


Abstract
Curcumin, a natural polyphenolic compound derived from turmeric (Curcuma longa L), has proven to be a modulator of multiple intercellular signalling pathways linked to inflammation, to proliferation, growth, invasion, drug sensitivity, angiogenesis and metastasis of cancer cells. Although curcumin has shown significant efficacy in cell culture studies, it has shown limited efficacy in clinical studies when administered in conventional oral formulations. This discrepancy is largely attributed to its poor oral bioavailability, which may result from its poor solubility, its poor pharmacokinetic profile, or a combination of both. To circumvent these barriers, alternative drug delivery strategies and systems should be explored. In this article, after a brief review of the physicochemical properties and pharmacokinetic profiles of curcumin, recent advances in curcumin oral delivery systems are discussed.
Origin
Curcumin is a component of turmeric, which is prepared by pulverizing the dried rhizomes of Curcuma longa L., a plant from the Zingiberaceae family. C. longa L. grows naturally in India and other parts of Southeast Asia. Alcoholic extract of turmeric contains approximately 3-5% curcuminoids and up to 5% essential oils and resins.
More than 10 different curcuminoids, which are compounds chemically related to their principal ingredient curcumin (curcumin I), have been isolated (1). The major curcuminoids are demethoxycurcumin (curcumin II) and bisdemethoxycurcumin (curcumin III) (Figure 1). Commercially available curcumin is not a pure curcumin but a mixture of curcumin (approx. 77%), demethoxycurcumin (approx. 18%) and bisdemethoxycurcumin (approx. 5%).
Sesquiterpenoids such as turmerone and curlone are components of turmeric essential oils and have biological properties similar to those of curcuminoids (2). However, differences in activity among the curcuminoid congeners and other oils remain to be determined. Therefore, when commercially available ‘curcumin’ or ‘turmeric’ is used or the activities of these preparations in the literature are compared, the results may depend on the origin or quality of the preparations.
Pharmacology
In India and Southeast countries, turmeric has been used for centuries as a dietary agent, food preservative and traditional medicine. In Ayurvedic medicine, curcumin is a well-documented treatment for respiratory conditions (asthma, bronchial hyper-reactivity and allergy), runny nose, sinusitis, rheumatisms, ulcers, fever, trauma, diabetes wounds and skin diseases such as psoriasis (3).
In recent years, extensive in vitro and in vivo studies have suggested that curcumin has anticancer, antiviral, antiarthritic, antiamyloid, antioxidant and anti-inflammatory properties. The underlying mechanisms of these effects are diverse and appear to involve the modulation of molecular targets. This modulation may occur through direct interactions by altering signaling pathways or target gene expression. Curcumin regulates the expression of inflammatory cytokines, growth factors, growth factor receptors, enzymes, adhesion molecules, apoptosis-related proteins and cell-cycle proteins. Curcumin also modulates the activities of several transcription factors and their signaling pathways (4-6).
Thus, because of its effective modulation of multiple targets and its safety for human use, curcumin has received considerable attention as a potential therapeutic agent for the prevention and treatment of various conditions and diseases, including cancer, arthritis, allergies, atherosclerosis, ageing, neurodegeneration, obesity, diabetes, hepatic diseases, psoriasis and autoimmune diseases (4).
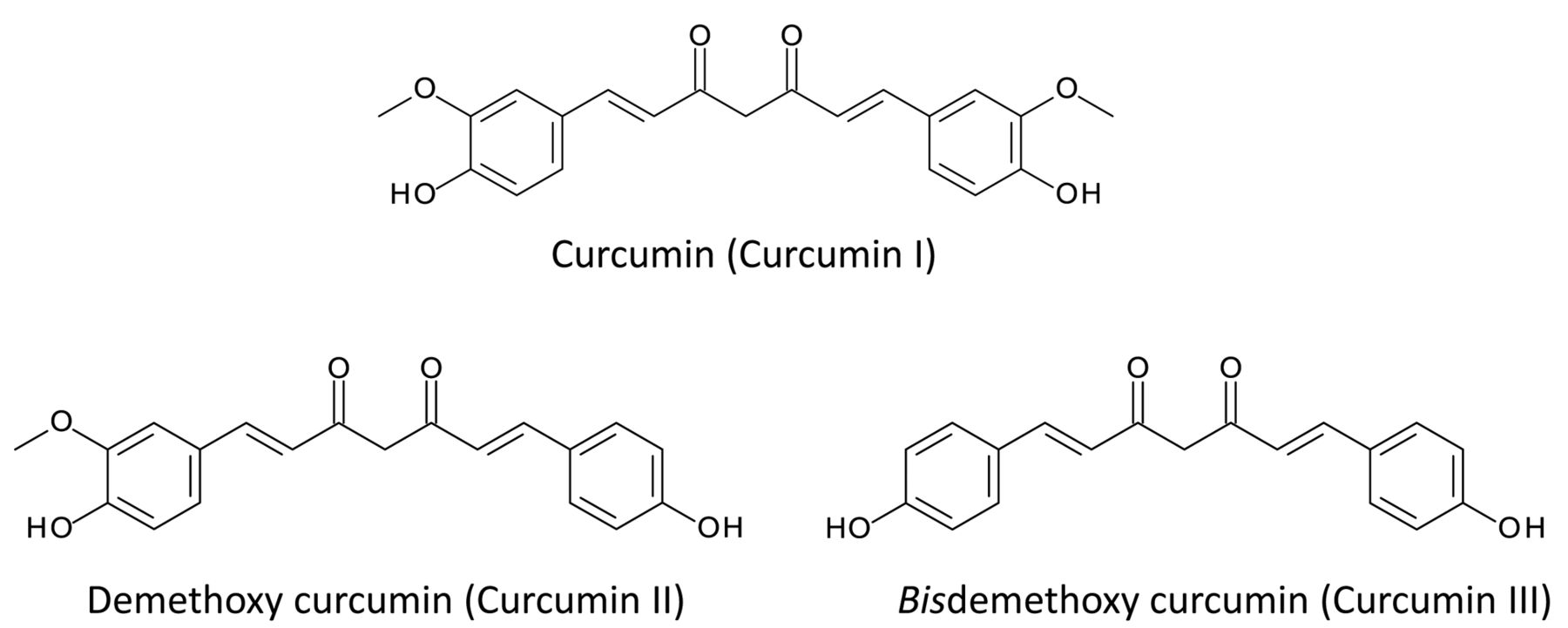
Structure of major curcuminoids found in turmeric.
