


Abstract
Background: Claudins are integral membrane proteins that constitute tight junctions. The aim of this study was to determine the clinical significance of claudin-1 in terms of the cell–cell adhesion, considering the poorly-differentiated tumor component. Patients and Methods: A total of 344 cases of stage II and III colorectal cancer were enrolled. We evaluated the expression of claudin-1 by immunohistochemistry and the extent of the poorly differentiated component. Results: Low expression of claudin-1 was associated with lymphatic involvement, histological differentiation, extent of poorly-differentiated component, reduced disease-free and overall survival. Multivariate analysis indicated that lymph node metastasis, venous involvement and low claudin-1 expression were independent predictors of recurrence, and that lymph node metastasis, venous involvement and low claudin-1 expression were associated with poor survival. Conclusion: Our study not only showed the significance of low expression of claudin-1 as a predictor of poor prognosis of colorectal cancer but also supported the concept of grading of the poorly-differentiated component.
Claudins are cell membrane proteins which play an integral role in the formation and function of tight junctions (1, 2). Tight junctions are the most apical cellular adhesion points that regulate paracellular permeability through their barrier function, and are critical for epithelial cell polarity due to this function (3, 4). The cellular organization observed in normal differentiated tissues is often lost in cancer, where tumor cells frequently exhibit reduced differentiation and cell polarity (5, 6). These features are important for the development of invasive phenotypes and the acquisition of metastatic potential (7). However, the role of the claudin family is only now starting to be understood. The mechanisms of regulation of claudins and their exact roles in the process of tumorigenesis remain largely unknown (8). Abnormal expression of claudin proteins has been reported in several types of adenocarcinomas. Up-regulation or down-regulation of claudins is known to be related to the carcinogenesis and metastasis of various types of cancer. For example, claudin-3 was reported to be up-regulated in ovarian and prostate carcinomas, and claudin-7 was reported to be down-regulated in oral squamous cell (9), breast (10) and thyroid carcinomas (11). However, studies of the clinical correlation between colorectal cancer and the expression of claudin-1 have shown conflicting results. Some reported up-regulation (12-14), while others have reported down-regulation of claudin-1 in colorectal cancer (15, 16).
The purpose of this study was to examine immunohistochemically the expression of claudin-1 and to determine its association with disease progression in colorectal cancer. To support our results, we also used the new histological grading system, POR reported by Ueno et al. (17, 18). A POR is a newly-defined region in which a tumor has no glandular formation, a higher POR grade being associated with a poor prognosis.
Patients and Methods
Patients and specimens. A total of 344 stage II and III (TNM staging) colorectal cancer cases were reviewed. All patients underwent curative surgery at the Department of Surgical Oncology (First Department of Surgery) of the Osaka City University Graduate School of Medicine (Osaka, Japan) between 2003 and 2008. The patients' characteristics are summarized in Table I. The mean age of the patients at initial surgery was 66.8 years (range: 26-90), and 197 males and 147 females were included in this study. Of the tumors, 200 were of the colon and 144 were of the rectum. Patients with familial adenomatous polyposis or inflammatory bowel disease, or those who had died within 30 days of surgery were not included in the analysis. No patient received chemotherapy or radiotherapy before surgery. All patients were informed of the investigational nature of this study and provided written informed consent.
Association between claudin-1 expression and the clinicopathological parameters in patients with colorectal carcinoma.
Pathological review. Slides of tumors stained with hematoxylin and eosin were examined by an experienced gastrointestinal pathologist. The depth of invasion (pT category), lymph node involvement (pN category), and pathological staging of all surgically-resected tumors were assessed according to the Union for International Cancer Control (UICC) TNM classification (19). Out of the 344 patients, 174 were diagnosed pathologically to have TNM stage II lesions and 170 had stage III lesions. The degree of tumor differentiation was defined based on the guidelines of the Japanese General Rules for Clinical and Pathologic Studies on Cancer of the Colon, Rectum and Anus (20). The grade of the poorly-differentiated component (POR) was assessed by using the tumor grading system based on the extent of the poorly-differentiated component (17, 18).
