


Abstract
Background/Aim: Soluble mesothelin-related peptide (SMRP) is regarded as a biomarker of malignant pleural mesothelioma (MPM). Herein, we compared the diagnostic performances of SMRP in matched pleural effusion (PE-SMRP) and serum (S-SMRP). Materials and Methods: Diagnosis on pleural biopsies was performed for all patients including 43 with MPM, 23 with non-MPM pleural metastases (MTS) and 36 with benign (BNG) pleural diseases. SMRP was measured by a MesoMark ELISA (Cis-Bio International Gif/Yvette; France). Results: Using the receiver operating characteristic (ROC) analysis, 12.70 and 1.08 nM were detected as cut-off values to optimal discrimination for PE-SMRP and S-SMRP, respectively. PE-SMRP showed a better diagnostic accuracy than S-SMRP in MPM vs. MTS+BNG (area under the ROC curve=81.6 vs. 70.5; sensitivity=69.8% vs. 46.5%; specificity=88.1% vs. 84.7%; diagnostic odds ratio (DOR)=17.1 vs. 4.8). In S-SMRP-negative patients, PE-SMRP maintained an acceptable performance (Sensitivity=47.8%; DOR=8.3; p=0.001), whereas in PE-SMRP-negative patients, S-SMRP performed very poorly (Sensitivity=15.4%; DOR=1.2; p=0.858). Conclusion: PE-SMRP detection has a superior diagnostic accuracy than S-SMRP detection in the diagnosis of MPM.
Malignant pleural mesothelioma (MPM) is an asbestos-related tumour, arising in the pleural cavity, with a poor prognosis (survival 4-12 months) (1, 2) and a worldwide incidence expected to increase in the next 10 years (3-5).
Pleural effusion (PE) is often the primary manifestation of MPM and can be found in about 90% of patients with MPM at-diagnosis (6-8). PE is obtained by performing pleural aspiration (thoracentesis) and is often important for the initial diagnostic investigation. Without a definite MPM diagnosis, thoracoscopy is recommended. Thoracoscopy is the established method which provides the possibility of visualising the pleural cavity and directly obtaining biopsy specimens for histological and immunohistochemical analyses (9). Thoracoscopy is recognized as the gold standard for the diagnosis of MPM, although it represents an invasive method which should be avoided whenever possible (9). Indeed, the investigation of soluble tumour biomarkers in serum and PE, which can be performed through a minimally-invasive procedure, has been considered (10-12). Among the biomarkers, soluble mesothelin-related peptide (SMRP) has recently received considerable attention. SMRP originates from mesothelin, a 40-kDa cell surface glycoprotein with putative function in cell-to-cell adhesion (13). Mesothelin is expressed by normal mesothelial cells and overexpressed by various types of cancer, such as MPM, pancreatic and ovarian adenocarcinomas in addition to others (14), and may provide opportunities for novel mesothelin-targeted cancer therapy (15).
SMRP can be detected in blood, PE and urine although the mechanisms of SMRP release from the cell surface are unclear. The serum levels of SMRP (S-SMRP) have been found to be significantly increased in patients with MPM (16-22) and, on this basis, S-SMRP has been approved by the U.S. Food and Drug Administration for the diagnosis and monitoring of MPM.
Recently, the PE levels of SMRP (PE-SMRP) were also proposed for the diagnosis of MPM (23-30). Indeed, PE-SMPR was found to be significantly increased in patients with MPM as compared to those with benign pathology (BNG) or non-MPM metastatic tumour (MTS). However, it still remains to be confirmed, in a larger number of patients and from different countries, which of these two tests performs better (25-29). The evaluation of the contribution that each test can give to the diagnosis of MPM may have an important impact on the choice to avoid or to proceed with a more invasive procedure such as thoracoscopy.
