


Abstract
Aim: To compare treatment results with use of nab-paclitaxel in routine clinical practice with data obtained from clinical trials. Patients and Methods: A retrospective chart review of all 36 patients with metastatic breast cancer treated with nab-paclitaxel was performed. Nab-paclitaxel was given weekly and usually started at 150 mg/m2. Results: Thirteen (36.1%) patients received nab-paclitaxel as first-line, seven (19.4%) as second-line and 16 as third- or further line treatment. Overall, the response rate was 9.7%, disease control rate 64.5%, median progression-free survival 7.5 months and median overall survival 14.2 months. The most frequent non-hematological toxicities of grade 3 or more were fatigue (27.8%), dyspnea, rash and arthalgia (all 5.6%). Six (16.7%) patients developed peripheral neuropathy of grade 2 or more. Incidence of neutropenia grade 3 or more was 41.7% with no case of febrile neutropenia. Conclusion: According to our experience, weekly nab-paclitaxel is effective and tolerable, with results at least comparable to those from the prospective clinical trials.
Taxanes are effective in the treatment of metastatic breast cancer (MBC) (1). Yet, solvents necessary due to the hydrophobicity of these agents cause crucial toxicities and impair the efficacy of conventional taxanes (2-5). Premedication with corticosteroids is mandatory but causes additional side-effects. In addition, docetaxel and paclitaxel are now broadly used in the (neo)adjuvant setting. Thus, the majority of patients will have been exposed to either of these two taxanes once they develop metastases.
Nab-paclitaxel is a unique formulation of paclitaxel attached to albumin-bound nanoparticles. The nanoparticle drug delivery system eliminates the need for toxic solvents such as cremophor. As one result, nab-paclitaxel does not mandate premedication in order to avoid hypersensitivity reactions. Importantly, nab-paclitaxel exhibits linear pharmacokinetics, allowing dose-dependent antitumor activity unlike solvent-based paclitaxel and docetaxel (6). Moreover, albumin binding facilitates the passage of the drug from the bloodstream via the endothelium of the blood vessels to the underlying tumor tissue by exploiting the physiological transport properties of albumin. The albumin-drug complex binds to the glycoprotein receptor (GP)-60 on endothelial cells, consecutively activating caveolin-1, resulting in transcytosis of intact nanoparticles across the cell membrane (7-10). Its binding to the glycoprotein secreted protein, acidic and rich in cysteine (SPARC) may contribute to peri- and intratumoral accumulation of paclitaxel (11). In clinical trials, treatment with nab-paclitaxel resulted in excellent clinical outcomes in patients with first-line and anthracycline-pretreated MBC, and in substantial efficacy in heavily pretreated, taxane-refractory MBC.
In the pivotal phase III trial, 460 patients with MBC (~40% first line, ~80% anthracycline-pretreated) were randomized to treatment with either nab-paclitaxel at 260 mg/m2 or solvent-based paclitaxel at 175 mg/m2 on day 1 every three weeks (12). Treatment with nab-paclitaxel resulted in a significantly higher overall response rate (ORR: 33% vs. 19%, p=0.001) and significantly longer median time-to-progression (TTP) (23.0 vs. 16.9 weeks; hazard ratio (HR)=0.75, p=0.006) as compared to treatment with solvent-based paclitaxel. There was a numerical difference in median overall survival (OS) (65.0 vs. 55.7 weeks) which did not reach statistical significance. In patients who received second- or further line therapy, the median TTP (20.9 vs. 16.1 weeks; HR=0.73, p=0.02) and median OS were significantly prolonged by nab-paclitaxel (56.4 vs. 46.7 weeks; HR=0.73, p=0.024) (12). Nab-paclitaxel led to a significantly lower rate of neutropenia. Grade 3 sensory neuropathy was higher for nab-paclitaxel as compared to conventional paclitaxel (10% vs. 2%) but could be managed with dose reductions and interruptions, and improved more rapidly as compared to neuropathy under conventional paclitaxel (median=22 vs. 79 days, respectively) (12).
