


Abstract
Background: Protruding adenomas in the Barrett's mucosa (BM) are very rare. Out of the 22 adenomas evolving in BM recorded in the literature, 21 were tubular and the remaining one, villous. Case Report: We describe a case of traditional serrated adenoma (TSA) in BM. The TSA displayed hyperplastic fronds with saw-like indentations lined with low-grade dysplasia. In addition, dysplastic cells and atypical mitoses reaching the luminal epithelial border (high-grade dysplasia) were observed in the lower part of the TSA. Cell proliferation (Ki67) mostly occurred at the bottom of the dysplastic serrations. In non-dysplastic subjacent glands with intestinal metaplasia, goblet cells contained sialomucins (alcian blue pH 2.5) and mucopolysaccharides (periodic acid Schiff). The TSA was found at the border of an invasive adenocarcinoma. Conclusion: The review of the literature indicates that this is first case of TSA in the BM ever reported. It remains unclear as to whether the TSA was an independent non-invasive neoplastic bystander, or an integral pre-cancerous remnant of the adenocarcinoma domain.
The vast majority of the dysplasias evolving in the Barrett's mucosa (BM) retain the flat (i.e. non-protuding) outline of the normal mucosa (1). Protruding BM dysplasias, also called adenomas, are very rare. In 1999, Thurberg, Duray and Odze (2) described five cases of adenomas in BM, and retrieved 12 additional cases from the literature. Since then, five new cases of adenomas in BM have been reported in humans (3-7) and one in a dog (8). Thus, 22 adenomas evolving in BM in humans are on record: 21 were tubular adenomas (2-6) and the remaining one, a villous adenoma (7).
Recently, we detected an adenocarcinoma in a patient with Barrett's esophagus. A biopsy obtained from a polypoid lesion, found at the margin of the tumour, revealed a traditional serrated adenoma (TSA).
The purpose of this communication is to report and illustrate this unique histological finding.
Case Report
Clinical data. A 68-year-old male with diabetes type-2, hyperlipidaemia, renal insufficiency requiring haemodialysis, hypertension, and myocardial infarction (2006), sought consultation in August 2012, for increasing dysphagia of three months' duration.
An endoscopic examination revealed a 26 cm-long Barrett's segment. Six cm proximal to the Z-line, a protruding tumor was found, measuring 3 cm in diameter, engaging approximately 75% of the esophageal circumference. On the tumour margin, a protruding lesion 4 mm in diameter was detected (Figure 1). Endosonography suggested an infiltrative carcinoma without signs of distant tumour. Because of severe co-morbidity, the patient was considered not suitable for primary surgery. At the time of writing this report, the patient is being treated with brachytherapy.
Histological findings. Biopsies obtained from the tumour revealed a moderately-differentiated adenocarcinoma. A biopsy taken from the protruding lesion at the tumor margin showed the presence of a TSA without invasive growth (Figure 2). This lesion exhibited hyperplastic fronds with saw-like indentations lined with dysplastic epithelium. Low-grade dysplasia was present in the upper part of the TSA (Figure 2). Other areas contained atypical mitotic figures (9) (Figure 3). The lower part of the TSA exhibited dysplastic cells and mitotic figures reaching the luminal border of the epithelium (Figure 4); these histological parameters were consistent with high-grade dysplasia.
Ki-67 immunostaining substantiated the identity of the non-invasive traditional serrated neoplasia, inasmuch as cell proliferation mostly occurred at the bottom of the dysplastic foveoli (10) (Figure 5).

Endoscopic view of a protruding lesion (arrow), at the margin of an irregular tumor with diffuse borders in a patient with Barrett's esophagus. The arrowed-protruding lesion was reported at histological examination as traditional serrated adenoma.
