


Abstract
Aim: To detect telomerase reverse transcriptase (TERT) expression in tissue and metastatic and non-metastatic lymph node samples from patients with non-small cell lung cancer; to evaluate whether TERT expression is correlated with pathological and clinical features, and/or patient survival times; to determine differences between TERT expression in metastatic and non-metastatic lymph nodes. Patients and Methods: Tumor tissue samples from 17 patients with squamous cell lung cancer and 11 patients with adenocarcinoma diagnosed between 2003 and 2004 were included in this study. All patients were diagnosed at our hospital and had samples stored in the pathology archive. Additionally, dissected lymph node samples, with and without metastases, were studied. Telomerase Gene Tex, Inc, Irvine, CA USA (TERT (2C4) antibody), Universal Kit (Lab Vision, Newmarket, UK) were used for immunohistochemical staining. Statistical analyses were performed using SPSS 17.0 statistical software. Results: TERT was positive in 18/28 of the samples, regardless of the histological tumor type. There was no significant correlation between TERT expression in lymph nodes with metastasis and clinical stage, histological type, tumor differentiation, or survival time. Conclusion: TERT expression may be used as a target for therapy. It may also be helpful in predicting metastasis but not in predicting survival time.
Telomerase is a ribonucleoprotein complex mainly composed of a reverse transcriptase catalytic subunit (telomerase reverse transcriptase gene) which copies a template region of its RNA subunit to the end of the telomere. Human telomeres function as a protective structure capping the ends of chromosomes. Dysfunction of telomeres plays an important role in cancer initiation and progression. Expression of human telomerase catalytic component (hTERT) is known to be elevated in cancer. Thus, hTERT is potentially useful as a diagnostic marker of cancer. Immunohistochemistry allows detection of hTERT protein expression at the individual cell level in human tissues (1-3). hTERT immunostaining in fixed tissues was concordant with telomerase activity and hTERT mRNA expression in corresponding non-fixed samples (1).
The determination of the molecular pathways implicated in non-small cell lung cancer (NSCLC) etiology and pathogenesis has already led to the identification of potential new therapeutic targets. Moreover, elucidation of the mechanisms of cytotoxic or molecular drug interactions has resulted in identification of novel biological markers within cancer cells which may be associated with individual patient chemosensitivity, thus allowing the application of chemotherapy or molecular targeted therapy for patients who are most likely to benefit from it (4, 5).
Telomerase activity is considered indispensable for tumor immortalization and growth. Telomerase expression has been directly linked to the ability of tumor cells to replicate indefinitely, and the inhibition of telomerase in tumor cells has been shown to lead to cell death. hTERT, the rate-limiting subunit of the telomerase complex, is therefore an attractive target for cancer vaccination (6-9).
Several studies using animal models and human NSCLC tissues have reported that TERT mRNA and TERT protein are overexpressed in lung cancer biopsies compared with normal lung tissues (10). Telomerase holds great promise as a biomarker for early detection of cancer and metastasis and monitoring, and has considerable potential as the basis for developing new anticancer therapies. Detection of hTERT might have prognostic value for patients with early-stage lung cancer.
We aimed at detecting TERT expression in the resected tissue samples and metastatic and non-metastatic lymph node samples from patients with non-small cell lung cancer. We evaluated whether TERT expression correlated with pathological and clinical features, and/or patient survival times. We also investigated whether differences exist between TERT expression in metastatic and non-metastatic lymph nodes.
Patients and Methods
Tissue samples of 17 patients with squamous cell lung cancer and 11 patients with adenocarcinoma diagnosed in 2003 and 2004 were included in this study. All patients were diagnosed at our hospital and had samples stored in the pathology archive. TNM patient evaluations were performed according to criteria indicated in the staging procedures of the International Association for the Study of Lung Cancer (IASLC) (11). Additionally, dissected lymph node samples, with and without metastases, from 14 of the patients with squamous cell lung cancer and 11 with adenocarcinoma were included in this study. Telomerase was immunohistochemically examined in a total of 78 samples (28 samples from resected masses and 50 from dissected lymph nodes). This retrospective study was conducted in 2007 and 2008. Since this was a retrospective study, our hospital's Institutional Review Board Committee waived ethics approval. The scientific study committee of the Yedikule Teaching Hospital for Chest Diseases and Thoracic Surgery reviewed and approved the database. The study was completed in 2008. Patient survival times were individually provided by family members by telephone.