Two controlled clinical trials evaluated nab-paclitaxel monotherapy of MBC in a weekly schedule. In a randomized phase II study, 302 first-line patients were randomized to four treatment arms: nab-paclitaxel at 300 mg/m2 on day 1 q3w; weekly at 100 mg/m2 or 150 mg/m2 on days 1, 8, 15 q4w, respectively; or docetaxel at 100 mg/m2 on day 1 q3w (13). Nab-paclitaxel at 100 and 150 mg/m2 weekly led to a higher ORR than docetaxel (45%, 49% vs. 35%, respectively), as assessed by independent radiologist review, without reaching statistical significance. The disease control rate (DCR) as assessed by independent review was significantly higher for both nab-paclitaxel at 100 (p=0.009) and 150 mg/m2 (p=0.017) versus docetaxel (75% and 80% vs. 58%, respectively). Treatment with nab-paclitaxel at 150 mg/m2 weekly resulted in a significantly longer median progression-free survival (PFS) as compared to docetaxel in the independent radiologist assessment (12.9 vs. 7.5 months; HR 0.495, p=0.0065) (13). In the final survival analysis, nab-paclitaxel at 150 mg/m2 weekly led to a median OS of 33.8 months as compared to 22.2 months for nab-paclitaxel at 100 mg/m2 weekly, 27.7 months for nab-paclitaxel at 300 mg/m2 every three weeks and 26.6 months for docetaxel at 100 mg/m2 every three weeks. Statistical significance was reached for the comparison of nab-paclitaxel at 150 mg/m2 versus nab-paclitaxel at 100 mg/m2 (p=0.008) (14). For docetaxel, a higher rate of grade 3 or 4 fatigue, neutropenia and febrile neutropenia was reported. The incidence of sensory neuropathy was similar across all arms. Time-to-improvement to grade 2 or less was shorter for all nab-paclitaxel arms, with a median of 20 days for the 150 mg/m2 -weekly as compared to a median of 41 days for docetaxel (13, 14).
Patients with a median of three (range of 0-14) prior chemotherapies for metastatic disease were treated in a phase II study with nab-paclitaxel at 100 mg/m2 (n=106) and in a second cohort at 125 mg/m2 (n=75) on days 1, 8 and 15 every four weeks. The ORR was 14% and 16%, DCR 26% and 37%, median PFS 3 and 3.5 months, and median OS 9.2 and 9.1 months, respectively. There was no survival difference between patients who achieved stable disease (SD) ≥16 weeks and those with a confirmed response. Overall, nab-paclitaxel was well-tolerated. Nine patients (8%) in the 100 mg/m2 cohort and 14 (19%) in the 125 mg/m2 cohort developed grade 3 sensory neuropathy. Patients who developed treatment-limiting peripheral neuropathy could be restarted on a reduced dose of nab-paclitaxel after a delay of one to-two weeks (15).
It is commonplace that controlled clinical trials provide the highest level of evidence. Yet it is also undisputed that clinical trials are prone to selection bias and do not always reflect clinical reality. Use of nab-paclitaxel in treatment of MBC is still not common in German clinical practice despite its recommendation in German treatment guidelines (16). In our Institution, nab-paclitaxel has been integrated into routine treatment of MBC. We wanted to determine how our treatment results compare with data generated in controlled clinical trials.
Patients' characteristics.
Patients and Methods
We performed a retrospective chart review of all patients with MBC who started treatment with nab-paclitaxel in our Institution from January 24th 2011 to September 25th 2012.
Nab-paclitaxel was given as monotherapy and was usually started at a dose of 150 mg/m2. Three heavily pre-treated patients were started at a lower dose: One patient had a starting dose of 120 mg/m2 and two other patients a starting dose of 100 mg/m2. In case of toxicities grade 3 or more, or neurotoxicity grade 2 or more, the dose was reduced by ~20%, corresponding mostly to 120 mg/m2 (level-1), 100 mg/m2 (level -2) and 80 mg/m2 (level -3). Patients received nab-paclitaxel as a weekly schedule for three out of four weeks.