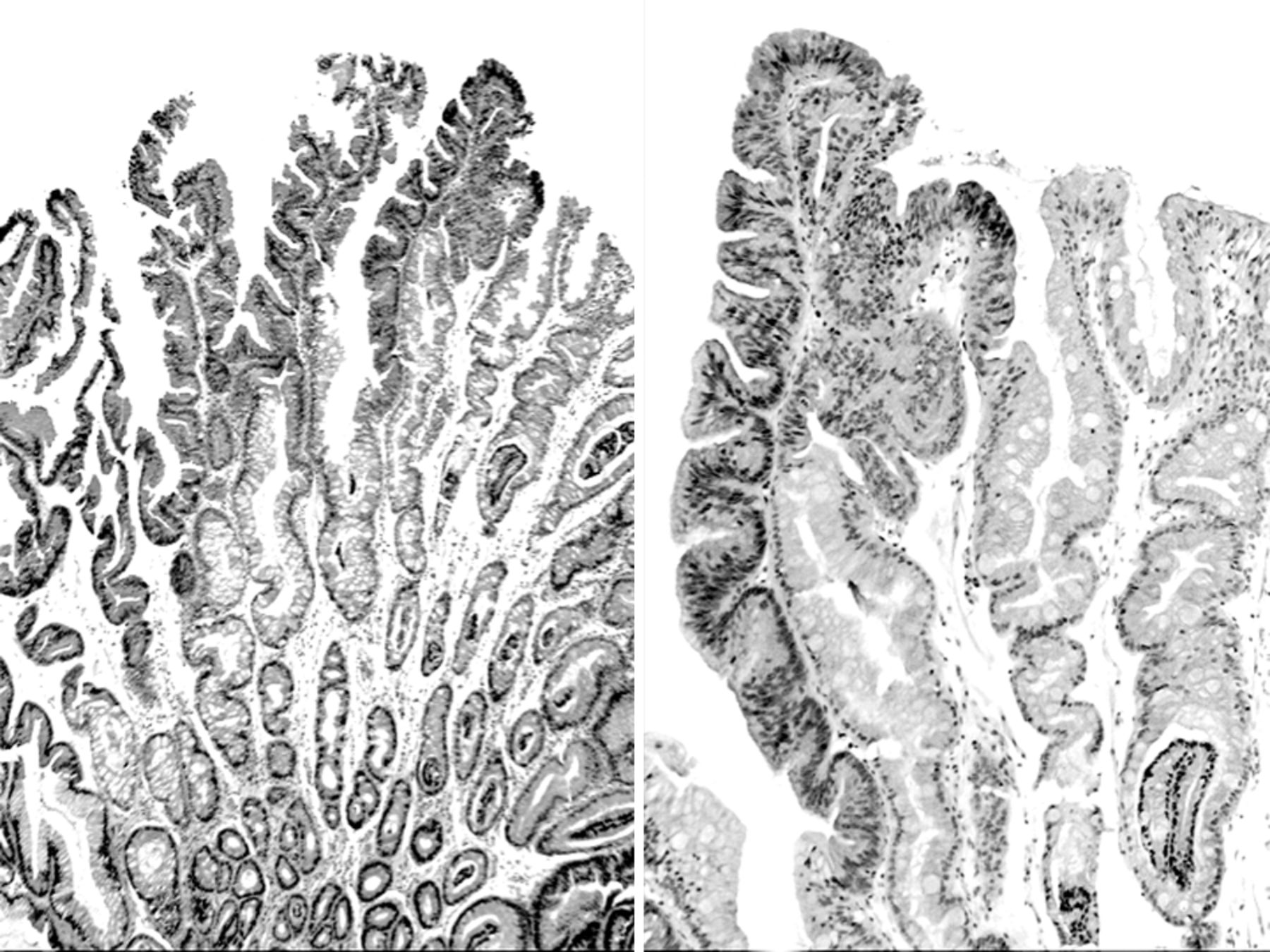
Left panel: Low power view of the traditional serrated adenoma (H&E, ×4). Right panel: Detailed view of the serrated epithelium with low-grade dysplasia (H&E, ×10).
In the subjacent non-dysplastic glands with intestinal metaplasia, the goblet cells contained mucopolysaccharides (periodic acid Schiff), and sialomucins (alcian blue pH 2.5).
Discussion
The review of the literature indicates that out of 22 adenomas evolving in BM, 21 were tubular adenomas (2-6) and the remaining one, a villous adenoma (7). Hence, ours appears to be the first case of TSA in BM in the literature.
We previously found TSA in other organs of the digestive tract: in the stomach (11), in the duodenum (12), in the pancreas (13), in the appendix (14), and in the colon and rectum, with and without ulcerative colitis (15-18).