The aim of the present study was to compare the diagnostic performance of PE-SMRP and S-SMRP in MPM. For this purpose, we assessed the levels of PE-SMRP and matched S-SMRP in specimens collected from a cohort of Italian patients whose diagnosis was performed by histology of the pleural biopsy. Our results point to the higher diagnostic utility of PE-SMRP than S-SMRP and provide information on SMRP levels in Italian patients with MPM for whom data are not yet available.
Materials and Methods
Patients and samples. This study included 102 patients who had developed PE. The patients underwent thoracentesis at the Division of Pneumology (Sarzana, La Spezia, Italy) between March 2008 and July 2011. PE and blood samples were collected from the same patients simultaneously. Thoracoscopy was performed in a fully-equipped operating theatre, under conscious sedation (i.v. propofol) (9). For each patient, a minimum of 10 parietal pleural biopsies were taken. The diagnosis was made for all patients by examination of hematoxilin and eosin stained biopsy sections combined with immunohistochemistry. The patients were followed-up at regular intervals for up to 24 months.
The study protocol was approved by the local Ethics Committee (approval number 57/2008) and informed consent was obtained from all the patients.
Forty three out of 102 (42.2%) samples were from MPM (93.0% male, median age=73.5 years, range=61.9-88.9 years), 23/102 (22.5%) samples were from different MTS (43.5% male, median age=71.5 years, range=43.1-85.5 years) and 36/102 (35.3%) samples were from different BNG (83.3% male, median age=77.4 years, range=46.1-85.5 years).
Histology and immunohistochemistry. Histology and immunohistochemistry were assessed by standard protocols used in the Division of Histopathology and Cytopathology (La Spezia, Italy). To perform immunohistochemistry, 5-μm thick paraffin sections were mounted on slides and deparaffinized. Antigens were localized by means of a Ventana Medical System/view™ DAB detection Kit (Ventana Medical Systems, S.A. Strasbourg, France) programmed for antigen retrieval. The immunostaining was performed using an automated immunostainer, PathVision (Ventana Medical Systems). Strong reactivity for calretinin (CONFIRM rabbit monoclonal primary antibody to calretinin, clone SP65) and cytokeratin 5/6 (mouse monoclonal primary antibody to cytokeratin 5/6, clone D5/16B4,) associated with negative reactivity for carcinoembryonic antigen (CEA) (mouse primary antibody for CEA, clone TF3H8-1), epithelial membrane antigen (EMA) (CONFIRM mouse monoclonal primary antibody to EMA, clone E-29) and thyroid transcription factor-1 (TTF-1)(CONFIRM mouse monoclonal antibody to TTF-1, clone 8G7G3/1) (all from Ventana Medical Systems) is considered to be supportive of the diagnosis of MPM.
Soluble mesothelin-related peptide (SMRP) levels in pleural effusion and serum. SMRP levels were detected by the MesoMark ELISA assay. All samples were tested in duplicate.
SMRP detection assay. Aliquots from both PE and serum were centrifuged (1500 ×g for 10 min at 4°C) and the supernatant was stored at −20°C until the SMRP analysis was performed. SMRP levels were measured by MesoMark Enzyme-linked immunosorbent assay (ELISA) kit (Cis-Bio International Gif/Yvette, France) according to the manufacturers' instructions. All PE and serum samples were tested in duplicate.
Statistical analyses. The diagnostic performance of SMRP was estimated through the receiver operating characteristic (ROC) analysis and the area under the ROC curve (AUC) was used as a measure of the accuracy of patient classification. The Mann Whitney test was applied to assess whether each AUC was statistically greater than 0.50 (level of non-discrimination or chance line). In addition, the exact binomial standard error of AUC was used to compute corresponding 95% confidence interval (95% CI) (31). On the basis of the ROC analysis, the optimal SMRP cut-off point of discrimination between the study subgroups (test-positive vs. test-negative patients) was also determined using the Youden index, which reflects the joint maximum values of sensitivity and specificity. Finally, in order to provide a measure of association between study biomarker and disease status, the diagnostic odds ratio (DOR) and corresponding 95% CI were also calculated (32).
