


Abstract
Background/Aim: The purpose of this study was to analyze the incidence and survival in all sarcomas based on year of diagnosis, anatomical site, grade, stage, and age of patient. Materials and Methods: The Surveillance, Epidemiology, and End Results (SEER) database was queried for the years 1975 to 2009 and included 18 registries across the United States representing 28% of the national population. Incidence rates for 2005-2009 and five-year survival rates for 2000-2004 were calculated for all categories of sarcomas for multiple key variables. Results: Sarcomas are rare, with most occurring in fewer than 5 per 1,000,000. The most common were leiomyosarcoma, Kaposi sarcoma, malignant fibrous histiocytoma, liposarcoma and fibrosarcoma. Survival was poorer for those with more advanced grade, stage, and age at-diagnosis. Most sarcomas affected the lower extremities, followed by the upper extremities and torso. Pelvic tumors were less common, but generally led lower survival than lesions of the extremities. Conclusion: The epidemiology of sarcomas varies widely by type and other variables. Incidence and survival data provide valuable information for patient counseling and may have implications in understanding the natural history of sarcoma. This study represents the most recently updated comprehensive report on all types of sarcomas in the United States.
Musculoskeletal sarcomas are a heterogenous group of rare malignant tumors involving bone and soft tissue. Sarcomas represent a small proportion of overall malignancies in most studies, varying from 0.7-1% for adult soft tissue, 0.2% for adult bone, 4-8% for pediatric soft tissue, and 5% for pediatric bone lesions (1-3). Because of the relative rarity of sarcomas and musculoskeletal tumors compared to carcinoma, lymphoma, leukemia and cancer affecting other sites, they are frequently lumped homogenously together in large-scale epidemiological reports. Useful data are difficult to extract and most statistics on individual types of sarcomas are based on retrospective series from large academic centers (4-6) or registries from smaller populations (7, 8).
The purpose of this study was to analyze the incidence and survival for all types of musculoskeletal sarcomas in the United States based on year of diagnosis, anatomic site, grade, stage, and age of patient. The Authors were unaware of any prior recent studies of similar nature and scope.
Materials and Methods
The National Cancer Institute's Surveillance, Epidemiology and End Results (SEER) program is the only comprehensive database in the U.S. that includes stage at time of diagnosis and patient survival data (9). For this study, incidence data between 1975 to 2009 (most recent year of complete data entry) were drawn from the original nine SEER registries consisting of the metropolitan areas of Atlanta, Detroit, San Francisco-Oakland, and Seattle-Puget Sound, and the states of Connecticut, Hawaii, Iowa, New Mexico, and Utah. These areas represent approximately 9.5% of the total U.S. population. Survival data were evaluated from SEER 18, which includes the additional registries of Los Angeles, San Jose-Monterey, rural and greater Georgia, Alaska, greater California, Kentucky, Louisiana, and New Jersey. These areas represent approximately 28% of the total U.S. population (9). SEER*Stat computer programming was used for survival, incidence over time, and most recent incidence. For survival data based on year of diagnosis, the years 1975 to 2004 (five-year lag time for five-year survival) were examined. For survival data based on site, age at-diagnosis, grade and stage, the years 2000 to 2004 were used in order to provide with the most recent data and to eliminate the likely effect of lower survival rates in earlier years. Although SEER was established in 1973, the first two years' data were believed to be less organized and therefore omitted from this study.
Incidence rates were age-adjusted based on the U.S. year 2000 standard population to account for the progressive aging of the U.S. population and generally higher incidence of tumors in elderly patients. Relative survival was calculated using an actuarial method to eliminate the rate of death attributable to other causes in a comparable cohort in the general population. The clinical staging scheme used was SEER historic stage A, which includes localized, in organ of origin, regardless of size; regional, extension into adjacent tissues or lymph nodes; and distant (metastasis). Tumors were divided histologically in SEER based on four grades: I, well-differentiated; II, moderate/intermediate differentiation; III, poorly differentiated; and IV, undifferentiated or anaplastic (9). Individual four-digit histology codes were grouped into major histological groups by two fellowship-trained orthopaedic oncologists (JLM, TJS). Age intervals included 0-4, 5-29, 30-59, and greater than 60 years. Anatomic groups were lower limb (bone, soft tissue, skin), upper limb including scapula (bone, soft tissue, skin), pelvis, spine, and trunk (retroperitoneum, ribs). Tumors of the extremities were further separated into those that affected long bones, short bones (of the hands and feet), and soft tissue.
Average annual, age-adjusted incidence rates, per 100,000 persons, for race/gender groups1 (case counts in parentheses).