Curcumin as a potential anticancer agent has gained particular attention because of its ability to suppress the proliferation of various cancer cell lines. Its ability is considered to be due to inhibition of protein kinase-B, Src family protein tyrosine kinases (SFK) and c-JUN N-terminal kinase, and down-regulation of nuclear factor-κB (NF-κB) p65, inhibitory subunit of NF-κB (IκBα), activator protein 1 (AP1), early growth response protein-1 (EGR1), epidermal growth factor receptor (EGFR), human epidermal growth factor receptor type-2 (HER2), insulin-like growth factors (IGF-1R), cyclooxygenase-2 (COX2), lipoxygenase (LOX), nitric oxide oxidase (NOS), tumor necrosis factor (TNF), matrix metalloproteinase (MMP)-2 and -9, urokinase-activated plasminogen activator (uPA), cyclin D and various chemokines (7-10).
Figure 2 shows the result of the search with the term ‘curcumin’ and ‘cancer’ in the PubMed database (http://www.ncbi.nlm.nih.gov/). Given that the number of publications retrieved with the term ‘curcumin’ was about 700 in 2010 (11), those retrieved with the combination ‘curcumin’ and ‘cancer’ account for almost half of the total.
Clinical Studies: Current Status and Issues
A website (http://www.clinicaltrials.gov) maintained by the U.S. National Institutes of Health displays a list of ongoing clinical trials, mainly those occurring in the USA. Table I shows a list of trials using curcumin as of February 2013, excluding those that have been withdrawn and pharmacokinetic studies in healthy volunteers.
The list reveals that many trials on curcumin are designed to study its curative effects in chronic or inflammatory diseases such as dermatitis, stomatitis, chronic colitis or rheumatisms, based on its antioxidative or anti-inflammatory capacities. Furthermore, the list also reveals that the effects of curcumin on the central nervous system related to Alzheimer's disease and depression are being evaluated. Curcumin is often evaluated in conjunction with chemotherapy or radiation therapy during oncology trials. Thus, researchers expect to find not only an anticancer effect due to curcumin alone but also a combinatorial effect of curcumin with chemotherapy or radiation therapy. Positive results are expected in these clinical trials.
In addition to the trials listed in Table I, many clinical studies of curcumin have already been conducted worldwide. There are a few examples with positive outcomes. In a phase II clinical trial on 25 patients with advanced pancreatic cancer, one patient was administered 8 g of curcumin orally for two months showed tumour regression and increased serum levels of cytokines (12). In other clinical trials, curcumin demonstrated some therapeutic effect in high-grade prostatic intraepithelial neoplasia (phase I) (13) and multiple myeloma (monoclonal gammopathy of undetermined significance and smoldering multiple myeloma) (14). However, it is well-known that such examples are exceptional and that most of the trials elicited limited clinical efficacy, despite substantial activity in pre-clinical research.
The discrepancy probably results from two factors: the low bioavailability of present curcumin formulations and the inadequate quality of past clinical studies. Most of the clinical studies had small patient enrolments and were neither double-blinded nor randomized. However, in recent trials, such as those on the list, quality has been improved. In this article, after we review the physicochemical properties and pharmacokinetic profiles of curcumin, we focus on recent advances in novel drug delivery systems for the enhancement of its oral absorption.
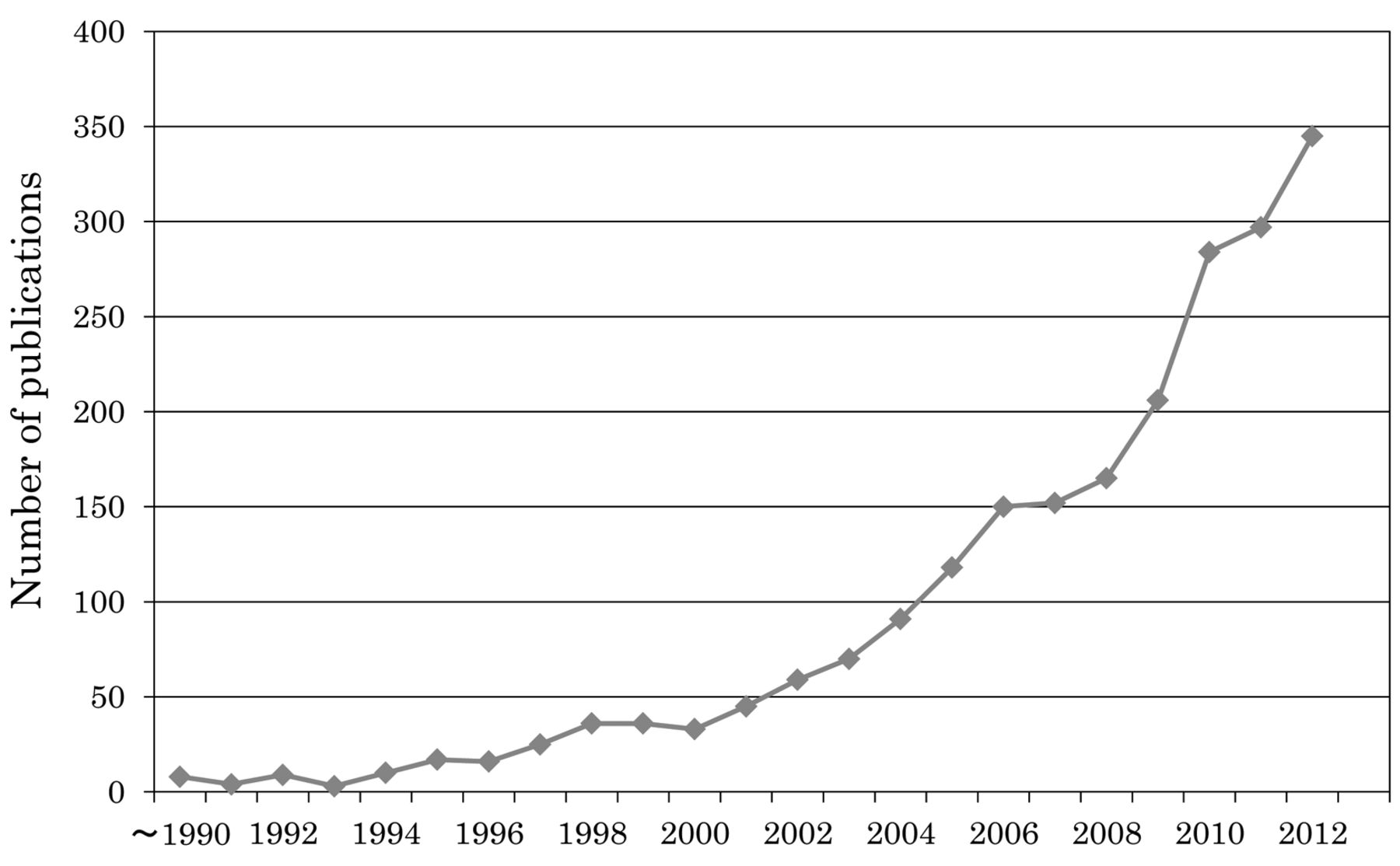
Number of publications retrieved with the search term ‘curcumin’ and ‘cancer’. Source: PubMed (http://www.ncbi.nlm.nih.gov/pubmed).
