


Abstract
Background/Aim: The present retrospective study was conducted to measure Wilms' tumor-1 (WT1) mRNA levels in the peripheral blood of patients with acute myeloid leukemia (AML) in order to examine any association with the clinical outcomes. Patients and Methods: A total of 58 AML patients were evaluated retrospectively in our institution. WT1 transcripts were determined by real-time reverse transcriptase-polymerase chain reaction in peripheral blood samples. Results: WT1 levels at diagnosis did not vary according to response of induction treatments, and the levels were comparable between the patients with durable remission and the patients with relapse of disease. WT1 levels at the completion of the treatment were higher in the group with relapse of disease than in the group with sustained remission. Detectable WT1 transcripts after the completion of chemotherapy courses were associated with poor prognoses. Conclusion: WT1 mRNA levels at treatment completion may predict for prognosis of AML.
The standard induction chemotherapy regimen achieves complete remission rates of more than 70% in young-adult patients with acute myeloid leukemia (AML) (1-4). However, long-term survivors account for only 30-40% of patients because of disease relapse (1-4). It is therefore important to predict therapeutic outcomes by detecting minimal residual diseases (MRDs), which will help formulate individualized treatment modalities including allogeneic stem cell transplantation for improving patient survival (1-6).
One strategy to monitor MRD is to measure Wilms' tumor-1 (WT1) mRNA in peripheral blood (PB) (7). WT1 was first identified as a tumor suppressor gene associated with the etiology of Wilms' tumor (8). Because different deletions and point mutations of WT1 have been described in this tumor type, the mutated WT1 protein is thought to be involved in carcinogenesis. WT1 is also overexpressed in the majority of AML cases, indicating that it is a useful marker for monitoring MRD (9-12).
It has been suggested that high WT1 expression at diagnosis or after chemotherapy correlates with poor prognosis (13-17). However, it is yet to be determined whether the optimal time for measuring WT1 in the treatment course, is before or after treatment. The present retrospective study was conducted in our department aiming to evaluate WT1 mRNA levels in the PB of patients with AML during the treatment course. The level of WT1 transcripts in PB was examined for any association with leukemia parameters and prognoses.
Patients and Methods
Patients. Patients who visited the University of Fukui Hospital between January 2005 and May 2011 were included for this study. They were all newly diagnosed with AML (except acute promyelocytic leukemia) and received remission induction chemotherapies. The diagnoses were based on evaluation of aspirated bone marrow (BM) samples using standard techniques, including hemograms, cell surface marker detection, and karyotyping. The classification of AML was made based on standard cytological and histochemical examination of bone marrow smears according to the French–American–British criteria (18). Karyotypic risk was assessed according to the report of Medical Research Council trials (19). This retrospective study was approved by the Ethics Committee of the University of Fukui Hospital (# 686).
Treatment and response criteria. All patients underwent remission induction chemotherapies. Those patients who were 65 years or younger received the standard ‘3+7’ induction chemotherapy with continuous intravenous infusion of cytarabine at 100 mg/m2 on days 1-7 and 30-min intravenous infusion of idarubicin at 12 mg/m2 on days 1-3. They then received 3-4 courses of post-remission chemotherapy when they achieved complete remission (CR). The patients who were older than 65 years of age received one of the following therapies according to the physicians' choice: a ‘3+7’ at reduced doses, a low-dose cytarabine-based regimen, barasertib in a phase I study (20). CR was defined as normalization of PB and BM characteristics, including the disappearance of blasts, granulocyte counts at >1,000/μl and platelet counts at >100,000/μl in PB, as well as ≤5% blasts in the BM (21). Other responses were considered as failures. After the completion of chemotherapy, the patients were discharged and their disease statuses were monitored periodically through physical examinations, blood tests, and BM examinations.

Relationship between peripheral WT1 transcript levels and white blood cell counts (A), and lactate dehydrogenase levels (B).
Measurement of WT1 mRNA levels. PB samples were drawn from the patients at diagnosis, one month after induction chemotherapy, and after treatment completion. The samples were evaluated for WT1 mRNA levels using real-time reverse transcriptase-polymerase chain reaction (RT-PCR). The primers were prepared by BML (Tokyo, Japan) (22).