All statistical tests were two-tailed and a p-value<0.05 was considered statistically significant. All statistical analyses were performed using Stata (StataCorp. Stata Statistical Software, release 11.2; Stata Corporation, College Station, TX, USA).
Results
Comparison of SMRP levels in PE and serum. An ELISA assay for SMRP detection was carried out in PE and serum from 43 patients with MPM, 23 patients with MTS and 36 patients with BNG.
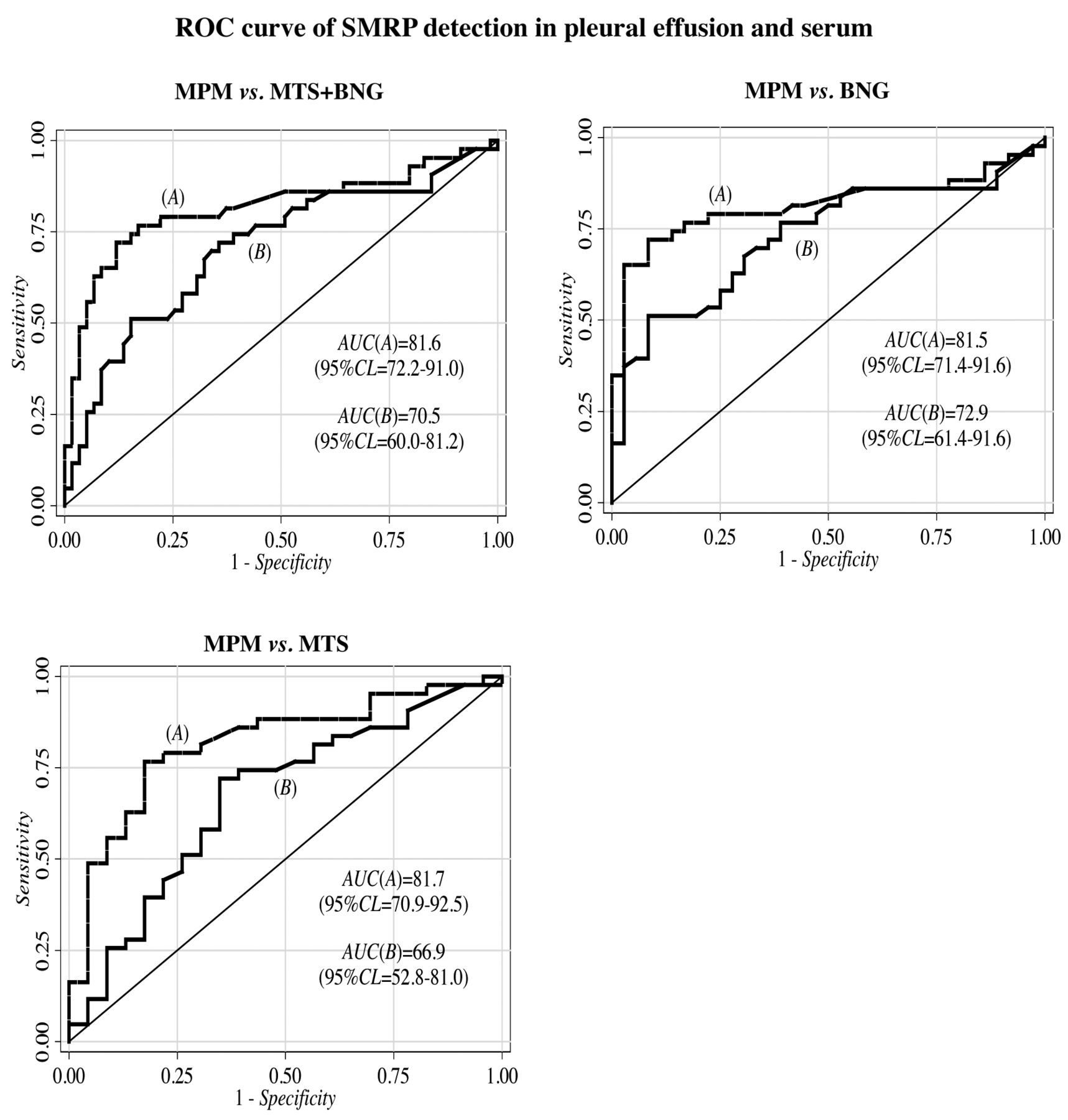
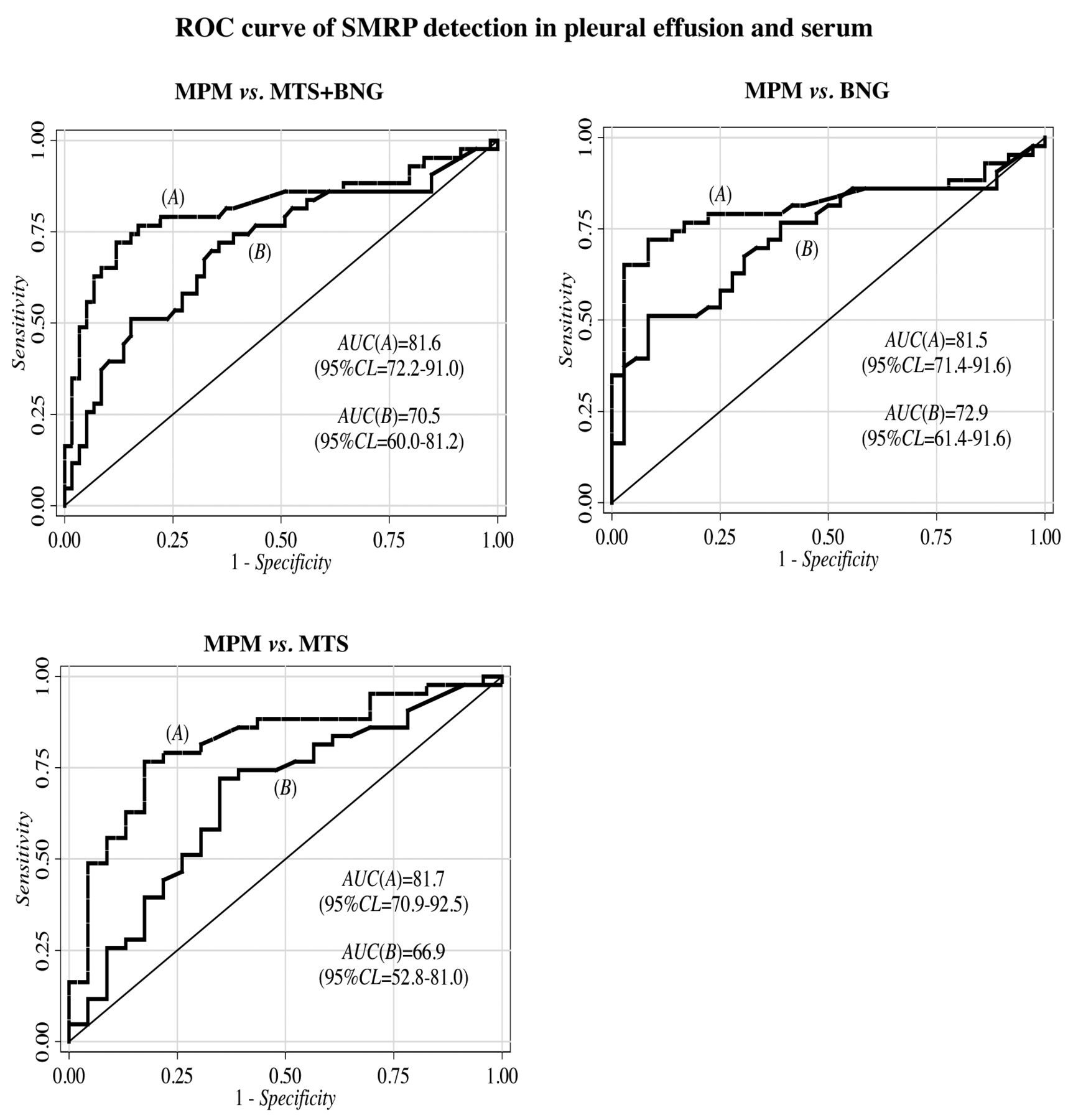
Diagnostic performance estimated through the ROC curve analysis of pleural effusion-SMRP (A) and serum-SMRP (B) for malignant mesothelioma (MPM) vs. other cancer metastasis (MTS) and benign disease (BNG) (upper left panel), malignant mesotheliama vs. benign disease (upper right panel) and malignant mesotheliama vs. other cancer metastasis (lower panel). SMRP levels were detected by the MesoMark ELISA assay. The cut-off values were 12.70 nM and 1.08 nM for pleural effusion-SRMP and for serum-SMRP, respectively. All samples were tested in duplicate. AUC: Area under the ROC curve; 95% CI: 95% confidence interval.