Follow-up. In 146 out of the 170 patients with stage III disease, adjuvant chemotherapy was given for at least six months. All patients were followed-up regularly by physical and blood examinations with mandatory screening by colonoscopy, ultrasound and/or computed tomography. The patients were observed for more than three years, and the mean duration of follow-up was 51.7 months for the survivors who were alive at the date of their last visit or who were checked by telephone.
Immunohistochemistry. Immunohistochemical staining for claudin-1 was performed on 4-μm paraffin sections of each colorectal cancer sample. Slides were stained with claudin-1 antibodies (polyclonal rabbit, 1:100, Zymed Laboratories South San Francisco, CA, USA). After deparaffinization in xylene and being rehydrated in a graded ethanol series, followed by rinsing with water, antigen retrieval was performed by microwaving the samples three times at 500 W for 5 min each in 10 mM sodium citrate (pH 6.0).
Following H2O2 and serum blocking, the slides were incubated with the primary antibody at room temperature overnight. The secondary antibody was a biotin-labeled goat anti-rabbit IgG (1:500, Nichirei, Tokyo, Japan). Detection was performed with the DAB kit (Histofine SAB-PO Kit; Nichirei, Tokyo, Japan) for 3 min. Slides were counterstained with hematoxylin, dehydrated, cleared and mounted on glass coverslips.
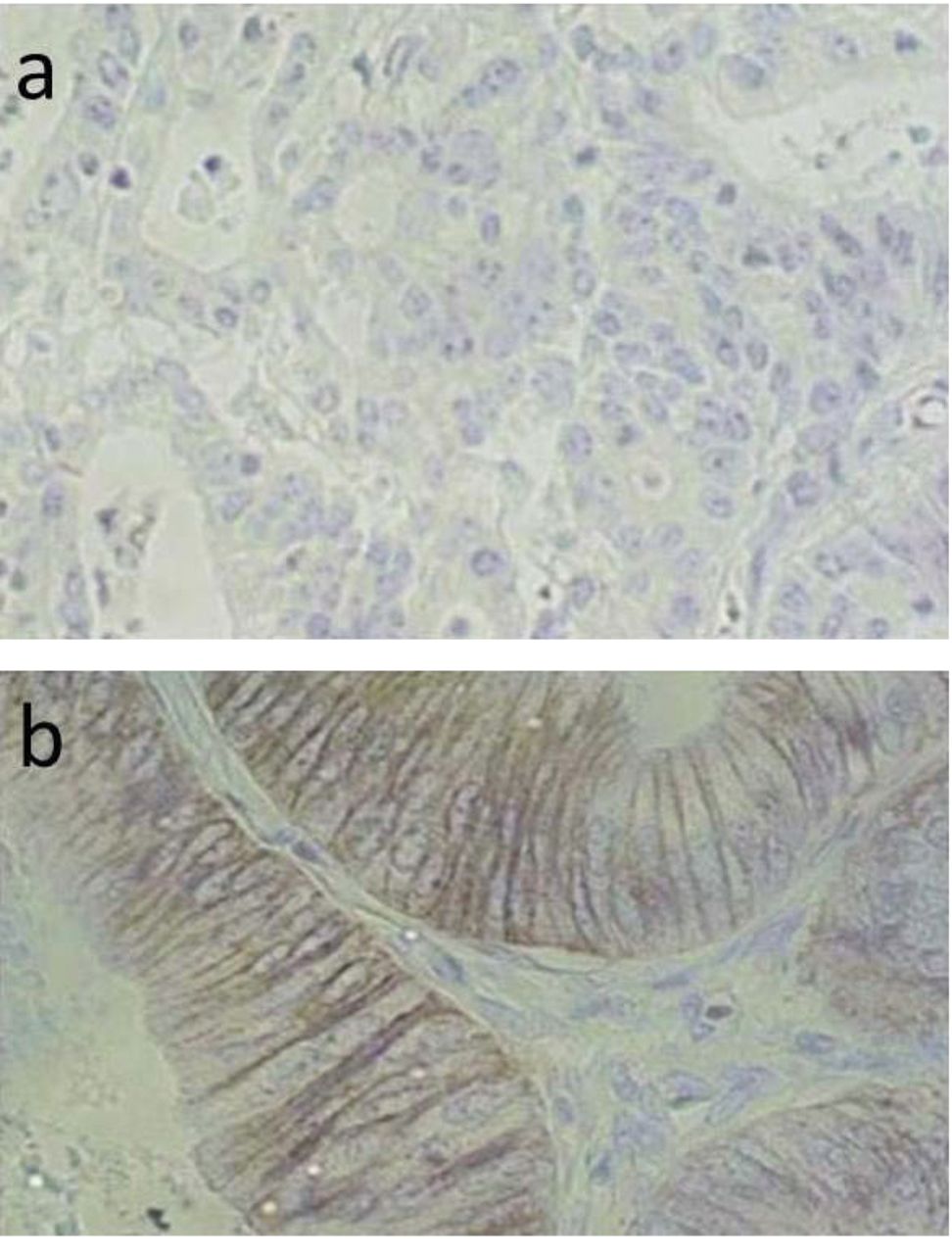
Claudin-1 expression in colorectal cancer (×400). a: Claudin-1 immunoreactivity is absent in the membrane of tumor cells in this case. b: Claudin-1 immunoreactivity is present in the membrane of tumor cells in this case.