According to our Center's guidelines, response was usually evaluated after every second cycle. Descriptive statistics were used to summarize patient and tumor characteristics. The ORR was defined as complete or partial response (CR+PR) according to the Response Evaluation Criteria in Solid Tumors (RECIST) criteria version 1.1 (17). DCR was defined as CR plus PR plus SD according to RECIST criteria. PFS was defined as the interval between the first dose of nab-paclitaxel and the time of disease progression or death. OS was defined as the interval between the first dose of nab-paclitaxel and death. PFS and OS were assessed using the Kaplan-Meier method censoring for patients with no documented event at the time of last follow-up. Analysis of OS was performed for all patients. Analysis of PFS was only performed for patients where tumor response had been evaluated.
Treatment with nab-paclitaxel.
Summary of efficacy data.
Results
Patients' characteristics. We identified 36 patients with MBC who started treatment with nab-paclitaxel between January 2011 and September 2012. Median follow-up was 194 (range 17-464) days. Patient and tumor characteristics are summarized in Table I and reflect a typical population of patients with MBC seen in our clinical practice. Their median age was 65 years. More than half of the patients had received prior (neo-)adjuvant cytotoxic therapy, roughly one-third had received taxanes as (neo-)adjuvant therapy. Overall, 83.3% had visceral metastases, 58.3% had bone metastases.
Treatment. Details of nab-paclitaxel treatment are outlined in Table II. Thirteen (36.1%) patients received nab-paclitaxel as first-line treatment. Most patients (91.7%) started with nab-paclitaxel at 150 mg/m2. The median number of cycles administered was 4 (range=1-11) and decreased with increasing treatment lines. The dose of nab-paclitaxel was delayed in 18 (50%) patients and reduced in 20 (55.6%) patients.
