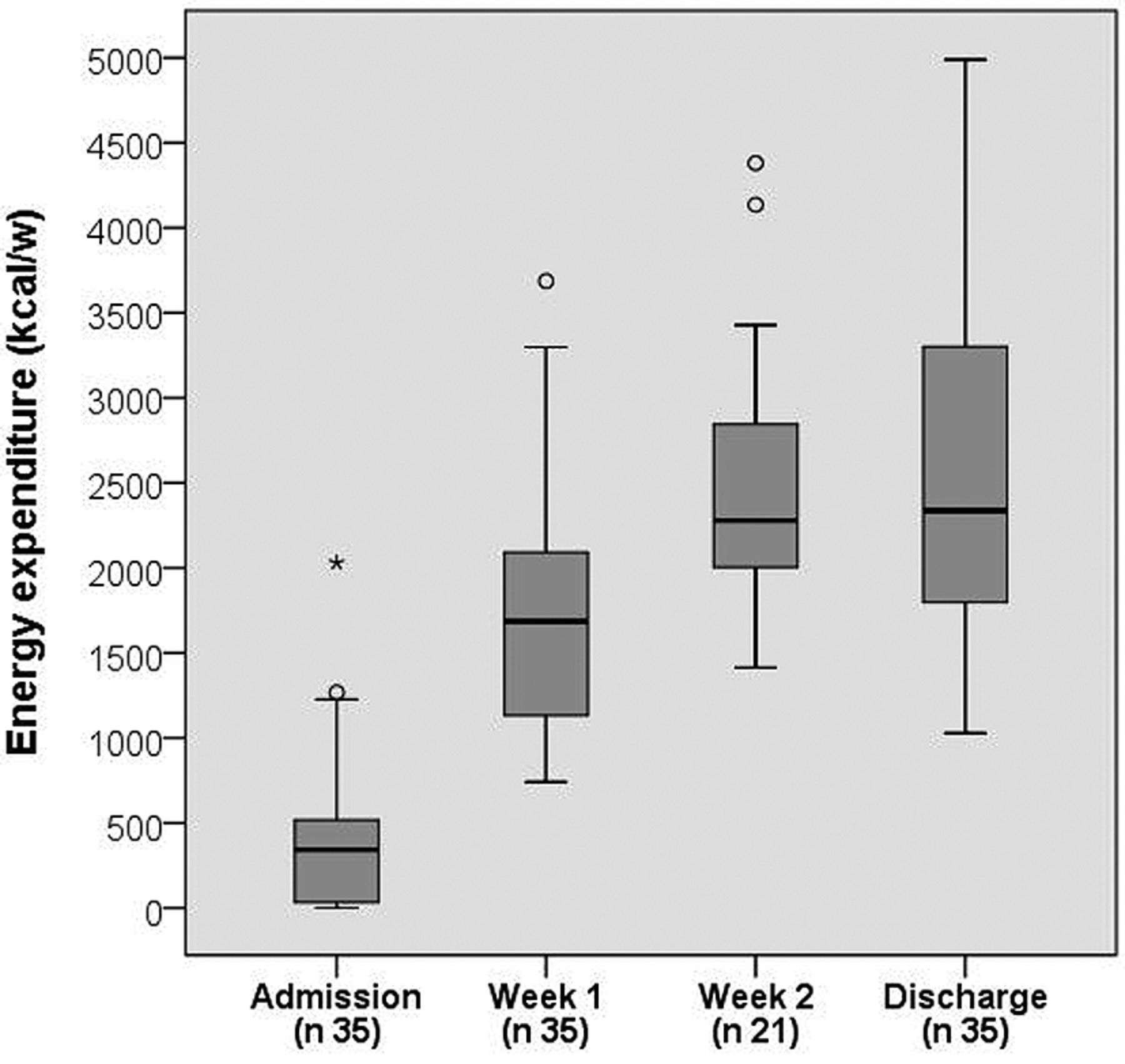
Development of energy expenditure in the course of rehabilitation (FQPA). Friedman test: p 0.001, Wilcoxon test: admission – week 1, p 0.001; week 1 – week, 2 p 0.001; week 2 – discharge, p 0.986. Boxplot diagram: Box, interquartile range with median; whisker, 1,5x interquartile range; point, outlier.
Finally, no significant influence of the analyzed sociodemographic, disease-related and treatment-specific factors were found regarding the improvement of cancer-related fatigue in the context of inpatient rehabilitation (Table IV).