Statistical analyses. All statistical analyses were performed using Microsoft Excel 2007 (Microsoft, Redmond, WA, USA). All of the graphs were generated using GraphPad Prism (version 5.0) (GraphPad Software, Inc. San Diego, CA, USA). Each comparison was evaluated by the Mann-Whitney two-tailed test. Values of p≤0.05 were considered statistically significant.
Results
Patients' characteristics. Between January 2005 and May 2011, 66 patients with AML were admitted to our Department. Out of these, a total of 58 patients that underwent remission induction chemotherapies, were evaluated retrospectively. The patients' characteristics are shown in Table I.
WT1 transcript levels at diagnosis and leukemia parameters. The PB WT1 transcript levels at onset ranged from <50 (undetectable, below the quantification limit) to 890,000 copies/μgRNA, suggesting a wide variability among patients. WT1 levels at diagnosis correlated with peripheral white blood cell counts (Figure 1A), suggesting that WT1 levels might reflect tumor burden. However, WT1 transcript levels did not correlate with peripheral lactate dehydrogenase levels, BM blast count, or BM cellularity (Figure 1B and 2A and B), nor was it associated with CD34 expression (Figure 2C). Moreover, WT1 levels did not vary among the different karyotypic risk groups (Figure 2D).
Patients' characteristics.

Relationship between peripheral WT1 transcript levels and bone marrow leukemic blast counts (A), bone marrow cellularity (B), CD34 expression in leukemic blasts (C), and karyotypic risks (D). Low vs. Int, p=0.50; Low vs. High, p=0.12; Int vs. High, p=0.14 in D. The bars represent the medians. NCC, Nucleated cell count.
Outcomes of induction treatments. Thirty-seven patients out of 58 (63.8%) achieved CR. In younger patients (≤65 years old), the CR rate was 79.6% (19/24), while the older patients had a CR rate of 52.9% (18/34) (Table I). In the CR group, 18 patients (48.6%) maintained remission for at least two years after the diagnosis, while disease in 19 patients (51.4%) relapsed within two years (Table I). Eight patients from the younger-age group underwent allogeneic stem cell transplantations. No patients in the older group received transplantation.
WT1 levels and therapeutic outcomes. WT1 levels in the PB samples collected over the course of chemotherapy were determined for the patients who achieved CR, but not for those who failed to achieve CR. Among the patients with CR, WT1 levels were highest at diagnosis with a median of 35,000 copies/μgRNA (range: <50-180,000), and the levels decreased as the treatment progressed (Figure 3). The values were lowest at the time of therapy completion. Compared with patients who achieved CR, those who did not achieved CR exhibited a median of 28,500 copies/μgRNA (range: <50-890,000) of WT1 at onset (Figure 4A), indicating no significant difference between the two patient groups. Lactate dehydrogenase levels were also similar at the response of induction treatments (Figure 4B) with a median of 356 IU/l (range: 155-3991 IU/l) for the CR group and 324 IU/l (140-1061 IU/l) for the non-responding group.

The time course of peripheral WT1 mRNA level in the patients who achieved complete remission. WT1 transcript levels were determined at diagnosis, at the time of complete remission, and after the completion of the treatment course. The bars represent the medians.
The patients who reached CR were further divided into two subgroups, including the non-relapsed group with sustained remission over two years and the relapsed group, in which AML relapsed within two years from the diagnosis. WT1 levels at diagnosis did not differ between the two groups (median: 31,000, range: <50-160,000 for the patients with sustained CR; median: 42,500, range: <50-170,000 for the patients who experienced relapse) (Figure 4C). On the contrary, more patients with sustained CR had undetectable WT1 levels after completing chemotherapy (12/14, 85.7%) than patients who experienced relapse (8/17, 47.1%) (Figure 4D). Moreover, undetectable WT1 transcript levels at therapy completion were associated with better prognoses, compared with detectable WT1 transcript levels (Figure 5). The results suggest that the achievement of undetectable WT1 transcript levels after treatment completion might be crucial for better prognosis.