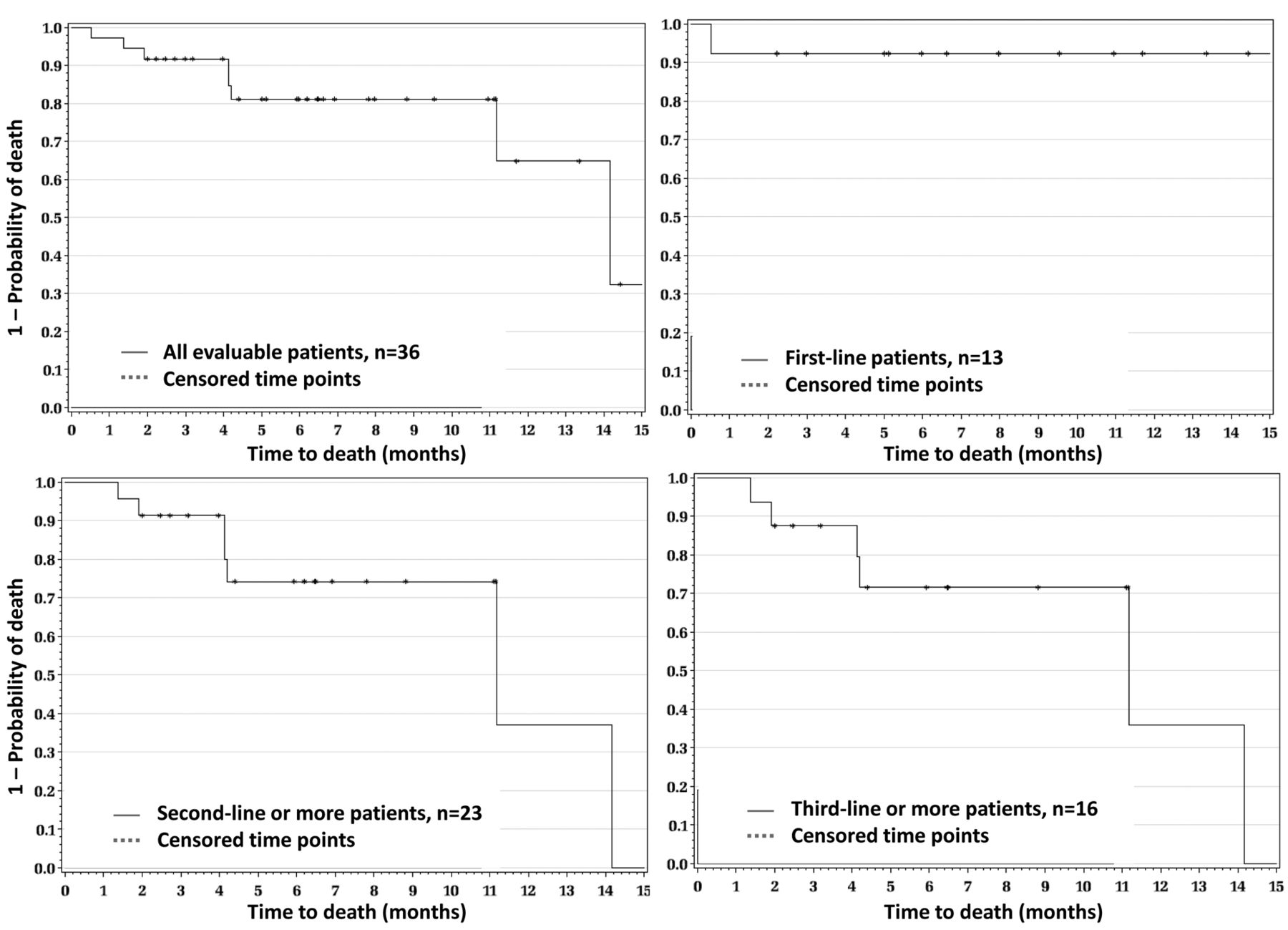
Efficacy. Efficacy data are summarized in Table III. No CR was observed. Overall response was observed in three (9.7%) patients. The DCR defined as CR, PR and SD, was 64.5%. With a median follow-up of 194 days, disease in 15 patients progressed and eight patients died. Overall, the median PFS was 7.5 months and the median OS 14.2 months. Figures 1 and 2 show the Kaplan-Meier plots for PFS and OS for the overall population according to treatment lines. Median PFS and median OS have not yet been reached in patients treated with nab-paclitaxel as first-line therapy.
Toxicity. A total of 451 doses of nab-paclitaxel were administered. Incidence of toxicities grade 3 or more is summarized in Table IV. There was no grade 5 toxicity. There was no grade 4 non-hematological toxicity. The most frequent non-hematological toxicities were fatigue, dyspnea, rash and arthalgia. There was one patient with grade 4 neutropenia; 14 (38.9%) patients had grade 3 neutropenia. No case of febrile neutropenia was documented. Patients did not receive primary prophylaxis.

Progression-free survival.
Overall, six (16.7%) patients developed peripheral neuropathy grade 2 or more. There was no grade 4 peripheral neuropathy. Only one (2.8%) patient developed grade 3 peripheral neuropathy which led to termination of treatment with nab-paclitaxel. This patient received nab-paclitaxel as fourth line therapy and had received docetaxel as adjuvant and vinorelbine as second-line therapy. Five patients had grade 2 peripheral neuropathy. Out of these, two received nab-paclitaxel as first-, one as second-, one as fourth-, and one as sixth-line therapy. In these five patients, toxicity was managed with dose reduction of nab-paclitaxel and was not the cause of treatment termination.
Adverse events.