Patients with MPM were found to have significantly higher PE-SMRP levels than S-SMRP levels. The SMRP levels in MPM were significantly higher than in non-MPM (i.e. MTS+BNG) patients and in both MTS and BNG, compared separately (Table I).
Comparison of diagnostic performance of SMRP detection in PE and serum. We assessed the diagnostic accuracy of SMRP detection by using the ROC analysis. The results showed that PE-SMRP outperformed S-SMRP (Figure 1). In particular, when MPM and MTS+BNG patients were compared, AUC of 81.6% (95% CI=72.2-91.0%) and 70.5% (95% CI=60.0-81.2%) were estimated for PE-SMRP and S-SMRP, respectively (Figure 1, upper left panel). Similar results were found for MPM vs. BNG (Figure 1, upper right panel) and for MPM vs. MTS (Figure 1, lower panel). Using the maximum value of the Youden index, we found the optimal PE-SMRP and S-SMRP cut-off points of 12.70 nM and 1.08 nM, respectively. On the basis of such threshold values, PE-SMRP gave rise to a true-positive fraction of almost 70% which was much higher than that obtained by S-SMPR (Table II). Comparable values for Specificity were found for both PE-SMRP and S-SMRP markers (Table II).
Diagnostic performance of assays for soluble mesothelin-related peptide (SMRP) in matched pleural effusion and serum. SMRP levels were detected by the MesoMark ELISA assay. The cut-off values were 12.70 nM and 1.08 nM for pleural effusion- and for serum-SMRP, respectively. All samples were tested in duplicate.
In order to assess the overall discriminatory power (31) of each dichotomized study biomarker, the DOR values were calculated. For the comparison between MPM and MTS+BNG, DOR highlighted a better diagnostic performance of PE-SMRP (DOR=17.1 vs. DOR=4.8 (Table II). Similar results were found for both MPM vs. BNG and MPM vs. MTS (Table II).
Analysis of concordance of SMRP detection between PE and serum. We analyzed the concordance of positive (SMRP level>cut-off point) and negative classification by PE-SMRP and S-SMRP detection. We found concordant results in 78/102 (76.5%) specimens in total. In particular, out of the 43 cases of MPM, 19 (44.2%) were PE-positive/S-positive and 12 (27.9%) were PE-negative/S-negative (Table III).
On the contrary, S-SMRP and PE-SMRP showed discordant results in 24/102 (23.5%) of total specimens. In particular, 11 (25.6%) cases of MPM were PE-positive/S-negative and one (2.3%) MPM was PE-negative/S-positive (Table III).
