


Abstract
Background: Primary central nervous system lymphoma (PCNSL) is a type of extranodal non-Hodgkin lymphoma that involves only the central nervous system. Untreated PCNSL in the elderly has a rapidly fatal course. Patients and Methods: In this retrospective study, we evaluated the demographics, management, and outcomes of patients over 60 years of age with PCNSL at our institution. Results: A total of 54 patients with a median age of 67 years were included in the analysis. The initial treatment regimens included whole-brain radiation therapy (WBRT), chemotherapy with or without consolidation WBRT. The median progression-free survival (PFS) was 8.0 months (95% confidence interval CI=2.7-22 months) and the median overall survival (OS) was 38 months (95% CI=18-65 months). On multivariable analysis, age younger than 70 years and Karnofsky Performance Status (KPS) no less than 70 were favorable prognostic factors for both OS and PFS. Conclusion: Aggressive treatment strategies for elderly patients with PCNSL with good performance status can lead to improved outcomes in this patient population.
Primary central nervous system lymphoma (PCNSL) is a rare form of non-Hodgkin lymphoma (NHL) that is confined to the brain parenchyma, cerebrospinal fluid (CSF), spinal cord, leptomeninges, or eyes. PCNSL accounts for approximately 3-4% of all primary brain tumors (1, 2). Patients over 60 years of age account for approximately half of those diagnosed with PCNSL, and it is important to evaluate the outcomes and identify the best management strategies for this patient population (3). Whole-brain radiotherapy (WBRT) improves outcomes in PCNSL from less than four months with best supportive care to approximately 12-18 months (4, 5). In patients greater than 60 years of age, however, the median survival with WBRT alone is only eight months (5). High-dose methotrexate-based chemotherapy regimens in combination with WBRT have resulted in improved survival ranging from 30 to 60 months (6-9). However, a high rate of neurotoxicity occurs, particularly in elderly patients treated in this manner (10). Recent retrospective studies in older patients have shown that methotrexate-based chemotherapy, avoiding WBRT upfront, can be an effective option (11). Although this approach results in high response rates, the omission of WBRT appears to produce shorter progression-free survival (PFS) in the elderly patients (11).
Despite the therapeutic advances, prognosis in older patients is worse compared to younger patients, even when the two groups are treated in a similar manner (3). Age and performance status have been identified as the two most important prognostic factors, with older age being associated with worse prognosis (12). In this study, we sought to elucidate the prognostic factors, treatment responses and outcome in a large cohort of elderly patients with PCNSL treated at the Cleveland Clinic, Ohio, USA.
Patients and Methods
In this retrospective study, we reviewed the charts of patients who were diagnosed and treated for PCNSL and were older than 60 years at the time of diagnosis at the Cleveland Clinic between January 1986 and December 2010. We excluded patients who were HIV-positive or had systemic lymphoma with CNS involvement. Patients were identified from the Brain Tumor and Neuro-Oncology Center database by histological diagnosis. During individual chart review, we confirmed the diagnosis and collected information of patients' demographics, disease presentation, initial and salvage therapy, and the clinical outcome. The Institutional Review Board approved this retrospective review CHRV 0106-CC961.
Patients were followed-up with regular brain magnetic resonance imaging (MRI) or computed tomography (CT), as well as routine neurological examination. We used previously reported criteria for response assessment (12). Complete response (CR) was defined as no contrast enhancement, no concurrent use of corticosteroid, negative CSF cytology, and a normal slit lamp eye examination. Progressive disease (PD) was defined as 25% increase of present lesions or emergence of new lesions, positive CSF cytology, or new ocular disease. All other patients were defined as the group of partial response or stable disease (PR/SD). PFS was defined as time from the date of treatment initiation to the date of disease progression. Overall survival (OS) was defined as the time from the date of diagnosis to the date of death.
Statistical analysis. In this study, categorical variables are summarized with frequency counts and percentages, and compared with Fisher's exact test. Continuous variables are summarized with medians and ranges. In the survival analysis, patients alive or those with no documented disease progression at the last follow-up were censored for OS or PFS, respectively. The Kaplan–Meier method was used to summarize time-to-event data. We used log-rank test and Cox proportional hazards regression to assess potential prognostic factors in univariate analysis. The optimal cutoff point for certain continuous variables was determined using recursive partitioning analysis in a conditional inference framework (13, 14). Cox proportional hazards regression was also used for multivariable analyses to identify potential prognostic factors when potential confounders were adjusted. Akaike information criterion was used during model selection process in a forward/backward fashion (15). The proportional hazards assumption was assessed based on the scaled Schoenfeld residuals with both tests and graphical diagnostics (16). In this study, comparisons with p<0.05 were considered statistically significant. All tests of statistical significance were two-sided. Statistical analyses were performed using R software package 3.0.0 (R Development Core Team, 2013; R Foundation for Statistical Computing, Vienna, Austria).
