


Abstract
Aim: Triple-negative breast cancer has a poor prognosis due to its aggressive behaviour and lack of effective targeted therapies. We aimed to verify whether clinical and/or pathological features may help us identify triple-negative breast cancer with a different outcome. Patients and Methods: Patients diagnosed with stage I-III triple-negative breast cancer at our Institution were included in the analysis. The impact of various factors (age, menopausal status, tumor characteristics, adjuvant treatment, etc.) on survival was evaluated. Univariate and multivariate analyses were performed. Results: A total of 149 patients were included in this retrospective analysis. At univariate analysis, a better disease-free survival was related to smaller tumour size and absence of lymphovascular involvement or necrosis. At multivariate analysis, tumour size and lympho-vascular invasion were independent prognostic factors. Conclusion: Triple-negative breast cancer represents a heterogeneous disease with different biology and clinical behaviour. These results re-inforce the wide use of adjuvant chemotherapy for all types of triple-negative breast cancer, regardless of tumour size or lymphovascular invasion. New biomarkers are mandatory for a better stratification of this heterogeneous population.
Triple-negative breast cancer (TNBC) is defined by the absence of estrogen receptor (ER), progesterone receptor (PR), and the tyrosine kinase human epidermal growth factor receptor-2 (HER2) overexpression. It accounts for 15-20% of all breast cancer cases, occurring more frequently in young premenopausal women (1-3). TNBC typically presents with a high-grade, ductal histology and a high proliferative rate and necrosis (4). Moreover, it includes a heterogeneous sub-group of tumours by gene expression profiling, although 50-70% of them are basal-like breast cancers (5,6). Several studies have shown that TNBC and basal-like breast cancer present a poor prognosis due to a high rate of early recurrence and distant visceral metastasis, especially to the brain and lungs, compared to other breast cancer subtypes (7-10). The recurrence peak occurs within the first three to five years from diagnosis. On the contrary, late recurrences decline over the following five years. Chemotherapy with standard cytotoxic agents represents the only systemic treatment option for these patients and most of them have an excellent chemosensitivity, especially in the neoadjuvant setting. However, the outcome of most patients is relatively poor, suggesting that current therapy fails to curtail the innately aggressive behaviour of TNBC in the majority of patients. The poor prognosis coupled with a lack of targeted use of therapies is reflected in the high mortality (11-13). Unfortunately, in daily clinical practice, we have no prognostic features predicting prognosis of these patients. Recently, consistent data supported the assessment of basal cytokeratins and androgen receptors (in addition to the traditional parameters such as tumor size and nodal status) in providing prognostic information in the group of TNBC (14-18). Nevertheless, these biological markers are not used in routine practice. Thus, in this retrospective analyses, we investigated the impact of traditional clinical and pathological features in order to identify TNBC with a more aggressive behaviour and a poor prognosis.
Patients and Methods
Patients. The study included all consecutive women diagnosed with invasive breast cancer at our Institution from January 2006 to December 2010. Based on pathology reports, we identified tumours lacking immunohistochemical expression of ER, PR and HER2 (triple-negative status). Patients with stage IV disease or history of other cancers (excluding non-melanoma skin cancer and dysplasia of the uterine cervix) were excluded. Patients' characteristics and clinical-laboratory features included in this analysis were: demographics (age, menopause) and tumour characteristics (tumor size, lymph node status, histological type, grade, presence and amount of vascular invasion, amount and type of a ductal carcinoma in situ component, amount of lymphocytic infiltrate and presence of central necrosis, type of surgery and adjuvant chemotherapy).