Physicochemical Properties of Curcumin
Curcumin, a yellow-orange powder, has the molecular formula of C21H20O6 (MW 368.39) and a melting point of 183°C.
The solubility of curcumin in various media is shown in Table II. In water, curcumin is insoluble at acidic and neutral pH, although the solubility increases at alkaline pH because of the ionization of its phenolic hydroxyl group. Its solubility is limited in common organic media such as ethanol and vegetable oils, which makes ordinary liquid formulation difficult. However, recent findings of slightly higher solubility in some oils and surfactants (15, 16) have made it possible to formulate dissolved curcumin in emulsions.
The stability of aqueous solutions of curcumin (water or water/organic medium mixture) is pH-dependent, being reasonably stable at pH 1-6 and unstable at pH >7. Under physiological pH conditions, such as 0.1 M phosphate buffer (pH 7.2) at 37°C, more than 90% of curcumin is degraded within 30 min. In alkaline aqueous solution, hydrolytic degradation products such as vanillin, ferulic acid and feruloyl methane were detected (11). Curcumin is also sensitive to oxygen. Autoxidation proceeds in aqueous solution, and bicyclopentadione was identified as a main degradation product. This pentadione compound has gained great attention because the same compound is formed after reaction of curcumin with LOX or COX (17). Furthermore, curcumin in solution decomposes with light (UV and visible). Therefore, to prevent loss during experiments, strict attention should be paid to the environment (pH, air and light).
Pharmacokinetic Properties of Curcumin
Available evidence indicates that only minute amounts of free curcumin reach the peripheral blood after high-dose oral administration in animals and humans. This low bioavailability is the result of poor oral absorption, rapid metabolism and rapid elimination. In this section, these processes are reviewed.
In this and the following section, concentrations of curcumin (or curcuminoids) in plasma or biological specimens are presented. To evaluate the values, one needs to appreciate the differences between analytical methods. The most frequently used analytical method is the quantification of free curcumin (or curcuminoids) by high-performance liquid chromatography (HPLC), after its extraction from biological samples into an organic phase. In this case, hydrophilic curcumin metabolites such as curcumin glucuronide or curcumin sulphate are excluded from the analysis. However, in several articles, curcumin was assayed after hydrolysis of these metabolites in biological samples using enzymes such as glucuronidase or sulphatase. The values obtained are said to represent the sum of free curcumin and its metabolites, although a negligible amount of free curcumin is usually confirmed in these cases. In the latter case, curcumin and its metabolites were quantified simultaneously. In the following sections, the second and the latter case are specified in the text.
Excerpt from a list of clinical trials with curcumin registered at Clinicaltrials.gov (February 2013).
Curcumin solubility in various media.
Absorption in vitro. The permeability of curcumin through the intestinal tract was recently assessed in vitro using human Caco-2 cells (18). The apparent permeability (from apical to basolateral) was <0.1×10−6 cm/s, which predicted low (0-20%) oral absorption (19). Another study using Caco-2 cells showed that the apparent coefficients in both directions (from apical to basolateral and from basolateral to apical) were similar, which ruled out a role for efflux pathways in the poor oral bioavailability of curcumin (20). These results suggest that the intrinsic membrane permeability of curcumin is very low. However, curcumin conjugates, such as glucuronides or sulphates, are actively transported out of the enterocyte through multi-drug resistance-related proteins (MRP1 and MRP2), which also accounts for the low bioavailability of curcumin (21).
Absorption in rats. Low bioavailability in vivo has been well-documented. When 3H-labelled curcumin was administered orally to rats at 2.4 mg/kg, more than 90% of the applied radioactivity was excreted in the faeces within 72 h, while only 7% was recovered in the urine (22). When unlabelled curcumin was administered to rats at 1 g/kg, the concentration of curcumin in plasma was less than 5 ng/ml. Within 72 h, 65-85% of the curcumin was recovered unchanged in the faeces, while less than 0.01% was recovered in the urine. After 3 h, a major part of the curcumin was found in the small intestine, while only 0.0155% of the applied dose was found in the liver, kidney and body fat (23). In rats, again, when 500 mg/kg of curcumin were administered orally, the plasma Cmax was 60 ng/ml (0.16 μM) at 40 min, and the elimination half-life was 28 min. The bioavailability, compared with intraperitoneal administration, was 1% (24). Low bioavailability was also observed at lower doses. A curcumin crystal suspension, at a 100 mg/kg dose, yielded a Cmax of 35 ng/ml (Tmax=80 min) and an area under the blood concentration time curve (AUC)0-∞ of 11 μg/ml min. The bioavailability, compared with intravenous administration, was 0.9% (25). These studies in rats suggest that curcumin is poorly-absorbed from the gastrointestinal (GI) tract after oral intake and is mostly excreted unchanged with the faeces.
Absorption in humans. Twelve healthy volunteers were administered 10-12 g of curcumin orally by C3-complex™ (Sabinsa), and the plasma concentrations of curcumin and its metabolites were studied. C3-complex™ is a product made of turmeric extracts in which the curcuminoid content is more than 95%. Free curcumin was detected in only one person after 30 min, giving a Cmax of 50 ng/ml. The Cmax of curcumin glucuronide and curcumin sulphate was 2 μg/ml (Tmax=4 h) and 1 μg/ml (Tmax=4 h), respectively. Despite the high dose, the levels of free and conjugated curcumin were very low (26). In another study, patients with high-risk or pre-malignant lesions received daily doses of 4-8 g curcumin for three months. The maximum curcumin concentration observed in their sera was 0.65 μg/ml, and no curcumin was detected in their urine (27). When 10-20 g of C3-complex™ was administered to healthy volunteers, the Cmax of curcumin was only approximately 50 ng/ml at Tmax (2-4 h) (28).