Results
Patients' characteristics. Fifty-four patients with PCNSL over the age of 60 years at diagnosis at our Institution from 1986 to 2010, met the inclusion criteria for final analysis. The median age at diagnosis was 67 years (range=60-89 years). The median Karnofsky performance status (KPS) at presentation was 70 (range=20-90). The median duration of symptoms was 1.5 months (range=0.1-13 months). Cognitive change was the most common initial symptom at presentation, seen in 27 patients (50%). Other symptoms in order of decreasing frequency included ataxia, aphasia, hemiparesis, ocular symptoms, headache, and seizure (Table I and Table VI). Initial sites of involvement included brain parenchyma in 53 patients (98%), leptomeninges in three patients (5.6%), and the eyes in one patient (1.9%). Three patients (5.6%) had more than one anatomical site involved. The diagnosis was established by stereotactic brain biopsy in 41 patients (76%), tumor resection in 12 (22%), slit lamp examination of the eye in four (7.4%), vitrectomy in three (5.6%), CSF cytology in two (3.7%), and CSF flow cytometry in one patient (1.9%). The median follow-up time for OS was 17.5 months (range=0.5-96 months). Twenty-nine patients (54%) were deceased at the last follow-up, among whom 24 patients (86%) had died from PCNSL.
Initial treatment. The initial treatment regimens included WBRT, or chemotherapy with or without consolidation WBRT. Forty-three patients (80%) received chemotherapy alone and five patients (9%) received WBRT alone, six patients (11%) received chemotherapy followed by consolidation WBRT. Among the patients who received chemotherapy with or without WBRT, 40 (74%) received methotrexate-based therapy; nine patients (17%) received non-methotrexate-based therapy, which contained high-dose cytarabine, temozolomide, rituximab, procarbazine, lomustine, etoposide, carboplatin, or cyclophosphamide. The median total dose of initial WBRT was 28.5 Gy (range=14-45 Gy).
Among these patients, 20 (37%) achieved a CR, 15 (28%) had PR/SD, while 19 (35%) had PD during treatment. The median PFS was 8.0 months (95% CI=2.7-22 months) (Figure 1A). The median OS was 38 months (95% CI=18-65 months) (Figure 1B). Patients treated with chemotherapy followed by consolidation WBRT had significantly higher response rates and longer survivals than patients who received WBRT alone (Table I, Figure 1C and D). No patients who received WBRT alone achieved a CR. In addition, methotrexate-based chemotherapy offered significantly longer PFS than non-methotrexate-based chemotherapy (p<0.001). No apparent significant treatment-related neurotoxicity or death were observed.
In univariate analysis, we evaluated potential prognostic factors such as age, gender, KPS, symptoms duration, prior malignancy, year of diagnosis, symptoms, and multiple site involvement for response rate, PFS, and OS (Table I). Recursive partitioning analysis identified 70 years as the cut-off point for age and 70 as the cut-off point for KPS. None of the potential prognostic factors were found to predict response to therapy. However, younger age, higher KPS were favorable factors for longer OS. Age was the only favorable prognostic factor for PFS, although higher KPS had a trend (p=0.08) towards longer PFS (Table I). When these factors were subjected to multivariable analysis, age older than 70 years and KPS less than 70 were the only prognostic factors for both poorer OS and PFS (Table II). The patients were divided into three prognostic groups based on the number of poor prognostic factors (0-2). The median PFS and OS for the group with no poor prognostic factors were 24 months and 65 months, respectively, as compared to the median PFS and OS of 0.6 month and 2.6 months in the group with all poor prognostic factors, respectively (Table III, Figure 1E and F).
Patients' characteristics and outcomes with initial treatment.
Salvage treatments. Twenty-four patients had disease relapse records after the initial therapy. Disease recurred in the brain parenchyma in 17 patients (71%), brain parenchyma and leptomeninges in three (12%), eye and leptomeninges in two (8.3%) brain parenchyma and eye in one (4.2%), and the eye only in one (4.2%). Leptomeninges and ocular disease were treated with intrathecal and intraocular chemotherapy, respectively. The first salvage therapy included WBRT, or chemotherapy with or without WBRT. WBRT alone and non-methotrexate-based chemotherapy were used more frequently in the salvage setting than at diagnosis. However, there were no differences among these regimens regarding response rates and survival (Table VII). Univariate analysis did not identify age and KPS as the significant prognostic factors for PFS from the first salvage treatment (Table VII). Table IV summarizes and compares the clinical outcome of both initial therapy and the subsequent three salvage therapies. Patients were less likely to achieve CR with subsequent salvage therapies (37% with initial therapy and 0% with third salvage therapy). PFS also decreased from 8.0 months with the initial therapy to 3.3 months with the third salvage therapy (Table IV).