Immunohistochemical analysis of telomerase activity. TERT (2C4) antibody (Telomerase Gene Tex, Inc., Irvine, CA, USA) and a Universal Kit (Lab Vision, Newmarket, UK) were used for immunohistochemical staining. From the resected lung tissue samples, 3-μm-thick each of tumor sections were prepared. The paraffinized blocks from lymph node samples, with and without metastases, were similarly cut into 3-μm-thick sections. Immunohistochemical assays were performed using the avidin-biotin peroxidase complex method. Hematoxylin was used for contrast staining. Respiratory epithelium from lung tissue and the bronchus wall were used as positive controls. Additionally, salivary gland tissue was used as an internal control.
Cells with nuclear staining were considered positive for TERT expression. Tumors in which 5% or fewer cells had nuclear staining were evaluated as negative for TERT, while tumors in which more than 5% had nuclear staining were considered positive. Besides the nuclear staining, the distribution of cytoplasmic particles attracted attention in the course of staining. Tumors with more than 50% staining of the tissue were accepted as being positive for TERT, while tissues with almost no reaction to the staining were considered negative for TERT. A more intense positivity occurred in the follicle centers of the lymph nodes; less intensity was observed in the parafollicular cells. Both tumor and lymphoid cells in metastatic lymph nodes displayed variable reactions in telomerase-positive samples. While lymphoid cells only showed positive reactions in non-metastatic lymph node samples, positive reactions were not found in tumor cells (12).
Statistical analysis. Normal distribution of data was assessed using the Shapiro-Wilk test and histograms. The values are presented as median (IQR), frequency and percentage. Nominal variable values were evaluated using the chi-square test, and Fisher's exact test. Quantitative variables were assessed using the Mann-Whitney U-test. Survival rates within groups were calculated using the Kaplan Meier method. Survival curves for patient with telomerase-positive and -negative tumors were estimated using the Kaplan Meier method, and differences between these survival curves were analyzed using the generalized log-rank test. Analyses were performed using SPSS 17.0 statistical software. Results with p-values less than 0.05 were considered statistically significant.