Human pharmacokinetic profiles of curcumin in conventional dosage forms.
A few pharmacokinetic studies have been reported in patients with colorectal cancer. After daily doses of 3.6 g curcumin (C3-complex™) for four months, the Cmax values for curcumin, curcumin glucuronide and curcumin sulphate were 4.1, 8.7 and 4.0 ng/ml in plasma and 0.37, 820 and 18 ng/ml in urine, respectively (29). In 19 patients with colorectal cancer, after a daily oral dose of 4 g curcumin (98% pure curcumin) for one month, no free curcumin was detected in the plasma, while the concentration of conjugates (sum of glucuronides and sulphate) was as low as 80 ng/ml (0.16 μM) (30). In this case, glucuronides and sulphates were reported as free curcumin, after enzymatic hydrolysis. C3-complex™ was recently administered orally to patients with mild-to-moderate Alzheimer's disease at 2-4 g daily. After 24 weeks, the Cmax values for curcumin, curcumin glucuronide, tetrahydrocurcumin (THC) and THC-glucuronide were 7.76 ng/ml, 96.05 ng/ml, 3.73 ng/ml and 298.2 ng/ml, respectively (31).
As described above, only very small amounts of free curcumin or its metabolites were detected after oral administration to rats and humans, even after very high doses. The human absorption data are summarized in Table III.
Distribution and elimination. In rats, as mentioned above, most curcumin is not absorbed through the intestinal tract. It moves down along the tract and can be recovered from the faeces. Transfer to peripheral blood or liver is negligible (22, 23).
In patients with colorectal cancer, the distribution of curcumin in the liver and portal vein was studied. Daily doses of 0.45, 1.8 and 3.6 g of curcumin (C3-complex™) were administered to 12 patients with hepatic metastases for one week before hepatic surgery, which was performed 6 h after the last dosing. No curcumin or reductive metabolites were detected in the liver tissue at the highest dose. In the portal blood, 3 nM curcumin was detected; the levels of the conjugates curcumin glucuronide and curcumin sulphate were around the detection limit (3 nM) (32).
Penetration of colorectal tissue was also studied in patients with colorectal cancer. After they received up to 4 g of curcumin for several days, the concentration of curcumin in the colorectal tissue was only 20 nmol/g (370 ng/g) (30).
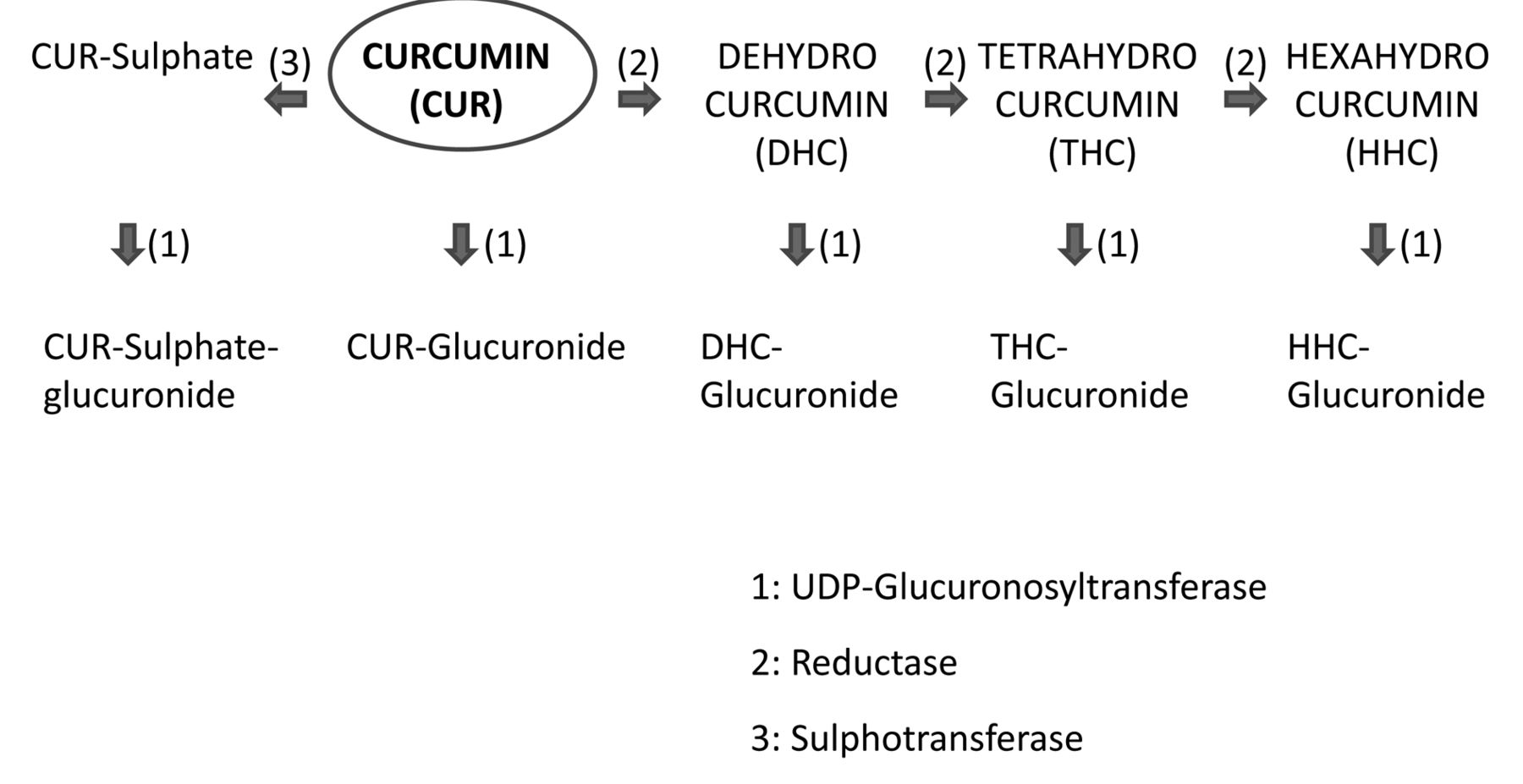
Metabolism. The metabolic pathway of curcumin is shown in Figure 3. Curcumin is metabolized by phase I and II enzymes. Phase I is a reductive process catalysed by enzymes, including alcohol dehydrogenase (ADH), in the cytosol of the liver or the intestinal mucosa (33). The metabolites in this phase include dihydrocurcumin (DHC), THC and hexahydrocurcumin (HHC), and they exist either freely or as conjugates, mainly glucuronides. Conjugate formation occurs via phase II metabolism. UDP-glucuronosyltransferases found in enterocytes or hepatocytes catalyse glucuronide formation, while sulphotransferases catalyse sulphate formation.