Immunohistochemistry. ER, PR and HER2 status determined by immunohistochemistry (IHC) were analysed. IHC analysis was performed on formalin-fixed, paraffin-embedded breast cancer tissue. The ER and PR analysis was based on an IHC assay in which a report of 10% or greater of cells that had nuclear staining for ER, as well as for PR, was considered a positive result. IHC was performed with antibodies to ER (clone: SP1, dilution: 1:200; NeoMarkers, Fremont, CA, USA) and to PR (clone: SP2, dilution: 1:250; NeoMarkers, Fremont) using an autostaining system (Ventana Medical Systems, Tucson, AZ, USA). HER2 IHC used only cell membrane localization for interpretation (Dako, Carpinteria, CA, USA). The intensity of membrans'staining was defined using a semi-quantitative score (0−3+). Tumor staining was compared to the staining of normal breast epithelium from the same patient as a negative control. For clinical purposes, 3+ staining, defined as uniform and intense membrans' staining in more than 30% of invasive breast cancer cells, was considered HER2 overexpression. No staining or weak (1+) and incomplete membrans'staining was considered a negative result. Patients with 2+ IHC staining for HER2 underwent fluorescence in-situ hybridization to confirm HER2 positivity. Triple-negative status was finally diagnosed and re-reviewed by the single study pathologist of our Institution.
Statistical analysis. Disease-free survival (DFS) was defined as the interval between the date of diagnosis of TNBC to the date of relapse or progression of disease, or the date of death from any cause. Overall survival (OS) was defined as the interval between the date of diagnosis of TNBC to death or last follow-up visit. Patients who were not reported to be deceased at the time of the analysis were censored at the date they were last known to be alive. Survival distribution was estimated by the Kaplan Meier method. The association between categorical variables was estimated by Chi-square test. The Cox multivariate proportional hazard regression model was used to evaluate the effects of the prognostic factors on survival. Significant differences in probability of surviving between the strata were evaluated by log-rank test. Hazard ratios and 95% confidence intervals (CIs) were estimated from regression coefficients. A significance level of 0.05 was chosen to assess the statistical significance.
Statistical analysis was performed with the MedCalc package (MedCalc® v9.4.2.0 Software, Ostend, Belgium).
Results
Patients' characteristics. From January 2006 to December 2010, a total of 149 women were included in the analysis (median age=54 years; range=26-83 years). The majority of them (55.7%) had a post-menopausal status. All patients underwent quadrantectomy or radical mastectomy (75.1% and 24.9%, respectively). Neoadjuvant chemotherapy was performed in 23 cases of stage III breast cancer: 22 patients received a regimen with anthracycline and taxane, while a single patient received chemotherapy with capecitabine and vinorelbine. After neoadjuvant chemotherapy, 7 (30.4%) and 8 (34.8%) patients achieved a complete and a partial pathological response, respectively, while stable disease was documented in eight cases (34,8%). Most of the patients presented pT1 tumours (up to 2 cm in size) (53.7%) and pT2 tumours (2-5 cm of diameter) (30.9%). Lymph nodes were disease-positive in 38.2% of cases. Postoperative radiotherapy was delivered after all-conserving surgery; while after mastectomy, external radiotherapy was delivered in 15 (10%) cases because of the presence of four or more affected axillary lymph nodes, tumour size >5 cm or presence of cutaneous or chest wall infiltration at diagnosis. 92.6% patients received adjuvant chemotherapy. Regimens are summarized in Table I.
The median follow-up time was 41.6 months (range=2.5-75 months). The median DFS was 28.49 months (range=2.5-75 months). In 80.7% of cases, distant or local recurrence occurred within the first five years after diagnosis. With regard to the other characteristics, ductal tumours (94%) and a grading of 3 (87.2%) were the most commonly observed categories. The median value for Ki-67 staining was 60% (range 5 to 95%). Patients' characteristics are summarized in Table I.
Univariate analysis. Univariate analysis including age, menopausal status, tumour characteristics, adjuvant treatment, etc. showed that significant risk factors for reduced DFS were: tumour size (p<0.01), lympho-vascular invasion (p=0.003) and necrosis (p=0.007). A better DFS was correlated to a smaller tumour size (≤2 cm) and to the absence of lymphovascular involvement or necrosis. Patients' age, menopausal status, lymph node status, type of adjuvant chemotherapy, grading, Ki-67, intraductal carcinoma and lymphocityc infiltration were not statistically significantly related to DFS (Table II).
Multivariate analysis. Multivariate statistical analysis showed that the significant independent prognostic variables influencing DFS were tumour size (≤2 cm vs. >2 cm; p<0.01; Figure 1), and lymphovascular invasion (presence vs. absence; p=0.02; Figure 2). No statistically significant results were reported for necrosis (Table II).