Results
Of the patients with lung cancer, 61.8% had squamous cell carcinoma (17/28) and 38.2% had adenocarcinoma (11/28). TNM classifications were as follows: 53.6% stage 1 (n=15), 42.9% stage 2 (n=12), and 3.6% stage 3 (n=1). No differences in the pathological features of resected tissue samples, such as tumor localization (lobe, bronchus, parietal and visceral pleural involvement), invasion of surgical borders, tumor differentiation, and microscopic features (stromal desmoplasia, stromal lymphocyte, perineural involvement, blood vessel invasion), were found between squamous cell carcinoma and adenocarcinoma of the lung (p>0.05). Additionally, TERT expression was not significantly different for different histological tumor types, such as lymph nodes and resected tumor tissue. Patient survival times were also not significantly different (Table I). Only lobe bronchus involvement was higher among patients with squamous lung cancer than among those with adenocarcinoma of the lung (p=0.002).
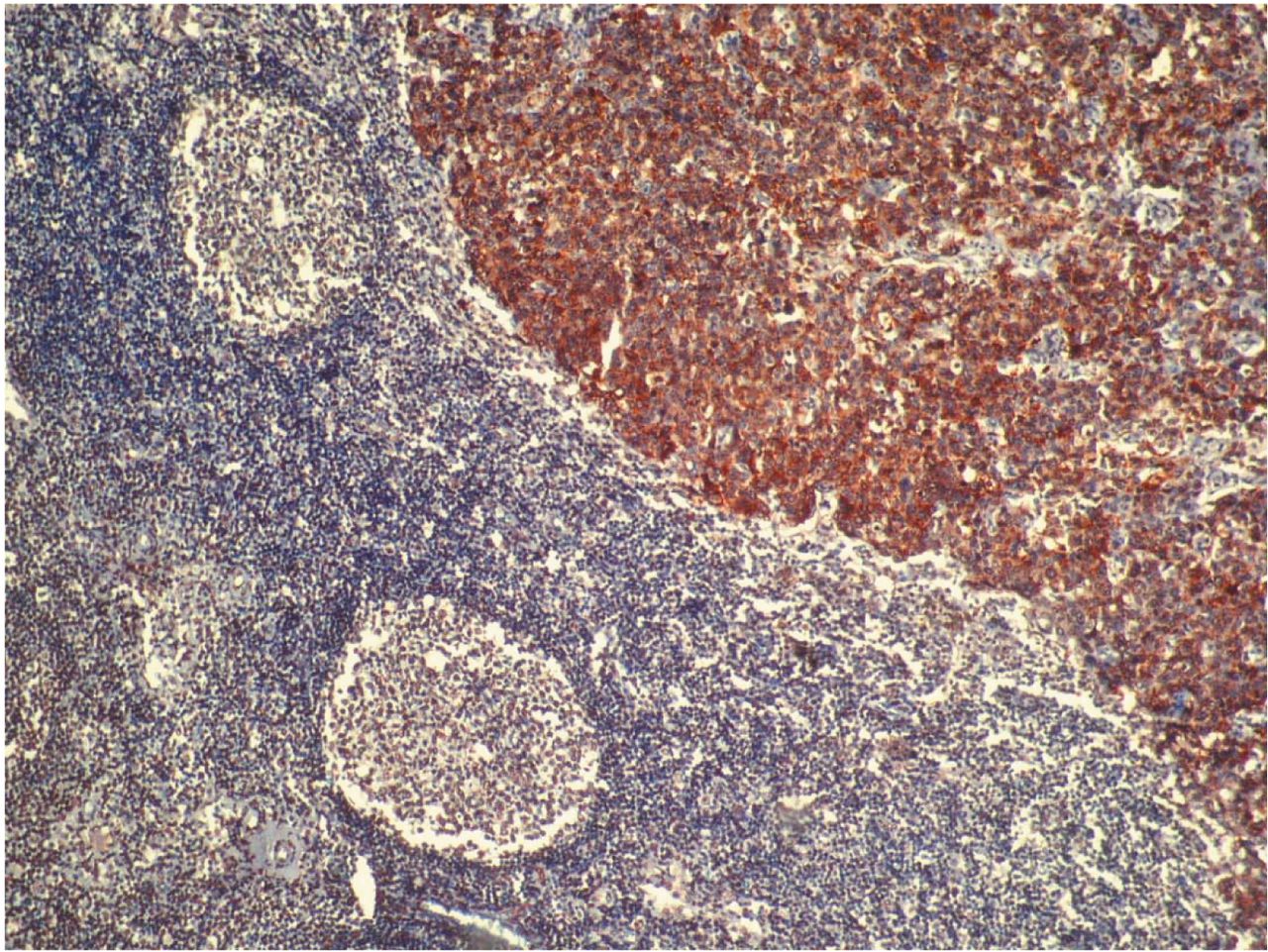
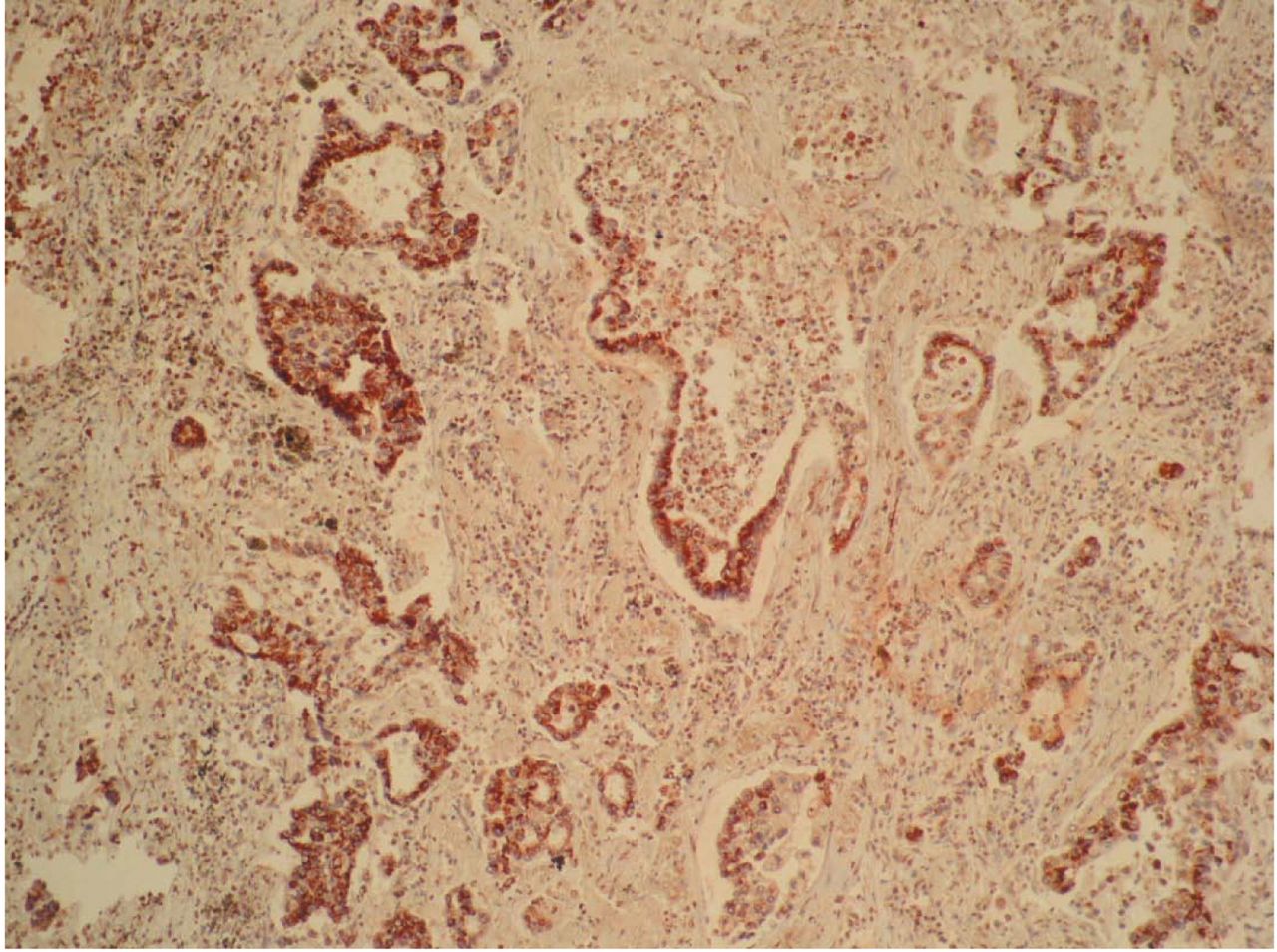
TERT expression was positive in 70.6% of the patients with squamous cell carcinoma (n=12) and in 54.5% with adenocarcinoma (n=6) (Figures 1 and 2). TERT was positive in 64.2% (n=18) of the patients, regardless of the histological tumor type. When TERT expression was compared between patients, the mean age of TERT-positive patients was 57.33±7.50 years and that of TERT-negative patients was 53.80±10.79 years. There was no statistical difference in mean age between the two groups. Furthermore, no differences in clinical stage, patient survival time, tumor size, localization, resection border distance, cytological type, or other pathological features of resected tissue samples were found between the TERT-positive and TERT-negative patients (p>0.05; Table II). The presence of TERT expression in resected tissue samples was not correlated with these parameters.
Features according to histological tumor type.