Discussion
Levels of cancer-related fatigue and physical activity. Compared to a representative sample of the healthy German population, the patients of the present study still exhibited strongly increased fatigue levels after an average postoperative period of 24 days after admission to rehabilitation (21). While postoperative fatigue reaches preoperative levels after a month in studies with non-cancer patients, patients with cancer experience severe symptoms of fatigue for a prolonged time after surgery (29-33). This appears to be both associated with the disease itself as well as with already preoperatively increased fatigue levels (30, 33). Additionally, the detection of more pronounced symptoms in the MFI-20 dimensions general fatigue, physical fatigue and reduced activity are consistent with the results of a number of studies in patients with cancer during and after acute treatment (20, 22, 34-37).

Linear and non-linear relationship between energy expenditure and improvement of cancer-related fatigue in the course of inpatient rehabilitation (n 35). R2, linear 65.9%; R2, quadratic 66.6%; R2, cubical 67.6%; single-factor ANOVA for each model with p 0.001.
Correlations between physical activity (kcal/w) and the improvement of cancer-related fatigue (MFI-20) in the course of rehabilitation (n 35).
The mean fatigue values at discharge approached the reference values for the healthy German population (21). In comparison, preoperative levels of fatigue were not obtained until three to six months after surgery in studies with patients with lung and esophageal cancer (29, 31).
The significant increase of physical activity levels after week 1 and throughout rehabilitation (Figure 1) shows that exercise is possible and safe in the early period of cancer rehabilitation. In consistency, a roundtable of the American College of Sports Medicine (ACSM) on exercise guidelines for cancer survivors recommends resuming and maintaining daily activities and exercise as soon as possible after surgical and non-surgical treatment of tumors (15).
Influence of sociodemographic, disease-related and therapy-specific factors on the improvement of cancer-related fatigue (MFI-20) in the course of rehabilitation (n 35).
Relationship between physical activity and cancer-related fatigue. The nature of the relationship between physical activity and the reduction of cancer-related fatigue in the course of inpatient rehabilitation was examined by three different explanatory models (Figure 2). Since the values for R2 were all in the same range, the different models cannot clearly be delimited in terms of their suitability for the analyzed data. Therefore the results need to be interpreted with great caution, and only tendencies can be derived. However, the cubic model best represents the central statement of the study regarding the relationship of cancer-related fatigue and physical activity.
The results show that a weekly energy expenditure of 3,000 kcal has the greatest effect regarding the reduction of cancer-related fatigue in inpatient rehabilitation. A weekly physical activity level of 3,000 kcal can be achieved with 8 hours of moderate walking or 11 hours of moderate exercise per week (26). But even shorter periods of increased physical activity are an effective treatment intervention for cancer-related fatigue. If the optimum energy expenditure of 3,000 kcal per week cannot be achieved, for example due to health-related limitations of the patients, the results show that even smaller amounts of physical activity are preferable to inactivity, since positive effects were also observed below the mentioned value. When looking at Figure 2, it also seems that all patients with a physical activity level above 2,200 kcal could benefit from the rehabilitation program. However, a further increase of physical activity above 3,000 kcal per week is not likely to show beneficial effects on cancer-related fatigue and there is a possibility of a renewed worsening of fatigue symptoms, although this cannot be interpreted with certainty. A possible reason could be the simultaneous increase in adverse health risks associated with an increase in physical activity (38). Therefore, the positive health effects expected with a higher level of physical activity might be diminished by the potential health risks, which results in a lower net effect than with moderate levels of physical activity (39). Current research does not provide information on a maximum safe level of physical activity that can be tolerated without risk due to the associated increased health risks and ethical restrictions (40). However, these exercise recommendations for patients with cancer-related fatigue can be used by therapists for effective treatment of cancer-related fatigue in therapy practice, which provides a crucial increase in the quality of inpatient cancer rehabilitation.
In contrast to the findings discussed above, current literature predominantly supports a linear explanatory model with a proportional relationship between physical activity and health-related outcomes in terms of cancer (38, 41). However, these statements mainly refer to primary prevention. Hardly any studies examine the period after cancer diagnosis and acute therapy, and there are no comparative evidence-based data regarding a dose-response relationship for physical activity and cancer-related fatigue in inpatient rehabilitation. General, non-cancer specific information on optimum energy expenditure was provided by Paffenbarger and colleagues in an extensive study with 17,000 participants (42). Accordingly, the greatest positive health effects can be expected within a range of 2,000 to 3,500 kcal per week, which is consistent with the results of the present study, although a comparison is of rather limited significance due to the primary preventive approach of the authors.