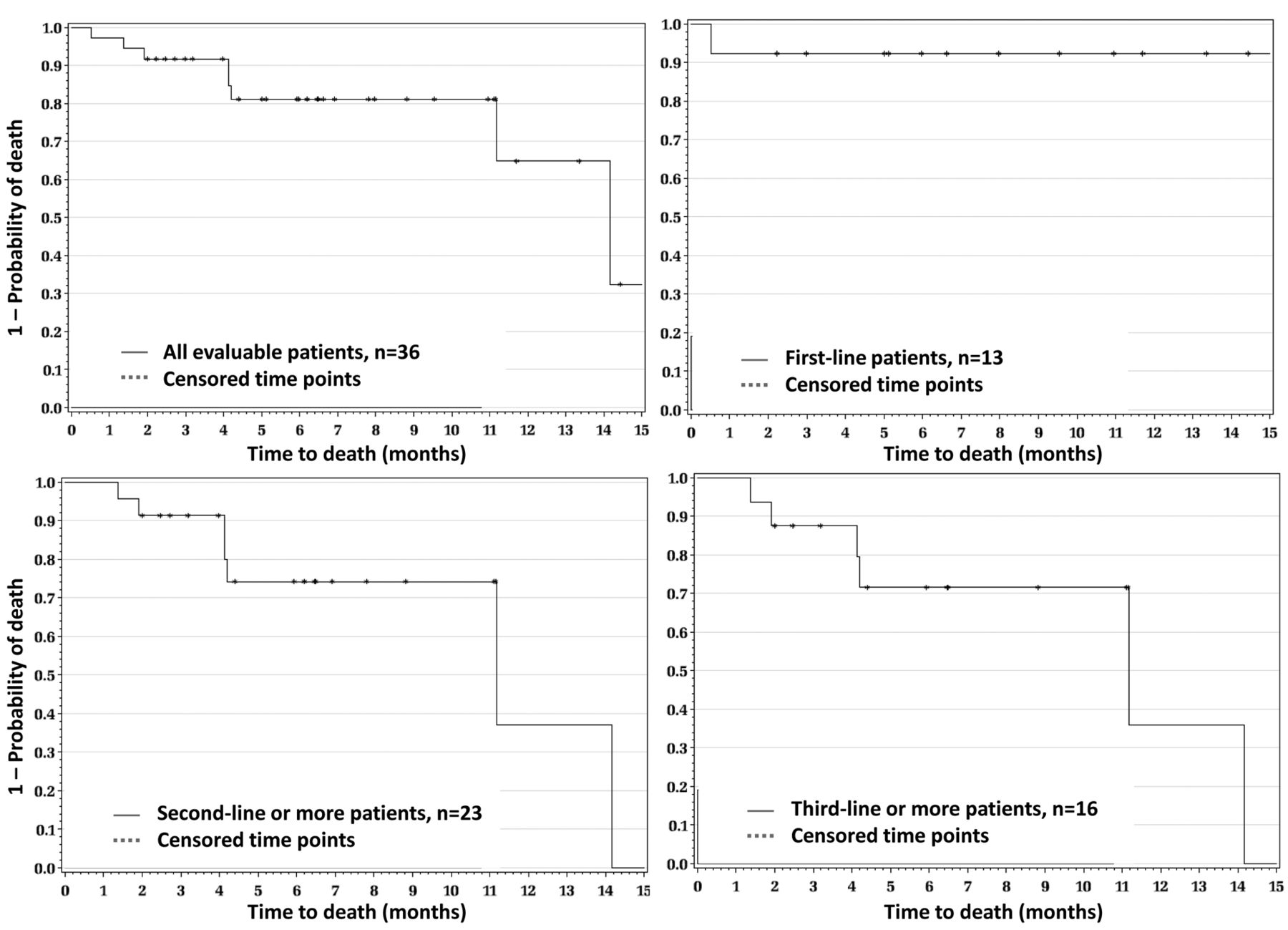
Overall survival.
Discussion
It is a challenge to compare results of controlled clinical trials with those from treatment in routine clinical practice. First of all, patient populations will almost certainly differ. Patients in our cohort were more than 10 years older, with a median age of 65 years as compared to a median age of 53 years (15) and 54 years (13) in the prospective trials evaluating nab-paclitaxel in MBC in a weekly schedule. A proportion of 17% of our patients had a performance status of 2 as compared to 6% (13) and 5% (15) in the prospective clinical trials. Most importantly, the clinical trials had measurable disease as a mandatory inclusion criterion (12, 13, 15). Of course this is different in a patient cohort from clinical routine. While for example, 6% of patients in the pivotal nab-paclitaxel trial had bone metastasis (12), this was the case for 58% of our patients. Evaluation of response in these patients is often difficult or impossible as disease is mostly not measurable. Thus, physicians in our clinical practice rather took a pragmatic approach and classified response as SD if there were no signs of progression of bone metastases. This may be one explanation for the low rate of PR even for first-line-treated patients in our cohort as compared to the rate reported in the clinical trials. The fact that treatment of patients in routine clinical practice is not linked to a strict protocol as in a clinical trial, which defines time intervals for evaluation of response and confirmation of tumor response, and the retrospective nature of our study may also have contributed to this difference. Looking at the DCR i.e. including patients with SD results from our cohort actually compare well with those reported from the trials: 82% in first-line vs. 75% (13) and 45% in second-line or more or 57.1 % in third-line or more, compared to those reported by Blum et al. in patients with a median of three prior lines of therapy at 26% (100 mg/m2) and 37% (125 mg/m2) (15).