TERT expression was positive in dissected lymph nodes in 9/17 patients with squamous cell carcinoma (Figure 3) and 5/11 patients with adenocarcinoma (Table I). The rate of concurrent TERT-positive resected tumor tissue and lymph nodes was lower in the patients with adenocarcinoma than in those with squamous cell carcinoma (p=0.05, Table I). TERT may be an important marker for indicating metastasis in patients with squamous cell lung cancer.
When this retrospective study was conducted, 67.8% of our patients were dead (n=19) and 32.2% were alive. The patients whose tissues were included in this study had a mean survival time of 37.47±4.28 months (Median 33.0 months, IQR: 27.81-38.18 months). There was no significant difference between the survival times associated with different histological tumor types. The mean survival time was 38.57±5.69 months for the patients with squamous cell carcinoma and 33.27±5.68 months for the patients with adenocarcinoma (p=0.311, Table II). Similarly, no relationship was observed between survival time and TERT positivity or negativity. Of the patients with lymph node metastases, 9/17 with squamous cell carcinoma and 5/11 with adenocarcinoma had TERT-positive lymph nodes. However, there was no TERT receptor expression in the lymph nodes without metastasis. Fifty-six percent (14/25) of the patients with NSCLC had TERT positive lymph nodes, regardless of the histological tumor type. There was no statistically significant relationship between TERT expression in lymph nodes with metastasis and clinical stage, histological type, tumor differentiation, or survival time. Additionally, TERT positivity was not correlated with microscopic tumor features (Tables II and III). However, TERT positivity was higher in tumors that had central and lobe bronchus involvement (p=0.021 for both).
Discussion
Telomerase activity and hTERT expression were found in 67-85% and 48-95% of lung tumors, respectively, in several studies (13, 14). This study's results support previous findings. TERT was detected in 18 out of 28 (64.2%) NSCLC tissue specimens (70.6% of squamous cell carcinoma specimens, 54.5% of adenocarcinoma specimens).

Telomerase immunopositivity in squamous cell lung cancer (×200).
Comparison of non-small cell lung cancer features according to expression of telomerase reverse transcriptase (TERT).

Telomerase immunopositivity in adenocarcinoma of the lung (×100).
Telomerase-positive metastatic lymph node with squamous cell lung cancer (×100).