Discussion
Although TNBC is generally characterized by a high rate of relapse, visceral metastasis and poor survival, its clinical course is heterogeneous, as tumors of apparently homogeneous characteristics may have different outcomes. In the past years prognostic biomarkers such as androgen receptors, and basal cytokeratin expression have also been recommended in order to identify more aggressive TNBC, even if assays for such parameters are not routinely performed (14-18). Currently, due to the absence of reliable surrogate IHC markers, or gene expression profiling, it is difficult to further define subtypes of TNBC. Therefore management decisions largely depend on IHC-defined triple-negative status. So far we have based our risk prediction using only traditional histological and clinical prognostic parameters, such as tumor size and lymph node status. In our whole TNBC series, tumor size and lymphovascular invasion are the most useful prognostic markers to predict for the risk of recurrence. Tumor size is a significant independent variable which largely influences prognosis: a better DFS was related to smaller tumor size (≤2 cm) and this result is consistent with previous studies. Rakha et al. (15) analyzed 282 patients with TNBC and revealed a higher risk of recurrence when larger tumor size (>1.5 cm) was documented, but only in the subgroup of node-positive patients. Conversely, our analysis suggests that tumor size of TNBC has prognostic value which is independent of lymph node status. Nevertheless, the presence of lymph node positivity is not related to poor prognosis and risk of recurrence; this probably depends on the different biology and natural behavior of TNBCs which are characterized by higher risk of distant recurrences than locoregional metastases, especially during the first 3-5 years of follow-up. As a matter of fact, our results confirmed that there is a sharp decrease in survival during the first five years after diagnosis, and distant relapse after this time is not common.
Baseline characteristics of 149 patients included in this study.
Univariate and multivariate Cox regression analysis of factors associated with disease-free survival in triple-negative breast cancer.
The prognostic relevance of lymphovascular invasion in patients with breast cancer was investigated in several studies. Locoregional and systemic spread of breast cancer cells to the lymph nodes and distant organs, respectively, occurs after invasion of tumor cells into the lymphatic channels and the blood vessels. The results of our study are consistent with other reports (19-21) showing that lymphovascular invasion was associated with the development of recurrence and poor prognosis of TNBC. Mohammed et al. (22) examined lymphovascular invasion in 197 basal-like and in 99 TNBC revealing that both the basal and TNBC, exhibited significantly higher lymphatic or microvessel density, or vascular invasion and poorer prognosis than the non-basal and non-TNBC groups did. Higher microvessel density may suggest that such groups may preferentially benefit from anti-angiogenic therapy. Nevertheless, vascular invasion might enable for stratification of TNBC phenotypes into distinct prognostic groups and further research is required to provide sufficient tools to allow for a more personalized tailored approach based on biological and molecular parameters.
In our analysis, no significant differences in DFS were reported for Ki-67, although some experience showed a prognostic role in TNBC. In this setting Kashiwagi et al. documented that TNBC with reduced Ki-67 expression (≤30%) showed significantly better overall survival time (p=0.0181, log-rank) (23). Moreover, there was no statistically significant difference impact of various chemotherapy regimens (anthracycline-based or non anthracycline-based) on risk of recurrence and survival. Therefore results on the the efficacy of anthracycline-based adjuvant regimens in TNBC remain controversial and several analyses seemed to reveal no added benefit for anthracycline over adjuvant classical CMF (cyclophosphamide, methotrexate, and fluorouracil) chemotherapy, suggesting that a non-anthracycline regimen may be adequate for TNBC (24-26).
Conclusion
TNBC represents a heterogeneous disease with different biological and clinical behaviour. In this retrospective analysis, factors related to poor prognosis were advanced tumor stage and lymphovascular invasion; no significant correlation was found for nodal status. These results re-inforce the wide use of adjuvant chemotherapy for all types of TNBC, regardless of tumor size or lymphovascular invasion. New biomarkers are mandatory for a better stratification of this heterogeneous population.