Therefore, if curcumin is absorbed through the intestinal tract, some of it may form a glucuronide or a sulphate by phase II metabolism in the intestine or liver, while some of it may form reductive metabolites by phase I reaction, followed by conjugation to form glucuronides or sulphates of the reductive metabolites. In circulating blood, curcumin glucuronides or its reductive metabolites are usually detected.

Metabolism of curcumin after oral administration in rodents and humans.
In fact, after oral administration of curcumin to mice, 99% of the curcumin-related material detected is curcumin glucuronide, and the rest includes DHC-glucuronide, THC-glucuronide and THC (34). In humans, as described above, curcumin, curcumin glucuronide, curcumin sulphate, THC and THC glucuronide were detected in the peripheral plasma or the portal vein (26, 29, 31).
Metabolism Inhibition by Adjuvants
If any adjuvant that can interfere with curcumin-metabolizing enzymes is administered concomitantly, absorption of curcumin may increase. The following are examples of such adjuvants.
Piperine. Piperine, an inhibitor of hepatic and intestinal glucuronidation, was co-administered with curcumin to rats and healthy human volunteers. In rats, bioavailability was increased by 154% compared with a control group without piperine. In humans, piperine (20 mg/kg) was co-administered with curcumin (2 g) and a much higher serum level of curcumin was observed from 0.25 to 1 h after drug administration. The bioavailability was 20-times that of the control group (35). However, enhancing bioavailability by inhibiting phase II metabolism must be carefully carried out since many xenobiotics are detoxified through this route.
Turmeric essential oils. Combinations of curcumin with turmeric essential oils (BCM-95™, Biocurcumax™ 500 mg/capsule) led to enhanced and sustained absorption. In a human study, 2 g of the preparations were administered. The Cmax of curcumin at Tmax (3.44 h) was 456.88 ng/ml, while a control curcumin formulation gave a Cmax of 149.8 ng/ml at Tmax (2 h). The bioavailability of this product (based on curcumin AUC) was about 6.93-fold higher than that of a control curcumin formulation and about 6.3-fold higher than a curcumin–lecithin–piperine formulation (36). The mechanisms of these enhancements are unknown.
Issue in curcumin pharmacokinetics: active species. Because of its poor absorption, rapid metabolism and elimination, free curcumin is hardly detected in circulating blood or peripheral tissues. However, in rodent models, curcumin has been shown to prevent cancer not only in the stomach, intestine and colon but also in the skin, soft palate, tongue, sebaceous glands and breast (37). Pilot clinical studies have also associated curcumin consumption with regression of pre-malignant lesions of the stomach, bladder, soft palate, cervix and skin (27). If no curcumin reaches these peripheral organs after oral administration, what accounts for the effects at the sites?
It has been hypothesized that the beneficial effects observed in such organs are mediated by congeners, metabolites or degradation products of curcumin. Whether curcumin metabolites are as active as curcumin itself is not clear. While most studies indicate that curcumin glucuronide and THC are less active than curcumin itself (38, 39), others suggest that they may actually be more active than curcumin (40, 41).
In addition to generation through auto-oxidation, bicyclopentadiones are generated even faster through enzymatic oxidation catalysed by LOX and COX (17). The metabolism and pharmacological activities of bicyclopentadiones derived from curcumin and its demethoxy congeners should be studied.

Schematic illustration of curcumin absorption in luminal epithelial cells. GI: Gastrointestinal.
Novel Oral Delivery Systems for Curcumin
Strategies for enhancement of oral bioavailability. As discussed in the previous section, the low oral bioavailability of curcumin is attributed to the following factors: Low absorption (Insolubility, instability in the GI tract and low membrane permeability); Extensive metabolism in intestine and liver; Rapid excretion.
To improve curcumin bioavailability, sophisticated drug delivery systems must be designed to address each factor.
Absorption of curcumin through luminal epithelial cells is generally considered to occur via passive transport. The permeation rate follows Fick's first law (Eq. 1), which states that the permeation rate (dQ/dt) is proportional to the surface area of the epithelial cells involved (A) and the solution concentration of curcumin at the surface (just outside) of the cells (Ca) (Cb, the concentration inside the cells, is practically negligible as permeated curcumin may be quickly cleared by capillaries)
 (Eq. 1)
where P is the permeability coefficient.
(Eq. 1)
where P is the permeability coefficient.
Figure 4 illustrates the process of curcumin absorption by luminal epithelial cells.
In the GI tract, only soluble curcumin can be absorbed through luminal epithelial cells. Insoluble curcumin descends in the tract, resulting in excretion with faeces. Therefore, solubilizing curcumin in the GI tract (increase in Ca in Eq. 1) is the first step towards enhanced absorption. Reduction in the particle size of crystalline curcumin should result in a higher dissolution rate through an increase in the surface area of the solid. Modification of the crystalline form, such as polymorphisms or an amorphous state, may contribute to an increase in solubility or the dissolution rate. Formation of inclusion compounds with cyclodextrins may also increase the solubility.
Soluble curcumin is exposed to a harsh environment in the GI tract. We should recall that curcumin is chemically unstable even at physiological pH. Therefore, it is necessary for the solute to avoid being ‘naked’ prior to absorption (maintenance of higher Ca in Eq. 1). Entrapment of curcumin molecules or particles in oil droplets, liposomes, polymers or lipid particles may be effective. These various strategies should proceed in areas closer to the epithelial cells and in a wider range of the lumen (increase in A in Eq. 1). To realize these conditions, dosage forms should show good dispersive properties in the GI tract and should localize in the neighbourhood of the mucosal membrane through mucoadhesive properties. If membrane permeation of curcumin is increased using these strategies, enzymatic metabolism in the intestine or liver may be saturated, increasing systemic bioavailability.
Inhibition of curcumin metabolism (Figure 4) with enzyme inhibitors has been described above. Although circumventing rapid excretion or targeting curcumin to the site of action, such as cancer or brain cells, is essential for better bioavailability, such routes are yet to be studied well. Therefore, in the last section of this article, discussion is limited to new delivery systems for the enhancement of oral absorption.