Assessment of immunostaining. The immunostaining was classified as follows: 0, no immunostaining present; 1, <25% of cells positive; 2, 25-50% of cells positive; 3, 51-100% of cells positive. In the evaluation, only membrane-bound positivity was considered to be significant, and cytoplasmic or nuclear immunoreactivity was ignored (Figure 1).
In addition, the staining intensity was ignored. The results were analyzed by two observers who had no knowledge of the clinicopathological data at the time of the analysis.
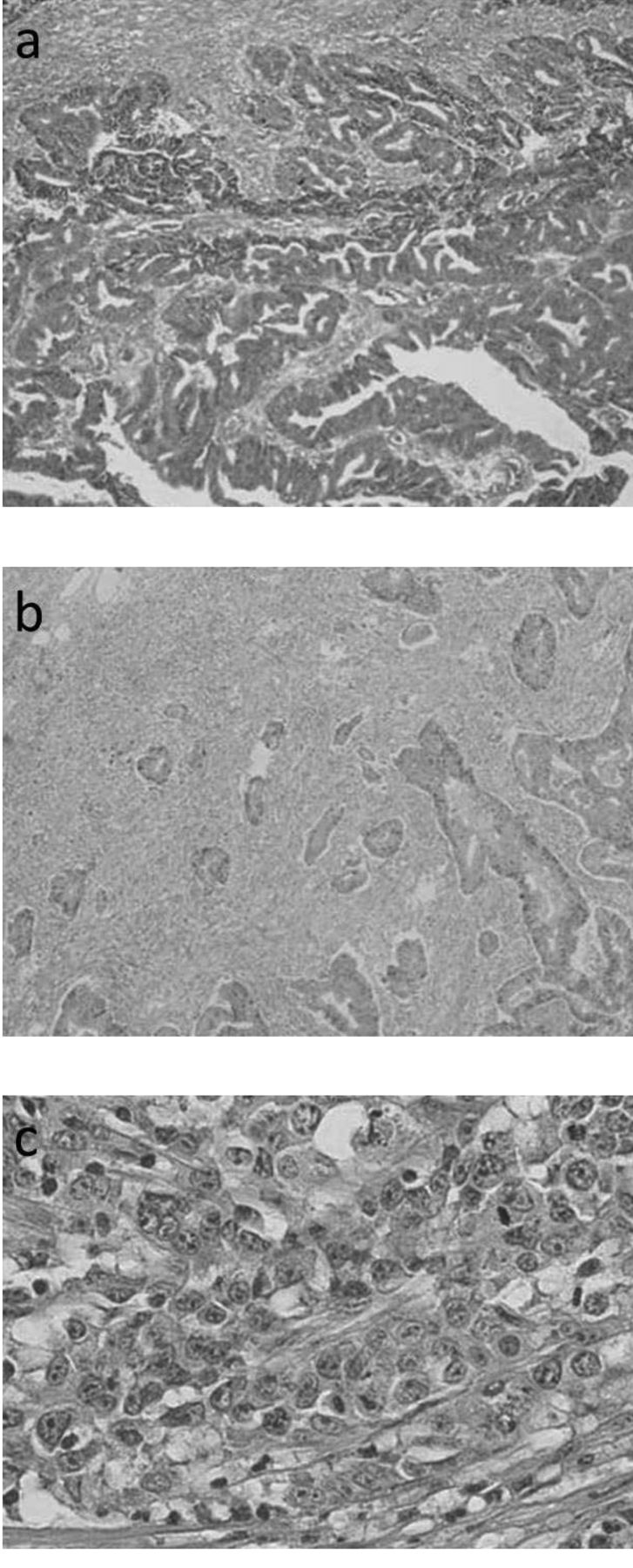
Assessment of the extent of the POR. Firstly, the largest POR area in the tumor was determined by surveying the entire tumor with a low-magnification objective lens (step 1). Next, the area chosen as the POR was examined to determine whether it completely filled the microscopic field of a ×400 lens (step 2). If it filled the field, the tumor was classified as grade 3. When the microscopic field of the ×400 lens was not occupied by the POR area alone, we focused on cancer clusters without gland formation composed of five or more cancer cells, which were mainly observed in the selected area. The number of solid cancer nests (SCNs) in the microscopic field of a ×40 lens was counted in the area where the SCNs were most numerous (step 3). Tumors with fewer than 10 SCNs were classified as grade 1, and those with 10 or more SCNs were classified as grade 2 (Figure 2) (17, 18).
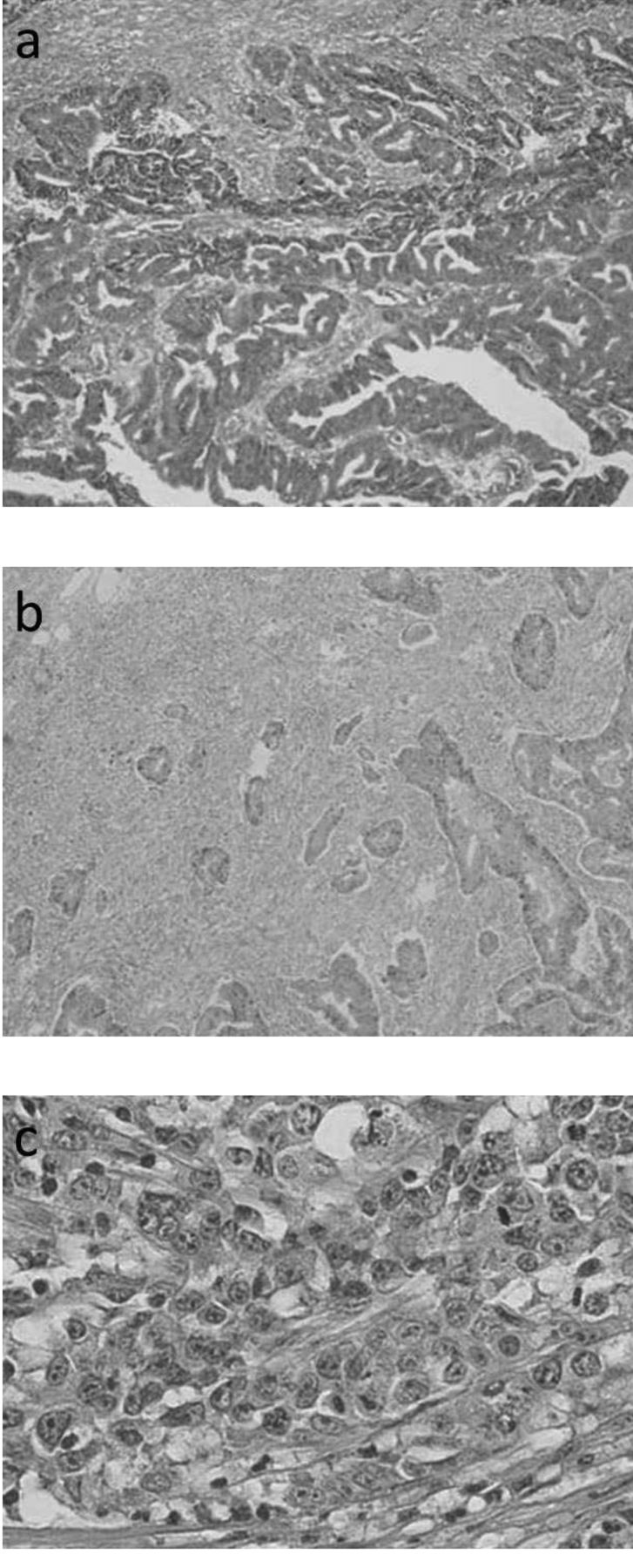