Discussion
Although a high remission rate is achievable by standard induction chemotherapy in patients with AML, nearly half of all patients experience disease relapse. Prediction of prognosis may allow better stratification of treatment, especially for the use of allogeneic stem cell transplantation to improve survival (1.2). In the present study, WT1 transcript levels at diagnosis were not predictive of the therapeutic efficacy in patients with AML (Figures 4A and C). Nevertheless, more patients achieved undetectable WT1 mRNA levels after completing chemotherapy in the non-relapse group compared with the relapsed group. (Figure 4D). Negative WT1 tests were also associated with better prognoses compared with detectable WT1 (Figure 5). The results thus suggest that WT1 mRNA levels that are determined serially may serve as biological markers for predicting prognosis, thus enabling individualized treatment options after induction chemotherapy.
WT1 mRNA levels have been clinically investigated in the context of AML prognosis. The latest publications emphasize on the importance of serial measurements of WT1 transcripts not only at diagnosis but after chemotherapy as well (15-17). Gianfaldoni et al. investigated the prognostic significance of early peripheral blast clearance as assessed by WT1 transcript reduction during the standard induction therapy in 57 adult patients with AML (15). WT1 transcripts were quantified in PB on days 1 and 5 of the treatment. The WT1 ratio between the values at day 1 and 5 was significantly greater in patients who achieved CR compared with the non-responders. The overall survival was significantly longer in patients displaying a greater WT1 ratio than in the ones with a smaller WT1 ratio. The authors concluded that early decrease in PB WT1 transcript level may better predict outcome and should be considered in the management of patients with AML (15). This study clearly showed the importance of the initial patient response to induction treatment, which might reflect the chemosensitivity of leukemia cells. Initial response to the induction treatment is also considered to hold prognostic values in acute lymphoblastic leukemia patients undergoing initial treatment with prednisolone (23). Shimada et al. determined WT1 mRNA expression in BM samples from 158 pediatric patients with de novo AML (16). WT1 expression in the diagnostic samples did not have any prognostic value. However, there was a statistically significant difference in the 5-year overall survival between the WT1-positive subgroup (54.5%) and the WT1-negative subgroup (79.4%), when BM WT1 transcripts were measured after the first induction chemotherapy. The authors concluded that WT1 expression measured in BM after the first induction chemotherapy is a useful predictor of clinical outcome in pediatric AML (16). They also demonstrated that higher WT1 expression was detected in the M0, M3, and M7 AML subtypes and lower expression in the M4, and M5 subtypes. Higher WT1 expression was also detected in patients with AML with inv(16), t(15;17) and Down syndrome, and lower expression in those with 11q23 abnormalities. WT1 levels did not differ among the karyotypic risk groups in our study (Figure 2D). This result might be attributed to the relatively small number of patients we evaluated. Gray et al. determined WT1 transcripts in 107 patients with de novo AML at the time of diagnosis, post-induction, post-consolidation, and relapse (17). They found that higher PB WT1 levels at diagnosis were associated with poorer leukemia-free survival. Moreover, when measured at post-consolidation, the presence of detectable WT1 in PB and BM was associated with poorer leukemia-free survival. The impact of WT1 at diagnosis on disease prognosis is still controversial (14). However, our results were consistant with the correlation between undetectable WT1 transcript levels at post-consolidation and disease prognosis in Gray et al.'s study (Figure 5). Thus, even though the results may not be uniform across different studies, they still suggest that serial measurement of WT1 may provide crucial information on the therapeutic outcome of AML.