Results
The five-year survival and incidences for each category of sarcomas are represented according to race and gender, grade and stage, anatomical site, and age at diagnosis (Tables I, II, III, IV and V). The overall changes in incidence over the past two and a half decades have been minor for common musculoskeletal maligancies, including Ewing sarcoma, liposarcoma, chondrosarcoma, synovial sarcoma, and osteosarcoma. The overall incidence of leiomyosarcomas has decreased (Figure 1).
Five-year relative survival probability according to grade and stage from cases diagnosed within the SEER Program, 2000-2004. - Denotes N=0 for time period; L/R/D, localized/regional/distant involvement; MFH, malignant fibrous histiocytomas; PNET, primitive/peripheral neuroectodermal tumor. Survival is rounded to nearest 1%. Incidence is based per 100,000.
The vast majority of categories of sarcomas had an incidence between 1 to 5 per 1,000,000. The most common were leiomyosarcomas, Kaposi sarcomas, malignant fibrous histiocytomas, liposarcomas and fibrosarcomas. Some sarcomas demonstrated higher incidences in certain populations such as leiomyosarcomas in white females, Kaposi sarcomas in black males, gastrointestinal in black males, chordoma in elderly adults, fibrosarcoma in middle-aged adults, and Ewing sarcoma in young adults. Survival was poorer for those with more advanced grade, stage, and age at diagnosis. The five-year survival from major musculoskeletal malignancies has risen since the mid-1970s approximately 5% to 20%, except for chondrosarcoma. Since the late 1980s, however, survival has remained relatively stable (Figure 2). Most sarcomas affected the lower extremities, followed by the upper extremities and torso. Pelvic tumors were less common, but generally led to lower survival compared to this of patients with lesions of the extremities.
Discussion
The epidemiology of sarcomas varies by type, and the incidence and survival are valuable information for patient counseling. This study represents the most recently updated comprehensive report on sarcomas in the U.S. In addition to providing data on the more common sarcomas, rarer malignancies have been included. The findings here reflect many of the results reported in narrower studies of individual sarcoma types.
Osteosarcomas had similar incidence rates in white and black males and females, but appeared to have a slightly lower incidence in Asians. This was a historically consistent trend (10). Osteosarcomas occurred in all age groups, with the 5-29 year age range having the highest incidence. This group had also the best five-year survival rate. Survival decreased with higher grade tumors and more advanced stage of disease. Patients with lesions of the extremities had better prognoses than these with pelvic or spinal lesions. These findings for osteosarcoma are similar to those of other reports (11, 12). A bi-modal age distribution, with a majority in the under-30 year category, is often described (1, 13), although others have found it to be a less pronounced peak (7, 14).
Ewing sarcoma was most common in white males, followed by white females. Consistent with prior literature (1, 13, 14), Ewing sarcoma was rarer in black individuals. Survival did not appear to vary significantly with the documented grade, but this should be expected since Ewing sarcoma is defined as high-grade (15) and variations in SEER grade are likely clerical. Those with grossly metastatic disease had fared worse than those with local disease or undetectable micrometastases, a consistent trend (16). Ewing sarcoma of the extremities led to higher survival than that of the pelvis or spine. Similar to other studies (1, 7, 13,14), the majority of affected patients were less than 29 years old and had a better prognosis than more elderly patients.
Five-year relative survival probability according to sarcoma type and anatomic region (n in parentheses) from cases diagnosed within the SEER Program, 2000-2004. MFH, malignant fibrous histiocytoma; PNET, primitive/peripheral neuroectodermal tumor; MPNST, malignant peripheral nerve sheath tumor; GIST, gastrointestinal stromal sarcoma; NOS, not otherwise specified. Survival is rounded to nearest 1%. Incidence is based per 100,000.
Chondrosarcoma had higher incidence rates in males than females in all races. Survival trends were consistent with those of other studies (17-23). It was more common with advancing age, and patients older than 60 years had lower survival rates. The survival rate dropped precipitously with more advanced tumor grades. Chondrosarcoma of the extremities had better prognosis than that of the pelvis or spine, and those with lesions of the short bones had the best survival.
Synovial sarcoma incidence did not vary significantly by gender, race, or age greater than five years. Traditionally, however, it is thought to be more common in adolescents and young adults (24). Survival decreases with higher grade and stage (25). Adults are known to have poorer outcomes than children with synovial sarcoma (26). Lesions of the lower extremities were most common, but those of the upper extremities had the best prognosis, followed by those of the lower extremities, then pelvic lesions.