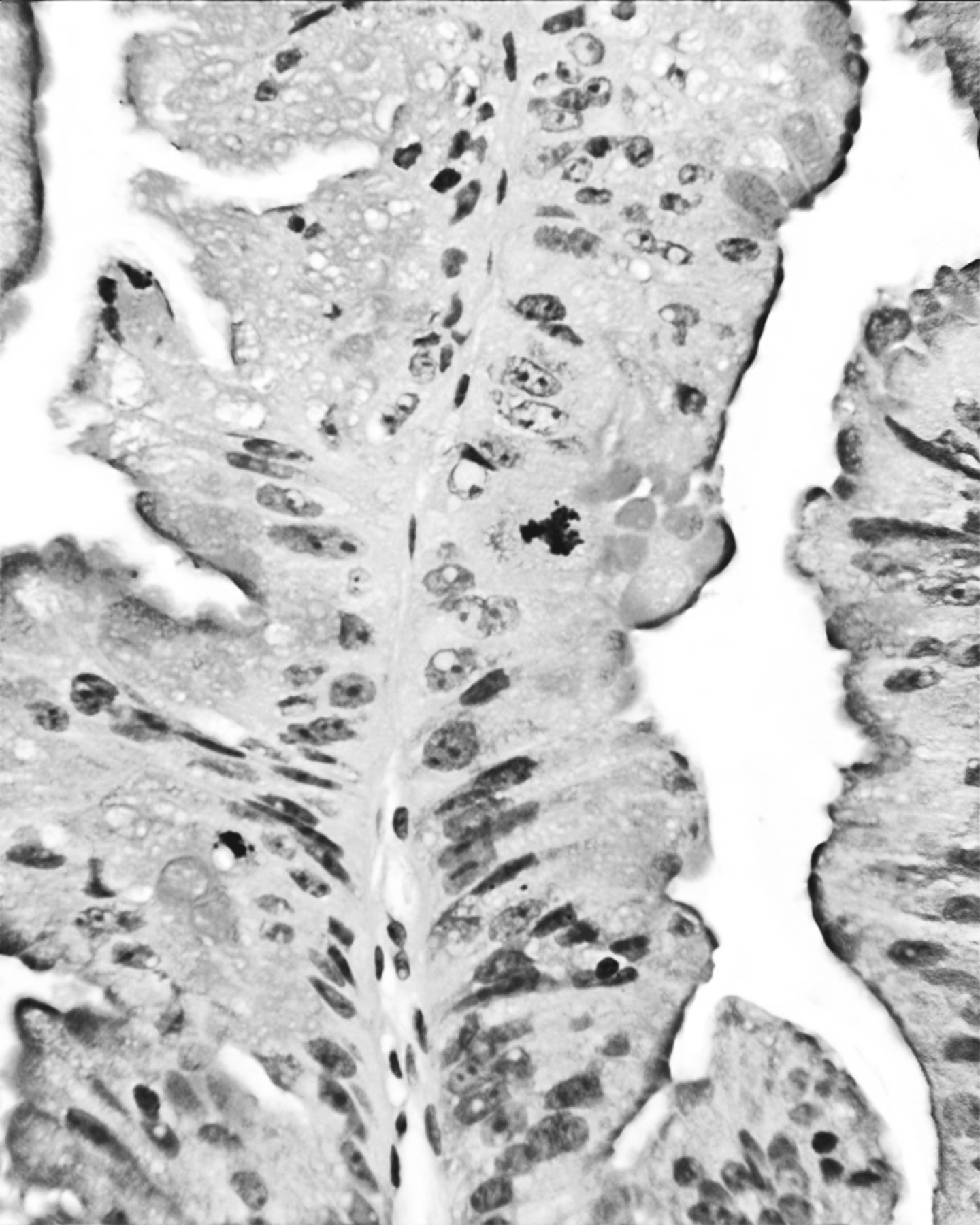
Traditional serrated adenoma, with a tripolar, atypical mitosis (periodic acid Schiff stain, ×40).