Novel Delivery Systems
In this section, we discuss the performance of novel delivery systems. To evaluate or compare the results, one needs to understand that there is considerable variation between laboratories. For example, The AUC of curcumin after intravenous injection in rats, which is the basis of bioavailability calculations, was presented by three different laboratories. Although the details of the experimental conditions were slightly different, the highest AUC was 350-times the lowest AUC, after dose normalization.
Solid Dosage Forms
Solubility enhancements by manipulation of crystalline forms. Manipulations of the crystalline state are one of the classical methods to increase solubility or the dissolution rate of insoluble curcumin.
Polymorphism and amorphous form of curcumin. A new polymorph, polymorph 2, was recently shown to have increased solubility and dissolution rate compared with the previously studied polymorph, polymorph 1 (42). However, oral absorption of the new crystalline polymorph is not yet known.
Amorphous forms are, by definition, non-crystalline materials and their structure can be considered to be similar to that of a frozen liquid. They are thermodynamically unstable and are the most energetic form, which may result in higher solubility or a higher dissolution rate. Oral absorption of amorphous curcumin was studied in rats. A dose of 250 mg/kg gave a Cmax of 70 ng/ml (Tmax=15 min), which was twice the Cmax of crystalline polymorph 1. Although absorption of the amorphous material was rather rapid, the oral bioavailability (AUC) was improved by only 1.45-fold compared with the control, which was not a significant difference (43).
Solid dispersions. Solid dispersion technology transforms crystalline materials to amorphous materials. Here, an active substance is embedded in a carrier, which is generally selected from suitable polymers. The active substance, which is originally crystalline, is usually transformed to an amorphous form in the dispersion. Thus, this formulation has been recognized as a method to improve dissolution and bioavailability.
A few curcumin dispersions were recently studied in rats. Dispersion in hydroxypropyl methylcellulose acetate succinate (HPMC-AS) gave a Cmax of 147 ng/ml (Tmax=60 min) at a dose of 20 mg/kg. The AUC (27.1 μg/ml min) was 12-times higher than that of a standard crystalline suspension and resulted in a bioavailability of 10.7% compared with intravenous injections (25). Next, dispersion with polyethylene glycol 660 12-hydroxy stearate gave a curcumin Cmax of 90 ng/ml (Tmax=15 min) at a dose of 50 mg/kg, and rapid absorption was observed. The AUC of the dispersion was five-times higher than that of a standard crystalline suspension (44). The last example is a dispersion of curcumin in cellulose acetate, which gave a Cmax of 187 ng/ml at the same dose. The AUC of this dispersion was eight-times higher than that of a standard crystalline suspension (45).
These results suggest that manipulation of the curcumin crystal itself has limited potential for absorption enhancement, while amorphous curcumin in solid dispersions led to significant increases in bioavailability. However, as the amorphous state is thermodynamically unstable, transformation to the crystalline state during storage should be carefully monitored.
Complex formation: Cyclodextrin inclusion compounds. Cyclodextrins (CDs) are cyclic oligosaccharides consisting of six to eight sugar molecules in a cyclic structure. They can sequester insoluble compounds within their hydrophobic cavity, resulting in improved solubility and enhanced chemical or enzymatic stability. A hydroxypropyl-β-CD inclusion compound with curcumin showed enhanced oral absorption in a rat study (46). Compared with a curcumin suspension, its Cmax (370 ng/ml) was about nine-times higher at a 500 mg/kg dose. A γ-CD inclusion compound, CAVAMAX™ W8 from Wacker, is available on the market (47). In a rat study, CAVAMAX™ W8 led to 10-20-times greater amount of total curcumin in the plasma than pure curcumin powder after oral administration. Curcumin was assayed after hydrolysis of the plasma with glucuronidase and sulphatase. Bioavailability was about 0.2%, which is four times that of standard curcumin.
Phosphatidylcholine complexes. A molecular complex of curcumin with phosphatidylcholine can be formed by refluxing in organic solvents. Phospholipid complexes, liposomes and micelles can reduce the hydrophobicity of curcumin; these carriers can also increase the permeability by interacting with membrane components.
Absorption of a curcumin:hydrogenated soy phosphatidylcholine complex was studied in rats. At a dose of 1 g (as curcumin)/kg, this formulation gave a Cmax of 1.2 μg/ml (Tmax=90 min) and an AUC of 524 μg/ml h, while standard curcumin had a Cmax 0.5 μg/ml (Tmax=45 min) and an AUC of 101 μg/ml h (48).
Complexes of curcumin with soy phosphatidylcholine were also prepared and administered to rats at 1 g/kg. The Cmax and AUC were more than three-fold greater than those of a physical mixture of both the components or standard curcumin crystals (49).
Meriva™ (Indena) is a product composed of complexes of curcuminoids (curcumin I, II and III) with lecithin (mainly phosphatidylcholine). Plasma concentrations of the three components were assayed after oral administration to healthy volunteers. Total curcuminoid absorption was about 29-fold higher for this complex than for the corresponding unformulated curcuminoid mixture. However, all the detected curcuminoids were conjugated metabolites (glucuronide or sulphate). Of note, complex formulation increased the absorption of curcumin II much more than that of curcumin I. Thus, the major plasma curcuminoid after administration of the complex was not curcumin I but curcumin II (50).
Micron (nano) particles. Nanoparticles can provide greater penetration of membrane barriers because of their small size. Besides their size, their potential for targeting specific organs through modification makes them excellent drug carriers.
To improve the oral bioavailability of poorly soluble drugs, crystalline particle size reduction to approximately 200-600 nm by high-pressure homogenization or media milling is well known. Absorption enhancement is expected because the increased surface area accelerates the dissolution rate and increases the solubility of the drug with decreasing radius of the spherical particle (Ostwald-Freundlich equation). The enlargement, however, often causes aggregation of particles. Therefore, selection of dispersing agents is also important. The other advantages of this technology include its simplicity, ease of scale-up and narrow particle size distribution.
A nanocrystal solid dispersion of curcumin was prepared using the NanoMill-01 wet-milling system, in which polystyrene beads micronize curcumin crystals (25). The resulting nanosuspension was composed of curcumin, hydroxypropylcellulose SL, sodium dodecyl sulphate (SDS) and water. The mean diameter of the curcumin particles was as low as 250 nm. The nanocrystal solid dispersion was then administered to rats at a dose of 20 mg/kg. The Cmax was 194 ng/ml (Tmax=55 min) and the bioavailability was 14.3%. Curcumin crystals used as a reference gave a Cmax of 35 ng/ml (Tmax=80 min) at a 100 mg/kg dose and a bioavailability of 0.9%.