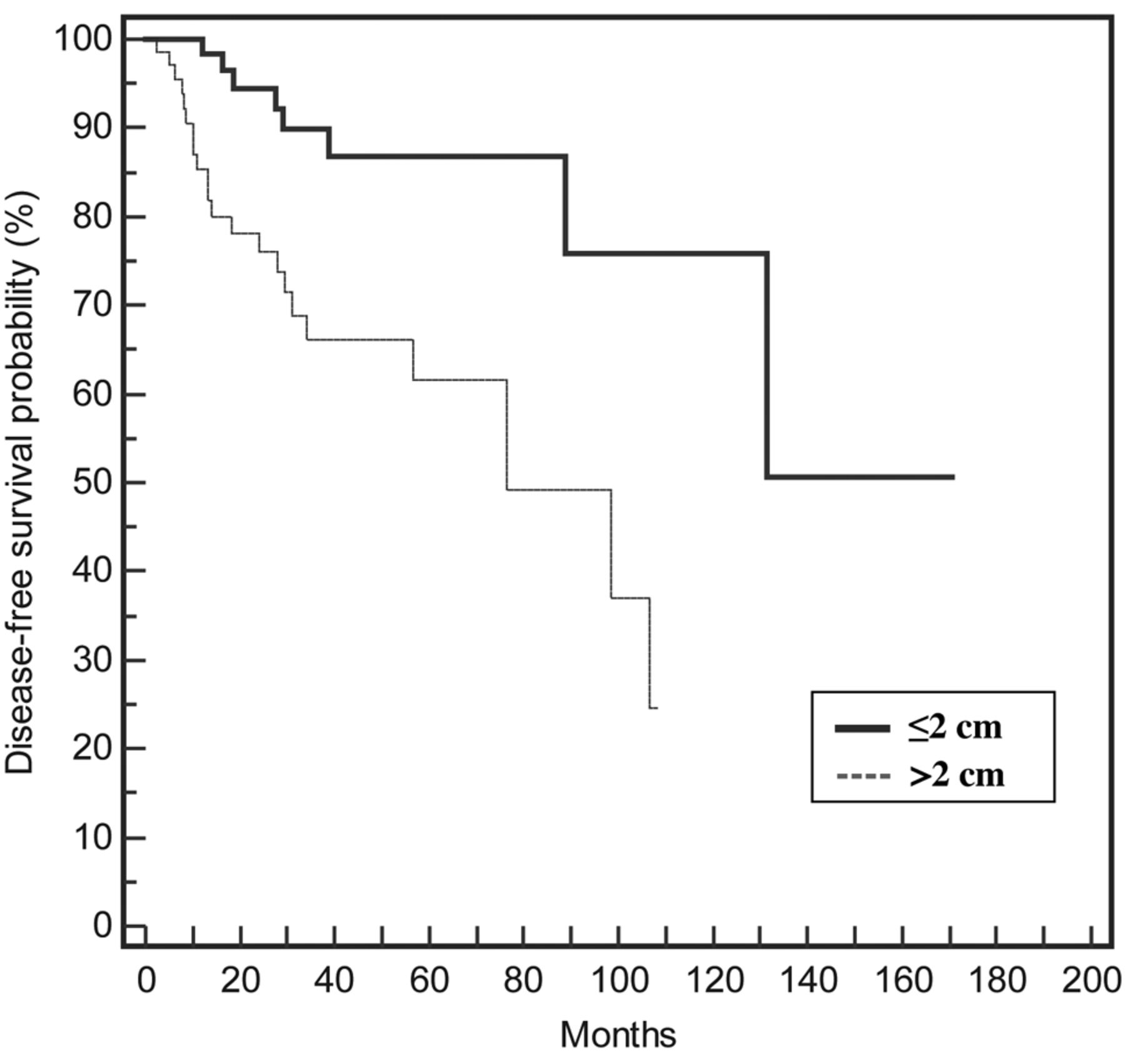
Disease-free survival of patients with triple-negative breast cancer based on tumor size (≤2 cm vs. >2 cm; p=0.004, HR=3.51, CI=1.48-8.28).