Multivariable analysis of overall survival (OS) and progression-free survival (PFS) for initial therapy.
Discussion
In this elderly PCNSL cohort, patient demographics and disease presentation are similar to those reported in previous studies, suggesting that the reported patient cohort is representative of elderly patients with PCNSL (3). Patients who received methotrexate-based chemotherapy had improved outcomes and less toxicity compared to those managed more conservatively with WBRT alone (3).
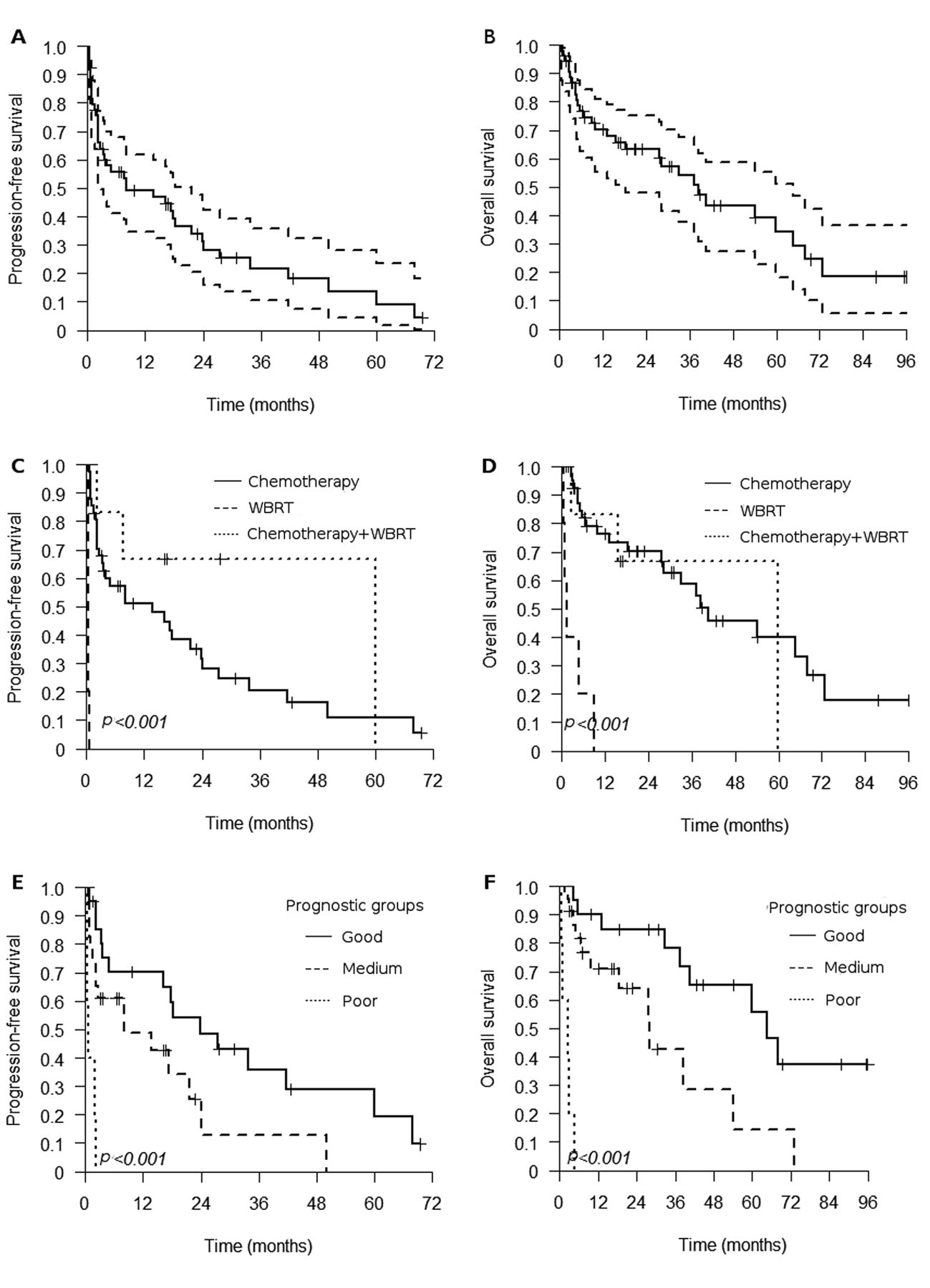
Progression-free survival (A) and overall survival (B) of patients who received initial therapy (dashed lines represent 95% confidence intervals). Progression-free survival (C) and overall survival (D) of patients who received the initial therapy stratified into chemotherapy only, whole-brain radiation therapy (WBRT) only, and chemotherapy followed by consolidation WBRT. Progression-free survival (E) and overall survival (F) of patients in good, medium, and poor prognostic groups.