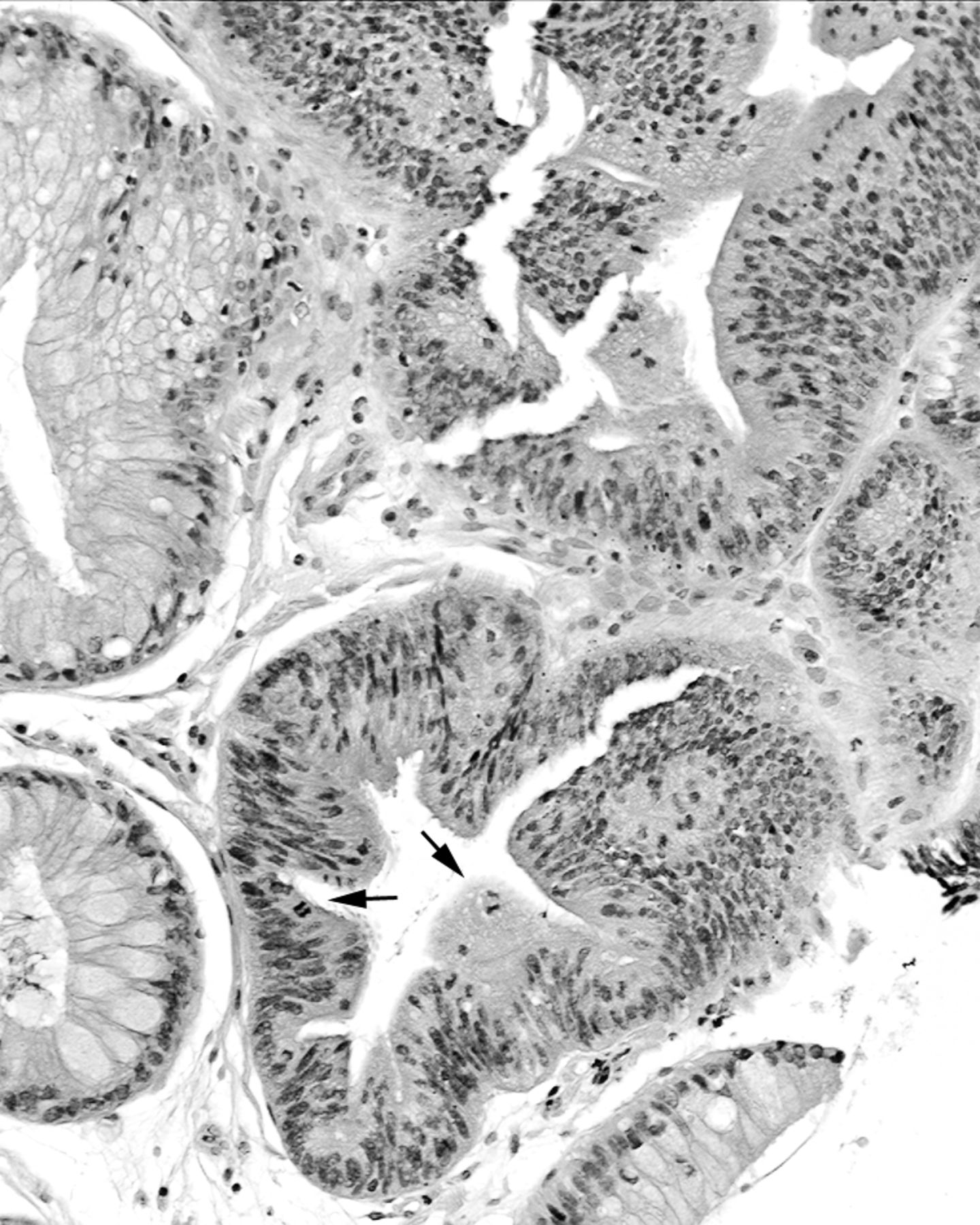
Base of traditional serrated adenoma. Note high-grade dysplasia with dysplastic cells and mitotic figures (arrows) reaching the luminal border of the epithelium (H&E ×20).
Years ago, Vogeltein et al. (19) reported a series of escalating molecular cytological aberrations evolving in colorectal tubular and villous adenomas, ranging from low-grade dysplasia to high-grade dysplasia and to invasive adenocarcinoma. TSAs were not included. In previous work, we found loss of heterozygosity (LOH) on 18q in colorectal TSA (20); this finding suggested a different genetic pathway between colorectal TSA on the one hand and colorectal tubular and villous adenomas on the other. The possibility that the same molecular pathway applied for the TSA of BM described here could not be explored.