Five-year relative survival probability according to age at-diagnosis (incidence rates per 100,000; total N in parentheses for 2005-2009) from cases diagnosed within the SEER Program, 2000-2004. MFH, malignant fibrous histiocytoma; PNET, primitive/peripheral neuroectodermal tumor; MPNST, malignant peripheral nerve sheath tumor; GIST, gastrointestinal stromal sarcoma; NOS, not otherwise specified. Survival is rounded to nearest 1%. Incidence is based per 100,000.
Liposarcoma was most common in white males and increased in incidence with advancing age. It is rare in the pediatric and adolescent population (27). Survival decreased with increasing grade, stage and age. Lesions of the extremities and pelvis had similar prognosis, but were distinctly higher than torso or retroperitoneal lesions (28).
Fibrosarcoma was most common in blacks, at nearly twice the incidence as whites or Asians. Most cases occurred in patients older than 30 years. Survival decreased with more advanced grade and stage, but the overall survival rate was excellent for lesions of the extremities and torso. Other studies have reported lower rates of survival from fibrosarcoma, but had confounding factors such as inclusion of all causes of death (29), or inclusion of patients prior to widespread use of adjuvant therapy (30).
Five-year relative survival probability for selected sarcomas according to anatomic grouping (n in parentheses) from cases diagnosed within the SEER Program, 2000-2004. MFH, malignant fibrous histiocytoma; PNET, primitive / peripheral neuroectodermal tumor. Survival is rounded to nearest 1%.
The trends in survival from Ewing sarcoma and osteosarcoma are consistent with other literature, with improvements mirroring the advent of effective chemotherapeutic agents (13). There has, however, been a plateau over the past two decades without new breakthroughs in therapeutic modalities. Chondrosarcoma is relatively chemoresistant and radioresistant, and has not changed in survival significantly, as it is primarily a surgical condition. Effective means to address micrometastases of chondrosarcoma have yet to be discovered. For soft-tissue sarcomas, although the ability to achieve limb-salvage surgery has improved and the general knowledge has advanced, overall survival has not increased. It has been suggested that risk stratification based on prognostic criteria, surgical techniques, perioperative management, and adjuvant therapy have reached the current limits of efficacy for extremity soft-tissue sarcomas (31). The limited changes in survival over time for liposarcoma and synovial sarcoma demonstrated here, support these conclusions.
Although some sources report a slightly increasing incidence of soft-tissue sarcomas, it has not been observed in all studies (8, 32). Interpretation may be confounded by under-reporting of malignancies, evolving diagnostic criteria, and temporal increases in certain subtypes such as AIDS-related Kaposi's sarcoma. The decrease in leiomyosarcomas may be due in part to re-classification of some gastric leiomyosarcomas as gastrointestinal stromal tumors (33). Similar to prior reports, the incidence trends for bone sarcoma have remained fairly steady (34, 35).
Some studies, however, have found changing incidences in certain groups. In Northern England, the incidence of osteosarcomas in patients younger than 40 years increased 2.5% per year between 1981 and 2002 (1). Paget's sarcoma of bone has decreased steadily, beginning even before the advent of effective treatment of Paget's disease (36). In the U.S., the incidence of osteosarcomas has decreased for whites, but increased for blacks and other races (10).
There are several limitations to this study. Firstly, survival and incidence rates for very rare types of sarcoma may have unreliable statistics due to a limited sample size. Nevertheless, the collection of patients represented by SEER is larger than most previously reported individual institution series. Secondly, changes in histological classifications such as malignant fibrous histiocytoma may affect incidence and survival rates. Comparison of tumors formerly known as malignant fibrous histiocytoma into the current category of high-grade pleomorphic sarcoma is difficult. Thirdly, further histological sub-typing and variable treatment modalities could reveal subtle differences in survival. However, it would be beyond the scope of a single article to examine the statistical nuances for each type of sarcoma. The purpose of this study was to provide a comparative template of all sarcomas, common and uncommon. Finally, the SEER grading system is not as widely used as the National Cancer Institute (37) or Federation Nationale des Centres de Lutte Contre le Cancer (French) (38) system. Unlike the Musculoskeletal Tumor Society staging system (39), which includes grade, compartment, and metastasis, the SEER, NCI and French systems are based on histological features. The SEER clinical stages for malignancies were also included in this study to help correlate with clinical behavior and the Musculoskeletal Tumor Society system.
These limitations highlight the importance of accurately reporting and detailed analysis of epidemiological data in understanding of the natural history and population-wide behavior of various malignancies. As new therapeutic modalities are instituted and different causative theories are postulated, historical survival rates and incidence levels can be used to judge their efficacy and validity.