SMRP detection in serum of patients with SMRP-negative PE and in PE of patients with SMRP-negative serum. We determined the reciprocal adjunct value of PE-SMRP and S-SMRP by taking into account their detection in SMRP-negative patients (Table IV). In other words, PE-SMRP diagnostic performance was assessed in 73 S-SMRP-negative individuals (23 MPM, 17 MTS, 33 BNG), and S-SMRP diagnostic performance was assessed in 65 PE-SMRP-negative individuals (13 MPM, 19 MTS, 33 BNG) (Table III). In this context, PE-SMRP detection maintained its clinical importance as, in MPM vs. MTS+BNG, it shows a sensitivity of 47.8% with specificity of 90.0% (Table IV). In contrast, S-SMRP showed a very low detection rate with sensitivity of 15.4% and specificity of 86.5% (Table IV).
Degree of concordance between soluble mesothelin-related peptide levels in pleural effusion and serum. SMRP levels were detected by the MesoMark ELISA assay. The cut-off values were 12.70 nM and 1.08 nM for pleural effusion- and for serum-SMRP, respectively. All samples were tested in duplicate.
Diagnostic performance of soluble mesothelin-related peptide (SMRP) detection in pleural effusion of patients with SMRP-negative serum and in serum of patients with SRMP-negative pleural effusion. SMRP levels were detected by the MesoMark ELISA assay. The cut-off values were 12.70 nM and 1.08 nM for pleural effusion- and for serum-SMRP, respectively. All samples were tested in duplicate.
Similar results were found for both MPM vs. BNG and MPM vs. MTS (Table IV).
In addition, in this context, the DOR values (DOR=8.3 vs. 1.2) pointed to PE-SMRP being a better diagnostic biomarker, although the study subgroups were not made up of the same patients (Table IV). Similar results were also found when BNG and MTS were considered separately (Table IV).
Discussion
The city of La Spezia has a history of industrial activities including harbouring, shipbuilding, shipyards, petrochemical plants and oil refineries. As a consequence, chronic exposure to industrial hazards, such as asbestos, is particularly high in this area. It has been pointed out that such an exposure is the cause of the increased frequency of MPM and it has been estimated that this increase will continue for several years (5).
In a previous study analysing the value of PE-SMRP detection, we concluded that this test can help in the diagnosis of MPM and may be incorporated into clinical practice (30). Herein, we carried out a comparative analysis of the diagnostic performance of PE-SMRP and S-SMRP detection.
In this study, performed on Italian patients, we confirmed previous reports from others showing that, for both PE and serum, the levels of SMRP were significantly higher in MPM as compared to non-MPM specimens, suggesting that both tests may be of assistance in MPM diagnosis (25-29).
We also confirmed that in MPM patients, SMRP levels were significantly higher in PE as compared to serum (median: 28.20 nM vs. 1.37 nM in our study) (25-29). A possible explanation for the higher value of PE-SMRP compared to S-SMRP is that mesothelin is a cell surface protein produced locally and released directly into the pleural cavity, as previously suggested by Davies et al. (26).
It is essential to point out that in the comparison of the diagnostic performance of two or more biomarkers, it is important to select the optimal cut-off point useful for classifying the study subjects. This selection can be driven by the purpose for which the diagnostic test is used. In fact, depending on the target pathology, it might be preferable to minimize the false-positive fraction (100–Specificity), in some cases, or the false-negative fraction (100–Sensitivity), in other cases. In the present study, we decided arbitrarily to use the SMRP threshold corresponding to the highest estimate of the Youden index (=Sensitivity+Specificity–100). In practice, the statistical criterion used here was based on the joint maximum values of Sensitivity and Specificity. As a result, the optimal thresholds were 12.70 nM and 1.08 nM for PE-SMRP and S-SMRP, respectively.