In the cohort of patients with first-line treatment, the median PFS and median OS have not yet been reached. Considering patients with two or more or three or more lines of treatment, the median PFS (7.5 and 3.1 months) and OS (11.2 months) were at least comparable with the data reported by Blum et al. i.e. 3 (100 mg/m2) and 3.5 months (125 mg/m2) and 9.2 and 9.1 months, respectively (15).
Overall, nab-paclitaxel was well-tolerated. Fatigue was the most frequently reported grade 3 or more adverse event at 27.8%. However, it is nearly impossible to separate fatigue as a consequence of the cytotoxic treatment from fatigue as a symptom of the underlying malignant metastatic disease. Interestingly, despite our patient population being heavily pre-treated peripheral neuropathy was less frequent than reported in the controlled clinical trials. The incidence of peripheral neuropathy of grade 2 or more was 16.7% in our cohort and only one patient (2.8%) had grade 3 neuropathy. This compares favourably to the grade 3 and 4 neuropathy rates of 26% and 22%, respectively, in the 150 mg/m2 arm in the first-line trial reported by Gradishar et al. (14) and to 25% and 17% (100 mg/m2) and 51% and 19% (125 mg/m2), respectively, in the Blum et al. trial (15). One may argue that adverse events and particularly neuropathy, are likely to be more thoroughly captured in clinical trials than in clinical routine and that it is thus not appropriate to compare incidences. However, we believe that this does not apply to our Center. Awareness of this critical toxicity is high at our Center due to the reported incidence of peripheral neuropathy from the clinical trials with taxanes, and in particular with nab-paclitaxel. Thus, patients are informed about the risk of developing peripheral neuropathy and the treating physicians as well as the nurses, have this toxicity in mind during their patient consultations. With the occurrence of grade 2 or more peripheral neuropathy immediate action was taken in the form of dose reductions. Except for the patient with grade 3 neurotoxicity, treatment was continued and peripheral neuropathy was not the reason for stopping treatment with nab-paclitaxel.
The mean number of cycles administered in our cohort in patients with two or more lines of therapy was somewhat lower than that in the Blum et al. trial with a mean number of cycles of 5.3 for the 100 mg/m2 dose and 4.7 for the 125 mg/m2 dose (15). The median number of cycles administered as first-line to patients in our cohort was 5 and clearly lower than the median of 10 cycles reported for the 150 mg/m2 nab-paclitaxel arm of the Gradishar et al. trial (14). As reported in the trial by Gradishar et al. (14) we had to reduce the starting dose of nab-paclitaxel in practically every second patient, and in our cohort, approximately every second patient required a dose delay. All of this may have contributed to the efficacy results in first-line but also to the more favorable tolerability profile regarding peripheral neuropathy in our experience.
In the palliative treatment of patients with MBC, efficacy and tolerability have to be balanced considering the individual patient's characteristics. In our hands, weekly nab-paclitaxel with a starting dose of 150 mg/m2 was an effective and tolerable therapy in routine clinical practice that could be handled in first and second line. In extensively pre-treated patients with MBC, a lower starting dose should be considered, which may result in a higher drug exposure and a higher efficacy. Of course, the methodological limitations of a retrospective chart review have to be acknowledged. But, overall, our results seem to be at least comparable to those from the prospective controlled clinical trials. In particular, the incidence of peripheral neuropathy was lower than reported in the relevant clinical trials and was managed effectively with dose reductions.
Footnotes
-
Disclosure
This study was supported by Celgene Corporation, Summit, NJ, USA. The Authors received editorial support in the preparation of this manuscript from Dr. Susanne Hell, funded by Celgene Corporation. The Authors were fully responsible for all content and editorial decisions for this manuscript.
- Received May 7, 2013.
- Revision received May 23, 2013.
- Accepted May 27, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.