Lymph node features according to telomerase reverse transcriptase (TERT) expression in the lymph nodes.
Lantuejoul and co-workers reported that hTERT expression was significantly lower in adenocarcinoma than in squamous cell carcinoma (10). Wu et al. demonstrated that neither telomerase activity nor hTERT expression in NSCLC was correlated with clinicopathological characteristics, such as grade, tumor stage, tumor type, or TNM values (15). In our study, there was similarly no significant correlation between the expression of TERT and other parameters, such as age, clinical stage, tumor size, resection border distance, survival time, type of surgery, tumor differentiation, or microscopic features of the tumor.
In the present study, the coincidence of TERT expression in both tumor tissue and metastatic lymph nodes was higher for squamous cell carcinoma than adenocarcinoma. There was no TERT expression in the non-metastatic lymph nodes. The rate of TERT expression was 56% in lymph nodes of NSCLC patients, regardless of cytological type.
These results suggest that TERT may be a promising biomarker for predicting micro-metastases, especially in patients with squamous cell carcinoma. Wallace et al. investigated micrometastatic disease in mediastinal lymph nodes of patients with NSCLC using endoscopic ultrasound-guided fine-needle aspiration. Detection of these micrometastases using molecular techniques, such as immunohistochemistry or reverse transcriptase-PCR has been shown to improve the detection of metastatic epithelial cells in the lymph nodes and bone marrow of patients with lung carcinoma (16, 17).
In one study, analysis of 136 primary tumors from patients with NSCLC identified telomerase activity in 78.6% compared with 4% in adjacent normal tissues. Hiyama et al. first observed a high level of telomerase activity in primary tumors and corresponding metastatic lesions (18). Wallace et al. determined that one-third of pathologically negative lymph nodes express telomerase (16).We determined that none of the pathologically negative lymph nodes expressed telomerase. Wallace et al. found that 63% of cytologically positive lymph nodes did have evidence of expression. We found similar results for squamous cell carcinoma. Wallace et al. failed to evaluate the relevance of clinical features and survival time and, therefore, could not compare histological types. TERT was highly specific (no expression was found in cytologically non-metastatic lymph nodes) and had limited sensitivity.
When we evaluated the relevance of clinical features, no correlation was found between TERT expression in lymph nodes with metastasis and any of the parameters, including clinical stage, differentiation, survival time, and microscopic features of the tumor. However, TERT positivity was statistically higher in tumors with lobe bronchus and central involvement. As these involvement types are features of squamous cell carcinoma, we hypothesize that the higher TERT positivity was due to the presence of squamous cell lung cancer, rather than involvement type.
For patients with NSCLC, the prognostic value of telomerase activity remains unclear. While most studies have associated overexpression with poor prognosis, others have failed to demonstrate any prognostic impact of overexpression in NSCLC. Of our patients, 67.8% died during the course of the study. There was no statistical difference in survival time for patients with and without TERT expression. Metzger et al. showed that high TERT mRNA expression was associated with improved five-year survival, while telomerase activity was not associated with survival, stage, pT and pN categories, histological type, or grading (19). Conversely, in our study, expression patterns were distinct among histopathological subtypes of NSCLC, and low hTERT expression was significantly associated with squamous cell histology.
In a study conducted by Komiya et al., patients with hTERT expression had shorter survival times than those without hTERT expression. Multivariate analysis showed that hTERT expression was an independent negative prognostic factor. These results suggest that expression of hTERT may be an independent prognostic factor for patients with NSCLC (20). Van den Berg et al. showed that TERT mRNA levels in tumor tissue had no prognostic value for patients with early-stage lung cancer. However, detection of hTERT mRNA expression in tumor-distant normal lung tissue may indicate an increased risk of progressive disease (21). Telomeres and telomerase are targets for anticancer drug development, and specific inhibitors are currently under clinical investigation. Several phase I studies of hTERT immunotherapy have been completed in patients with breast, prostate, lung, and other types of cancer, and clinical and immunological results are encouraging (22, 23).
In conclusion, we identified TERT expression in NSCLC tissue samples and lymph nodes with metastasis using immunohistochemistry, and there was no expression in non-metastatic lymph nodes. We did not demonstrate a correlation between TERT expression in NSCLC and clinicopathological characteristics, such as tumor type, clinical stage, grade, differentiation, microscopic tumor features, and survival time. TERT may be useful in identifying a telomerase-targeted therapy which can prevent tumor growth. TERT may also be helpful in predicting metastasis but not in predicting survival time.
- Received April 12, 2013.
- Revision received May 17, 2013.
- Accepted May 20, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.