The improvement in cancer-related fatigue is probably not a result of the physical exercise interventions alone. In the context of the multidisciplinary rehabilitation program further influencing factors such as an improved nutritional status or a good psycho-social support may result in a reduction of cancer-related fatigue. This should be examined in future studies using control groups and regression analysis. Also conceivable is an indirect mechanism of physical activity, as illustrated and presented by current research (7, 43). Thus, an increase of physical activity indirectly reduces cancer-related fatigue through an improvement of psychological, behavioral and social factors.
Regarding the MFI-20 dimensions of mental fatigue and reduced motivation, the improvement cannot be attributed to physical mechanisms associated with an increase of physical activity or an improvement in physical function, as also shown in another study of inpatients with lung cancer (44). The results suggest that interventions of the rehabilitation program other than physical activity are more likely to be effective. A study by Dimeo and colleagues showed equivalent improvements in cancer-related fatigue with progressive relaxation training compared to aerobic exercise, although it was not clear which dimension of cancer-related fatigue was improved (45). Based on the results of the present study, the mechanisms that lead to an improvement of mental and emotional aspects of fatigue remain unclear. Future studies should examine the influence of cognitive and psychological treatment interventions.
Influence of sociodemographic, disease-related, and treatment-specific factors. The results show that the reduction of cancer-related fatigue in the context of inpatient rehabilitation is independent of the analyzed factors age, gender, diagnosis, tumor stage and previous treatment (Table IV). Cancer-related fatigue equally affects all age groups and both sexes, as also shown in a number of other studies (20, 22, 35, 46-48). The majority of studies also support the theory of an independence of cancer-related fatigue regarding disease-related factors, cancer diagnosis and tumor stage, and the factor of previous treatment (20, 22, 35, 48, 49). These findings should, however, not be misinterpreted by the means of insignificance of the analyzed factors in the context of therapy, since they still need to be considered in the establishment of treatment interventions, and no standard therapy exists for all patients with cancer.
Study limitations. The validity of the present study is restricted by some limiting aspects, such as the small sample size. However, the minimum of 30 participants for the applicability of most statistical tests has been exceeded, for which reason a representative sample size could be achieved. By the exclusion of patients over 80 years, no statements can be made about this population. Since tumors mainly manifest at an advanced age, this should be considered in future studies in order to be able to provide evidence-based treatment decisions for this age group (50). Additionally, tumors of the digestive organs and respiratory system are by far the most represented in the sample (Table I). For this reason, the validity of the present results is limited to these types of cancer.
Due to legal requirements and ethical reasons, clinical trials in inpatient rehabilitation are bound by certain restrictions, resulting in limitations of internal validity (51). Thus, it was not possible in the present study to withhold treatment interventions from the patients in order to set up a control group.
The most practical and widely used method to measure physical activity in clinical practice is the assessment by questionnaire (52). However, due to its subjectivity, this method is often characterized by a general overestimation of physical activity levels in comparison to objective methods (52-54). Future studies should therefore validate the results of the present study regarding the optimum level and type of physical activity in inpatient oncological rehabilitation by using more objective methods.
Conclusion
The high prevalence and predominantly severe forms of cancer-related fatigue observed in the present study underline the necessity for appropriate assessment and treatment strategies for patients suffering from cancer-related fatigue in inpatient rehabilitation. In this context, the general efficiency of the multidisciplinary rehabilitation program of the present study is supported by the highly significant reduction of cancer-related fatigue in the course of rehabilitation.
In terms of the relationship between physical activity and the improvement of cancer-related fatigue in inpatient rehabilitation, the results of the present study support a non-linear dose-response relationship. The observed data and recommendations predominantly apply to patients post-therapy for cancer, with moderate to severe and long lasting forms of fatigue, and particularly with tumors of the digestive organs and respiratory system. To our knowledge, this is the first study providing specific exercise recommendations for an effective treatment of cancer-related fatigue. The results represent a first step to a better understanding of the effects of physical activity on cancer-related fatigue in the context of cancer rehabilitation. Based on the previously discussed study limitations, further research is needed to validate the observed trends with larger sample sizes and in relation to other cancer entities. For example, the data and recommendations are not necessarily applicable to patients with extensive metastatic disease or in palliative care.
Footnotes
-
Conflicts of Interest
The Authors have no conflicts of interest to declare.
- Received April 29, 2013.
- Revision received May 27, 2013.
- Accepted May 29, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.