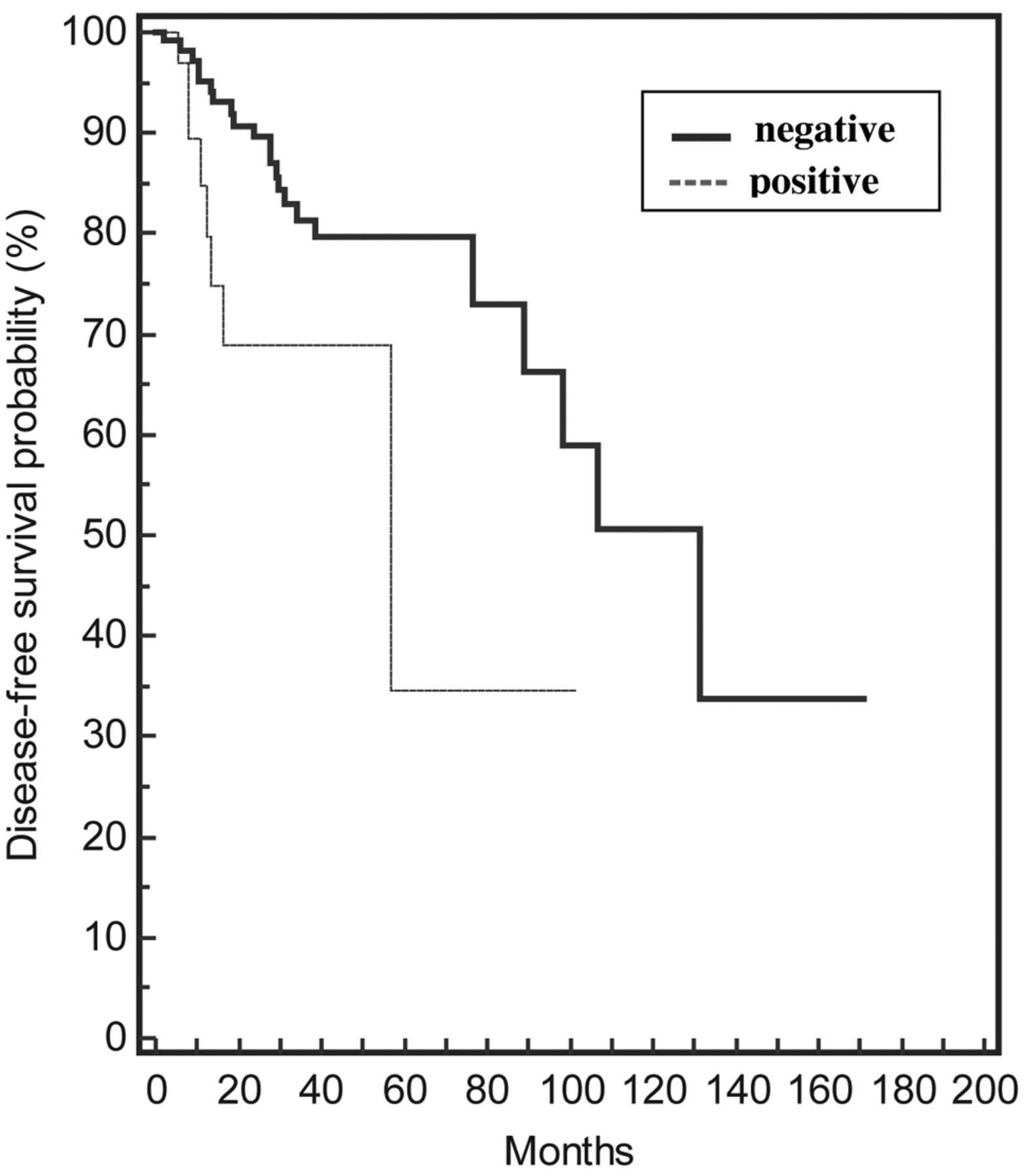
Disease-free survival of patients with triple-negative breast cancer based on lymphovascular invasion (negative vs. positive; p=0.02, HR=3.22, CI=1.19-8.7).
Footnotes
-
Disclosures
All Authors declare no conflict of interests.
- Received April 6, 2013.
- Revision received April 24, 2013.
- Accepted April 25, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}