The poorly-differentiated component (POR) in colorectal cancer a: POR grade 1. The number of solid cancer nests in the microscopic field of a ×40 lens was fewer than 10. b: POR grade 2. The number of solid cancer nests in the microscopic field of a ×40 lens was 10 or more. c: POR grade 3. The largest POR filled the field of a ×400 lens.
Statistical analysis. For the statistical evaluations, the immunohistochemical staining intensities were grouped as negative (which included scores of 0 and 1) and positive (which included scores of 2 and 3). The statistical analyses were carried out using SPSS, version 11.0.1.0, software program for Windows (SPSS Japan Inc., Tokyo, Japan). Associations between the claudin-1 expression and clinicopathological parameters were analyzed using Fisher's exact and χ2 tests. The univariate survival analysis was carried out according to the Kaplan–Meier method. Differences in survival curves were assessed with the log-rank test. Multivariate analysis was performed according to the Cox regression model. Two-tailed p-values ≤0.05 were considered to be statistically significant.
Results
Clinicopathological characteristics. The mean tumor size was 4.83 cm (range=0.8-11.0 cm). The histological details of the cases are provided in Table I. Eighty-eight patients in all had recurrent disease. A total of 76 patients died during the follow-up period, 55 of whom died from cancer-related events.
Immunohistochemistry. Staining of 0, 1, 2 and 3 was observed in 62, 48, 112 and 122 cases, respectively. The majority (n=234) of colorectal cancers stained positively for claudin-1.