Another micronized form of crystalline curcumin, Theracurmin™, was prepared from curcumin, ghatti gum and water using a wet grinding mill (Dyno-Mill), followed by high-pressure homogenizer dispersion (51). The mean diameter of the curcumin particles was 190 nm, determined using a laser diffraction scattering method. When Theracurmin™ was orally administered to rats at a dose of 50 mg/kg and 10 mg/kg, the Cmax was 764 ng/ml (Tmax=1 h) and 900 ng/ml (Tmax=1 h), respectively (52). A 30 mg dose of Theracurmin™ or curcumin powder was then orally administered to healthy human volunteers. The AUC of Theracurmin™ was 27-fold higher than that of curcumin powder. The Cmax was 30 ng/ml (Tmax=1 h) (51). The results of a higher dose of Theracurmin™ was reported from the same laboratory (53), where 150 mg and 210 mg doses were administered to healthy volunteers. The Cmax values were 189 ng/ml (Tmax=4 h) and 275 ng/ml (Tmax=2 h), respectively. In these studies, plasma curcumin was assayed after hydrolysis with glucuronidase. Free curcumin was detected neither in rats nor humans. Clinical data of Theracurmin™ have been published recently (54).
Polymer sub-micron (nano) particles. Polymeric submicron- or nanoparticules are particles of diameter below 1 μm, prepared from natural or synthetic polymers, in which curcumin is embedded in the polymeric spheres. Synthetic biodegradable polymers have received great attention in this context. The most widely used polymers have been poly(lactic acid), poly(glycolic acid) and their co-polymers poly(lactic-co-glycolic acid) (PLGA). PLGA microspheres with 20-30 μm size are well-known carriers for sustained release and subcutaneous or intramuscular injections. However, spheres of smaller size have been extensively studied for oral drug delivery.
Curcumin-loaded PLGA nanoparticles with an average particle size of 264 nm were orally administered to rats at a dose of 100 mg/kg (55). The Cmax was 265 ng/ml (Tmax=2 h) and the AUC was about 10-fold higher than that of a standard crystalline suspension.
Similar PLGA spheres with a smaller average size of 200 nm were prepared and orally administered to rats at the same dose (56). The Cmax was as high as 6.75 μg/ml (Tmax=2 h) and the bioavailability (relative AUC compared with that of intravenous administration) was, surprisingly, 26.6%. The bioavailability of a standard crystalline suspension as reference was 4.7%, which seems much higher than the values (around 1%) reported in other studies (24, 25).
In a recent report, PLGA nanoparticles with an even smaller particle size of 163 nm were prepared. A Cmax of 57 ng/ml (Tmax=15 min) was found after oral administration to rats at a 50 mg/kg dose (57).
PLGA sub-micron- or nanoparticles are a relatively new technology for curcumin delivery. Detailed studies investigating issues such as the effects of particle size or differences in manufacturing methods are expected.
Solid lipid nanoparticles (SLNs). SLNs, which are in the sub-micron size range, usually consist of biocompatible and biodegradable materials, such as triglycerides and fatty acids. The production and properties of SLNs have been reviewed elsewhere (58).
SLNs composed of polysorbate 80 (45.45%), soy lecithin (0.58%) and Compritol 888 ATO™ (7.27%) were prepared by microemulsification. The particles were spherical in shape, with an average particle size of 134.6 nm. The SLNs were administered to rats at a dose of 50 mg/kg. The Cmax was as high as 14.3 μg/ml and the AUC was 39 times higher than that of a control curcumin solution (59). In these studies, plasma curcumin was assayed after hydrolysis with glucuronidase. The values reported were the total of free curcumin and curcumin glucuronide.
Another SLN was composed of poloxamer 188, glyceryl monostearate, soy lecithin, medium chain triglyceride (MCT) and curcumin. The particle size was 129 nm. The SLNs were administered to rats at a dose of 80 mg/kg. These SLNs gave a significantly higher Cmax (565 ng/ml vs. 279 ng/ml), shorter Tmax (0.5 h vs. 1.0 h) and greater AUC (820 mg/l h vs. 344 mg/l h) compared with a crystalline curcumin suspension (60).
In LONGVIDA™, curcumin is formulated as LNPs. It is composed of turmeric root extract, soy lecithin, docosahexaenoic acid, stearic acid, ascorbyl esters and inert additives. The curcumin content by weight is 20-30%. In healthy volunteers, 650 mg of the product (130-260 mg curcumin) gave a Cmax of 22 ng/ml (Tmax=2 h). In patients with osteosarcoma, 2000 mg of the product (400-800 mg curcumin) gave a Cmax of 32 ng/ml (Tmax=3.5 h) (61).
Liquid Formulations
Liposomes. Liposomes are a well-established delivery system incorporating poorly soluble drugs and enabling their administration in aqueous mediums. Liposomes are usually used for parenteral administration, and some pharmacokinetic profiles after intravenous injection of curcumin liposomes have been reported (62, 63). Here, however, only examples of oral administration are included. Curcumin-loaded liposomes made with lecithin (SLP-PC70), with an average size of 253 nm, were prepared and orally administered to rats (64). At 100 mg/kg, the Cmax was 319 ng/ml (Tmax=30 min), while the Cmax of a control curcumin crystal suspension was 65 ng/ml (Tmax=2 h). The AUC was 5-fold higher than the control. In this study, curcumin was assayed after hydrolysis with glucuronidase and sulphatase. Curcumin-loaded silica-coated liposomes (157 nm in size) were prepared to protect the particles in the harsh environment of the GI tract (65). These liposomes showed higher stability against artificial gastric fluid and more sustained drug release in artificial intestinal fluid. In a rat study, a 50 mg/kg dose gave a Cmax of 450 ng/ml (Tmax=2 h) and an AUC that was 7.8-fold higher than that of a standard curcumin suspension.
Micron (nano) emulsions. Micron (nano) emulsions are defined as colloidal, optically isotropic, transparent or slightly opalescent formulations consisting of surfactant, co-surfactant oil and water.