Prognostic groups.
Treatment, response, and survival.
Previous studies on older patients with PCNSL.
Patients' characteristic, response, and survival for the initial treatment.
In our cohort, advanced age was associated with less chemotherapy or combined chemoradiotherapy use and increasing use of radiation therapy alone, a less preferable approach as radiation at standard doses in older patients increases the risk of vascular-related dementia (17). Eighty-two percent of our patients (for whom treatment data was available) were treated initially with methotrexate-based chemotherapy. A smaller percentage of patients (7%) received WBRT alone.
In our cohort, patients who received high-dose methotrexate-based chemotherapy regimens had a median OS of 54 months compared to 1.4 months of those treated with WBRT alone. Although the number of patients treated with WBRT was small (only five in our series), generally patients with poor performance status and older age (>80 years) tend to be treated with WBRT alone. Survival is generally superior when chemotherapy is part of the initial treatment plan and is noted to be higher for methotrexate-based regimens as compared to non-methotrexate-based chemotherapy. The patients who received non-methotrexate-based chemotherapy had significantly worse median OS and PFS of 3.1 and 2.1 months, respectively, compared to those receiving methotrexate. One possible explanation is that patients who were older and/or who had a lower KPS were judged not well enough to tolerate high-dose methotrexate and therefore received non-methotrexate-based chemotherapy or WBRT.
Patients' characteristic, response, and survival at the first relapse or progression.
We reviewed the available literature regarding elderly patients treated with methotrexate-based regimens (Table V) (3, 8, 11, 18, 19). The reported PFS and OS range from 5.9 to 24 months, and 14 to 37 months, respectively. In this study, recursive partitioning analysis identified age and performance status as prognostic factors for both OS and PFS. Medium and good prognostic groups based on the age and KPS cutoffs had median PFS of 8 and 24 months and median OS of 28 and 65 months, respectively. These outcomes are comparable to those reported by others (3). Although the available data, including our analysis, are retrospective in nature, the information suggests a consistent improvement for this population receiving methotrexate-based chemotherapy compared to WBRT alone. In addition, methotrexate-based chemotherapy is not only effective, but also safe for elderly patients. Although toxicity data were not available for the entire patient cohort, no significant treatment-related toxicities were seen in this study, which is consistent with low toxicity reported by previous studies (3). This observation is likely due to the decreased/delayed use of WBRT in elderly patients. The toxicity of high-dose methotrexate (4 g/m2) was evaluated in a prospective manner as part of a multicenter study evaluating the role of adjuvant WBRT (20). The analysis demonstrated no significant differences between methotrexate-related toxicities in patients aged >60 years versus those aged <60 years (20).
This study has several limitations, including the inherent biases of a retrospective study. Some of the information was not universally available for all the patients, especially patients treated before the electronic medical record era. Therefore, we combined the patients with PR and SD to the therapy for analysis. We also accept that there is referral bias in this single-center study. One would expect that older debilitated patients would not be referred to a tertiary care center for further care, which suggests that these data are biased in favor of patients with a better KPS than a population with similar age. Data on other important variables such as quality-of-life measures, and treatment-related toxicities on all patients were not available. Nonetheless, this study reflects a relatively large group of older patients with PCNSL, a rare disease in this patient population, exploring prognostic factors, and outcomes of specialized treatment practices.
Although elderly patients diagnosed with PCNSL have a poor prognosis compared to younger patients, aggressive management with methotrexate-based chemotherapy in appropriate patients can improve outcomes. Elderly patients remain vulnerable to the toxicities of therapies, and the best treatment approach for these patients remains unclear. Prospective trials are needed to determine the best treatment approach in this patient population.
Footnotes
-
Disclosures
Dr. Ahluwalia's disclosures are speakers' bureau for Merck & Co., Inc and advisory board for Genentech. There are no potential conflicts of interest for other authors. No funding was given for this study.
- Received May 7, 2013.
- Revision received May 22, 2013.
- Accepted May 23, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}