POR grade. Grade 1, 2, and 3 POR was observed in 134, 132 and 78 cases, respectively.
Correlation between the expression of claudin-1 and the clinicopathological parameters. Loss of claudin-1 expression had a significant relationship with lymphatic invasion (p=0.038), poor tumor differentiation (p<0.001), high POR grade (p=0.024) and recurrence (p<0.001) (Table I). An assessment of the prognosis showed that the overall and disease-free survival were significantly worse in patients with claudin-1-negative tumors (Figure 3). However, the claudin-1 expression was not correlated with other clinicopathological parameters.
The correlation between disease-free survival and various clinicopathological factors are shown in Table II. In the univariate analysis, the disease-free survival had a significant relationship with lymphatic involvement, venous involvement, the POR grade, lymph node metastasis and claudin-1 expression. However, the multivariate analysis indicated that only venous involvement, lymph node metastasis and low claudin-1 expression were independent risk factors for the recurrence of colorectal cancer.
The correlations between the overall survival and various clinicopathological factors are shown in Table III. In the univariate analysis, the overall survival had a significant relationship with venous involvement, lymph node metastasis and claudin-1 expression. The multivariate analysis indicated that venous involvement, lymph node metastasis and low claudin-1 expression were independent risk factors for recurrence and for poor prognosis of colorectal cancer.