At these cut-off levels, we found that PE-SMRP showed better diagnostic performance parameters than S-SMRP (e.g. MPM vs. MTS+BNG: AUC=81.6% vs. 70.5%; Se=69.8% vs. 46.5%; Sp=88.1% vs. 84.7%; DOR=17.1 vs. 4.8). Thus, we may assert that PE-SMRP evaluation is more clinically useful than S-SMRP in establishing the diagnosis of MPM. Moreover, in patients with MPM, we found 12 specimens (28%) in which PE-SMRP and S-SMRP had discordant results. Eleven out of those specimens were PE-positive/S-negative, whereas only one was PE-negative/S-positive supporting the higher diagnostic value of PE-SMRP compared to S-SMRP detection. The higher clinical significance of PE-SMRP was also confirmed by the observation that in S-SMRP-negative cases, PE-SMRP maintained an acceptable diagnostic performance (Sensitivity approximately 47% and Specificity of 90%) and maintained high statistical correlation between SMRP and disease status (DOR=8.3, p-value=0.001). In contrast, in PE-SMRP-negative cases, S-SMRP had lower sensitivity (~15%) and its correlation with disease status was not statistically significant (DOR=1.2; p-value=0.858).
SMRP-positive specimens in MTS and BNG were found for both PE and serum. This is in accordance with previous report (14) showing that mesothelin may be found expressed at mRNA and protein levels in various tumours and on the surface of normal mesothelial cells. However, among the three PE-positive cases in the BNG group, one patient with pneumonia (PE-SMRP=16.5 nM) developed a myelodysplastic syndrome 24 months later and one patient with tuberculosis (PE-SMRP=16.6 nM) developed lung squamous cell carcinoma 22 months later. The other patient (PE-SMRP=51.4 nM) did not show any evidence of neoplasia 24 months later. In contrast, of the three S-SMRP-positive cases observed in the BNG patients group (two were tuberculosis and one pneumonia) none has, so far, shown malignancy. Thus, despite the very low number of patients analyzed in our study, these results suggest that only PE-SMRP positivity might have a prognostic significance.
In BNG, the concordance rate between matched PE and serum samples was about 83% but we did not find any double-positive cases. Simultaneous detection of PE-SMRP and S-SMRP remains restricted to the tumour (in our study, 19 MPM and two MTS) and this finding, if confirmed in further studies, may also be important for clinical diagnosis.
In conclusion, we showed that matched PE-SMRP and S-SMRP at the cut-off points of 12.70 nM and 1.08 nM, respectively, may help clinicians in the diagnosis of MPM but we confirm that the diagnostic accuracy of PE-SMRP is superior to that of S-SMRP (27). Thus, detection of PE-SMRP appears to be more informative than S-SMRP and it can better indicate the need for proceeding with an invasive investigation for the definitive diagnosis of MPM.
However, MPM is a rare malignancy consequently, it is difficult to collect specimens from large cohorts of patients with MPM. As our findings were obtained in a limited number of patients, to estimate the actual contribution of PE-SMRP and S-SMRP to the choice of thoracoscopy, further investigation is definitely required.
Acknowledgements
This work was supported by a grant from Ricerca Sanitaria Regione Liguria 2009 and from AIL (Sez, Francesca Lanzone) La Spezia, Italy. The Authors thank A. Camaiora, V. Balestracci, R. Tome and L. Lombardi for collecting the PE samples, the doctors and staff of the Pneumology Division (San Bartolomeo Hospital, Sarzana), the Histopathology and Cytopathology Division and the Clinical Pathology Division (Sant'Andrea Hospital, La Spezia). In addition, we thank Dr. B. Bacigalupo and Dr. A. Vigani for contributing to mesothelioma diagnosis and Dr. G. Leto for critically reading the manuscript.
- Received April 8, 2013.
- Revision received April 24, 2013.
- Accepted April 25, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical utility of diagnostic biomarkers in malignant pleural mesothelioma: a systematic review and meta-analysis
- Comparison of the Diagnostic Performance of Fibulin-3 and Mesothelin in Patients with Pleural Effusions from Malignant Mesothelioma
- Mesothelin in Serum and Pleural Effusion in the Diagnosis of Malignant Pleural Mesothelioma with Non-positive Cytology
- Diagnostic values of soluble mesothelin-related peptides for malignant pleural mesothelioma: updated meta-analysis