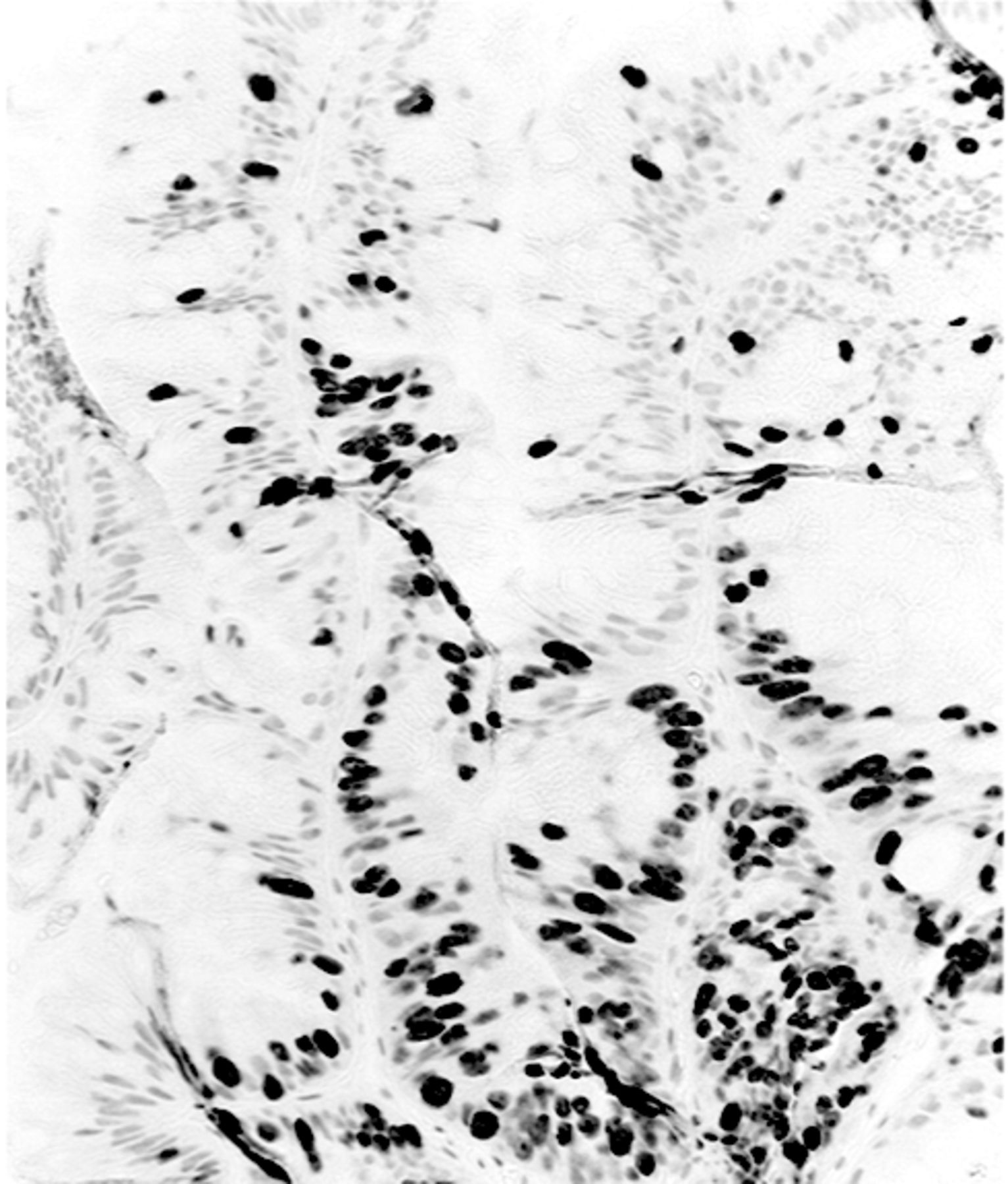
Traditional serrated adenoma, showing cell proliferation mainly at the base of the lesion (Ki-67, ×10).
In sum, the first case of TSA found at the border of an adenocarcinoma in a patient with Barrett's esophagus is presented. It remains unclear as to whether the TSA was an independent non-invasive bystander neoplastic lesion, or an integral pre-cancerous remnant of the adenocarcinoma domain.
- Received February 12, 2013.
- Revision received March 18, 2013.
- Accepted March 19, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}