A micron (nano) emulsion composed of Capryol 90 (propylene glycol monocaprylate, 11%, oil), Cremophor RH40 (polyethylene glycol 40 hydrogenated castor oil, 44%, surfactant) and Transcutol P (highly purified diethylene glycol monoethyl ether, 42%, co-surfactant) in an aqueous solution was prepared, in which the curcumin solubility was 32.5 mg/ml and the droplet size was 27.3 nm (16). A pharmacokinetic study of this emulsion was conducted in rats and compared with the corresponding suspension. At a dose of 200 mg/kg, the microemulsion had a substantially increased Cmax (3.57 μg/ml; Tmax=138 min) and an AUC (690.5 μg/ml min), while the control, at a dose of 100 mg, had a Cmax of 0.83 μg/ml (Tmax=1.5 h) and an AUC of 153.2 μg/ml min. The bioavailability of curcumin in the emulsion was 22.6-fold higher than that in the control suspension.
A micron (nano) emulsion with a droplet size of 218 nm was prepared using curcumin, oil (MCT), surfactant (Span 20, monostearin, modified starch, Tween 80) and water (66). The bioavailability of this microemulsion was studied in mice at a dose of 197 mg/kg. The Cmax was 29.9 μg/ml (Tmax=1 h) and the bioavailability (compared with intravenous administration) was 9.8%, which was nine-times higher than that of unformulated curcumin.
The rapid absorption from the micron (nano) emulsion was observed in some examples. An emulsion composed of curcumin, PEG 600 and Cremophor was prepared such that the concentration of curcumin was 100 mg/ml and the drop size was 69 nm. At a dose of 1.8 g/kg in mice, the Cmax was 4.73 μg/ml (Tmax=20 min) (67).
In another example of rapid absorption, an emulsion composed of PEG 400, polyethylene glycol, ethanol, Tween 80 and water was prepared with an average drop size of 176 nm (25). With a 20 mg/kg dose administered to rats, the Cmax was as high as 451 ng/ml (Tmax=8.7 min). The clearance from plasma was also rapid and bioavailability was 7.9%, which was less than a nanocrystal suspension or an amorphous dispersion prepared by the same laboratory.
Self-emulsifying Drug Delivery Systems (SEDDS)
SEDDSs are a vital tool in solving the low bioavailability problems of poorly soluble drugs. Using SEDDS, hydrophobic drugs can be dissolved, enabling them to be administered as a unit dosage form for oral administration. When such a liquid system is released in the lumen of the GI tract, it disperses to form a fine (micron/nano) emulsion with the aid of GI fluid. This leads to the in situ solubilization of the drug that can subsequently be absorbed. SEDDSs are composed of either oils and water-insoluble surfactants, or oils, surfactants and co-solvents (both water-insoluble and water-soluble).
Human pharmacokinetic profiles of new curcumin formulations.
If a liquid SEDDS is transferred into a solid dosage form, it combines the advantages of liquid SEDDS with those of the solid dosage form. Solid dosage SEDDSs overcome the limitations associated with liquid formulations, which include manufacturing processes that result in high production costs, incompatibility between the fill and the soft gelatin shell, and storage temperature issues.
A solid SEDDS composed of Aerosil (solid carrier), Lauroglycol Fcc (oil), Labrasol (surfactant) and Transcutol HP (co-surfactant) was studied. The particle size of the oil droplets that were formed after contact with water was around 147 nm. After oral administration to rats at a dose of 100 mg/kg, the Cmax was 156 ng/ml (Tmax=30 min) (15) and the AUC was 7.6-times that of a standard curcumin powder.
Another SEDDS containing Cremophor, Labrasol (surfactant), Labrafac PG, Capryol 90 (oil) and curcumin was prepared and formulated into a pellet dosage form (68). It rapidly formed oil-in-water emulsions with a particle-size range of 25.8-28.8 nm. A pharmacokinetic study of the formulation in rats at a 50 mg/kg dose showed 14-fold increased absorption (AUC 32.3 μg/ml min) compared with an aqueous suspension (AUC 2.3 μg/ml min).
Micelles
The self-association of amphiphile into small aggregates (diameter less than 100 nm) is called micelles. In aqueous solution, the aggregates have a hydrophobic core surrounded by hydrophilic layer. The hydrophobic drugs are then dissolved in the core, thus forming an aqueous solution of the drugs usually for parenteral dosage.
An in situ micelle formation system for curcumin oral absorption was prepared (69). It was composed of water-soluble surfactants and co-solvents: Gelucrie 44/14 (lauryl macrogol-32 glycerides), Labrasol (PEG-9 caprylic/capric glycerides), V.E.TPGS (V.E. PEG 1000 succinate) and PEG 400. Oral bioavailability of the optimized formulation was evaluated in rats at a dose of 250 mg/kg. The control curcumin suspension had a Cmax and AUC of 32.29 ng/ml and 38.07 ng/ml h, respectively. The formulation improved Cmax and AUC by 11.56- and 35.8-fold, respectively over the control.
Among the new systems described above, those with human pharmacokinetic data are summarized in Table IV. For further information on curcumin delivery systems, a few excellent reviews may be recommended (70, 71).
Conclusion
Low oral bioavailability is one of the major reasons why curcumin has been unsuccessful in achieving therapeutic outcomes in spite of its pleiotropic pharmacological properties. In order to increase its absorption through the intestinal membrane, a higher concentration at the membrane surface is most important. Curcumin delivery systems with increased solubility and stability, or accessibility, in or to the GI tract, were introduced. The systems that have been already introduced to clinical research include nanosuspensions, phosphatidylcholine complexes and SLNs. Their bioavailability is far beyond that of the conventional dosage forms. Furthermore, other systems such as polymer particles or nanoemulsions are being extensively studied.
In addition to the advances in delivery technology, simple and reproductive analytical methods should be developed. To begin with, elucidation of active species and required concentration of the species at the site of action must be studied.
In the near future, with advances in science and technology, the therapeutic or preventive benefits of curcumin are expected to surface.
- Received April 4, 2013.
- Revision received June 5, 2013.
- Accepted June 6, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Origin
- Pharmacology
- Clinical Studies: Current Status and Issues
- Physicochemical Properties of Curcumin
- Pharmacokinetic Properties of Curcumin
- Metabolism Inhibition by Adjuvants
- Novel Oral Delivery Systems for Curcumin
- Novel Delivery Systems
- Solid Dosage Forms
- Liquid Formulations
- Self-emulsifying Drug Delivery Systems (SEDDS)
- Micelles
- Conclusion
- References
- Figures & Data
- Info & Metrics