Changes in incidence per 100,000 persons, 1973-2009. The incidence of primary bone sarcomas and of synovial sarcoma and liposarcoma has remained fairly steady for the past three decades. The overall incidence of leiomyosarcoma has decreased since the 1970s.
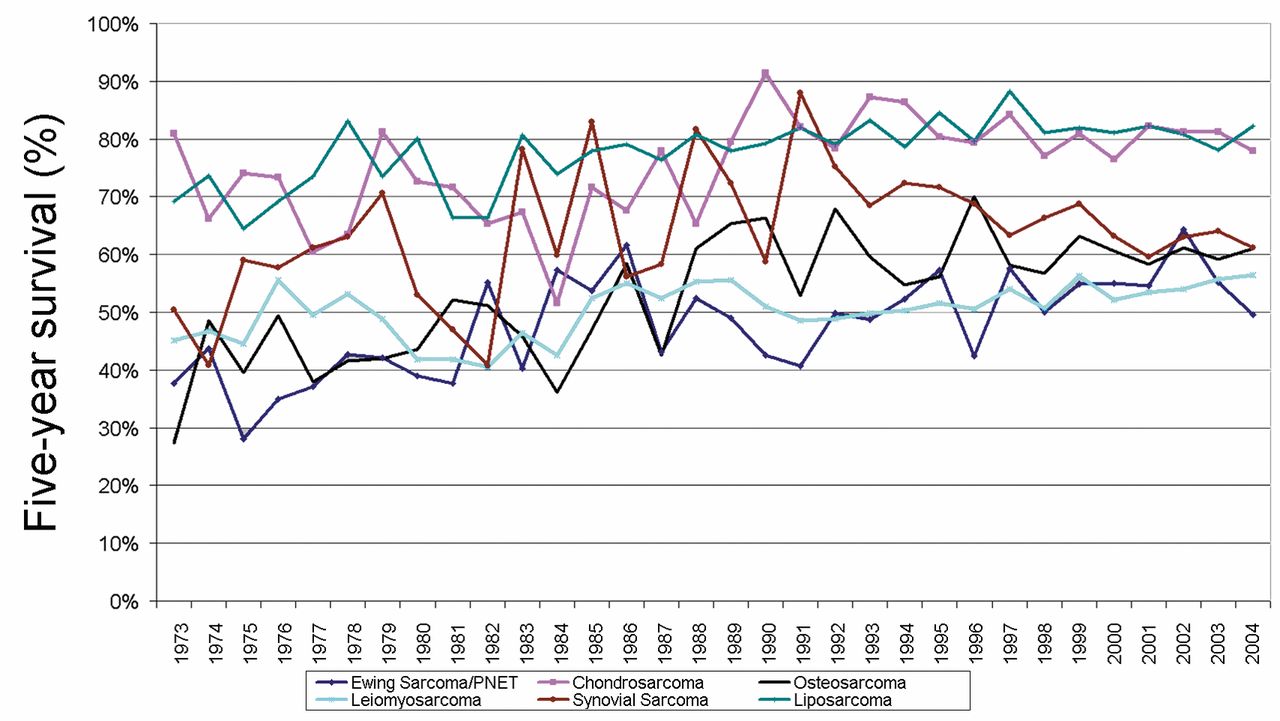
Changes in five-year survival rates, 1973-2004. The survival rates for patients with osteosarcoma and Ewing sarcoma have increased since the mid-1970s, but appear to have reached a plateau in the past two decades. The survival for those chondrosarcoma has not changed over time. The survival for those with some of the more common musculoskeletal soft tissue sarcomas have improved slightly.
- Received April 2, 2013.
- Revision received April 25, 2013.
- Accepted April 29, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- SHARPIN enhances ferroptosis in synovial sarcoma cells via NF-{kappa}B- and PRMT5-mediated PGC1{alpha} reduction
- Metastatic malignant peripheral nerve sheath tumour in a patient with neurofibromatosis 1 and review of contemporary systemic treatments
- Outcome of Scapular Ewing Sarcoma
- Racial and Ethnic Differences in Sarcoma Incidence Are Independent of Census-Tract Socioeconomic Status
- The Immunosuppressive Niche of Soft-Tissue Sarcomas is Sustained by Tumor-Associated Macrophages and Characterized by Intratumoral Tertiary Lymphoid Structures
- Safe and Effective Sarcoma Therapy through Bispecific Targeting of EGFR and uPAR
- Managing Liposarcomas: Cutting Through the Fat
- Vitamin D Levels and Dietary Intake Among Patients with Benign Soft Tissue Tumors and Sarcomas
- Malignant Peripheral Nerve Sheath Tumors