The Kaplan–Meier postoperative survival curves. The disease-free (a) and overall (b) survival among colorectal cancer patients defined by the status of the claudin-1 expression. Both the disease-free and overall survival were significantly worse in the patients with claudin-1 negative tumors.
Discussion
Disease recurrence is a major problem in patients who undergo surgical treatment for colorectal cancer because it is associated with a poor prognosis. Therefore, it would be very beneficial to identify the risk of disease recurrence after a potentially curative operation for colorectal cancer.
Correlations between the disease-free survival and various clinicopathological factors.
Correlations between the overall survival and various clinicopathological factors.
We focused on the expression of claudin-1, a cell membrane protein that plays an integral role in the formation of tight junctions, because the loss of inter-cellular adhesion in the neoplastic epithelium is the initial step in the process of metastasis (21). Some earlier studies indicated that there was an association between the expression of claudin-1 and the prognosis after curative surgery for colorectal cancer. Matsuoka et al. reported that reduced expression of claudin-1 was associated with a poor prognosis in colorectal cancer by using cluster analysis of claudin-1 and -4, E-cadherin, and β-catenin expression (15). Resnick et al. also reported an association between low expression of claudin-1 and a poor prognosis on a tissue microarray study (16).
In this study, we found that a low expression level of claudin-1 was correlated with recurrence and poor patient survival, compared to patients with positive claudin-1 expression. In addition, in the multivariate analysis, the expression of claudin-1 proved to be an independent prognostic factor for patients with colorectal cancer.
When we considered the associations between claudin-1 expression and the clinicopathological parameters, we found that low claudin-1 expression was correlated with poor tumor differentiation. This result suggests that the loss of claudin-1, a factor associated with inter-cellular adhesion, led to a loss of paracellular permeability and cell polarity, and therefore contributed to the underlying disorganization of colon cancer cells (3, 4).
We also focused on the poorly-differentiated component of the tumors. The concept of a poorly-differentiated component is a new pathological index advocated in recent years, and the poorly-differentiated component is defined as a region in which cancer has no glandular formation (17, 18). Special attention was paid to the deepest invaded area, called the invasive front (22), because the tumor morphology in the tumor's leading front is known to reflect the biological behavior of the tumor (23). Ueno et al. reported that an increase in the poorly-differentiated component was associated with a poor prognosis (18). The reduction of inter-cellular adhesion might trigger the release of cancer cells from the primary cancer nests (24). In addition, cancer cell clusters without glandular formation (i.e. the poorly-differentiated component) may have been released from the primary cancer nest, and may be one step in the process of metastasis, which can be analyzed microscopically.
In this study, we found that a low expression of claudin-1 was associated with a higher POR grade. Furthermore, we found that in many cases, the expression of claudin-1 was especially low in the poorly-differentiated component. These results support our hypothesis that a low expression of claudin-1 is a predictor of disease recurrence and poor prognosis in colorectal cancer.
Various regimens of adjuvant chemotherapy have been administered to patients with advanced colorectal cancer in an attempt to prevent recurrence after curative surgery. An analysis of the claudin-1 expression in resected tumor specimens may provide additional information to identify the patients at high-risk for recurrence who need intensive adjuvant chemotherapy, such as chemotherapy with adjuvant 5-fluorouracil, leucovorin, and oxaliplatin (FOLFOX).
In conclusion, this retrospective study demonstrated that the loss of claudin-1 expression is an independent prognostic factor for recurrence and poor survival in patients with colorectal cancer. If these findings are confirmed by a larger study, it might be possible to identify patients with a high risk of disease recurrence and use this information to plan for more aggressive surveillance and therapy.
Acknowledgements
There are no conflicts of interests to report for any of the Authors.
- Received May 10, 2013.
- Revision received May 24, 2013.
- Accepted May 27, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}