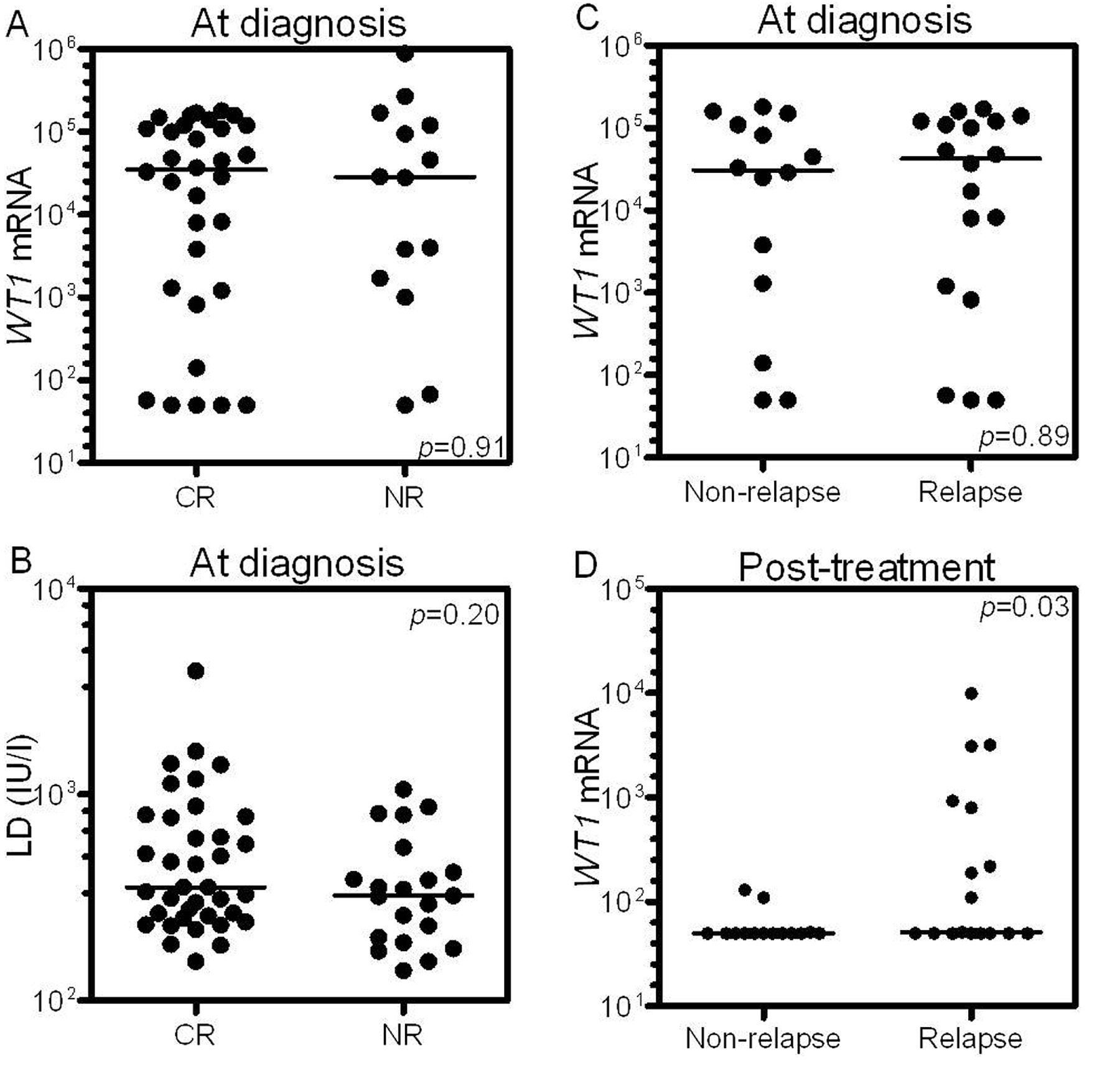
Correlation between WT1 expression and therapeutic outcomes. A: WT1 levels at diagnosis vs. remission induction results. B: Lactate dehydrogenase (LD) levels vs. remission induction results. C: WT1 levels at diagnosis vs. occurrence of relapse within two years from the diagnosis. D: WT1 levels at treatment completion vs. occurrence of relapse. CR, Complete remission; NR, no response. The bars represent the medians.
There are several limitations to the present study. Firstly, the number of patients evaluated was relatively small and the study was conducted retrospectively at a single institution. The association between WT1 transcript levels and karyotypic risk classification or AML subtypes may be revealed more clearly by increasing the number of enrolled patients. Secondly, the follow-up period was short. Lastly, the treatment regimens for older patients were not uniform. Nevertheless, the present study suggests that the WT1 transcript levels after completion of a chemotherapy course may predict the prognosis of AML, which may then enable the individualization of treatments for patients with poor prognosis.

Overall survival curves for the patient groups with and without detectable WT1 expression at treatment completion (p=0.019, log-rank test). The patients who underwent allogeneic stem cell transplantations were excluded.
- Received May 13, 2013.
- Revision received June 16, 2013.
- Accepted June 18, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}