


Abstract
Background: Postoperative infectious complications are associated with a poor long-term prognosis after resection of malignant tumors. We hypothesized that postoperative infectious complication such as surgical site infection (SSI) may have a negative impact on the outcome of elective hepatic resection for colorectal liver metastases (CRLM), and that the Glasgow prognostic score (GPS), which reflects the systemic inflammatory response, might predict for such complications. Patients and Methods: The subjects of the study were 77 patients who underwent hepatic resection for CRLM between January 2000 and December 2009. We retrospectively investigated the relation between SSI and disease-free, as well as overall, survival. Moreover, we assessed the risk factors pertinent to SSI. Results: In multivariate analysis, having more than four lymph node metastases (p=0.015) was a significant predictor of disease-free survival, while significant predictors of overall survival were the presence of more than four lymph node metastases (p=0.001) and SSI (p=0.008). Moreover, bilobar distribution (p=0.026), intraoperative fresh-frozen plasma transfusion (p=0.036) and GPS 1 or 2 (p=0.023) were found to be independent risk factors for SSI. Conclusion: Development of SSI after elective hepatic resection is associated with worse long-term outcomes in patients with CRLM. The GPS may be useful for preoperative risk stratification of SSI in such patients.
- Colorectal liver metastases
- surgical site infection
- Glasgow prognostic score
- systemic inflammatory response
Hepatic resection is the most effective and potentially curative therapy for liver metastases from colorectal cancer (CRLM), with a reported 5-year survival of 30 to 50% (1-3). In spite of improvements in surgical techniques, instruments, and perioperative management, morbidity in such patients remains high, ranging from 15% to 35% (2-6). Postoperative morbidity is associated with increased length of hospitalization and greater economic cost (7). Recent data suggest that postoperative complications are also associated with poor overall and cancer-specific survival after resection of various types of cancer (8, 9), including primary colorectal cancer (10, 11) and CRLM (4, 12-14). Therefore, it is important for te management of patients with CRLM to be able to predict the development of postoperative complications.
There are few reports on prediction of infectious complications by preoperative systemic response (15, 18). Recently, several studies have indicated that the measurement of systemic inflammatory response using the combination of serum C-reactive protein (CRP) and albumin concentrations before surgery or chemotherapy, i.e. the Glasgow prognostic score (GPS), predicts cancer-specific survival for patients with a variety of common solid tumors (16, 17), and postoperative infectious complications in primary colorectal cancer (18). The GPS is simple, and may predict for postoperative infectious complications. However, to the best of our knowledge, the relationship between the GPS and postoperative infectious complications in patients with CRLM has not been previously reported.
Therefore, we hypothesized that a postoperative infectious complication such as surgical site infection (SSI), may have a negative impact on the outcome of elective hepatic resection for CRLM, and that the systemic inflammatory response represented by the GPS might predict for postoperative infectious complications.
Patients and Methods
Between January 2000 and December 2009, 82 patients with CRLM underwent hepatic resection at the Department of Surgery, Jikei University Hospital, Tokyo, Japan. Out of these, five patients were excluded, one patient due to death from a cardiovascular event, and four patients who were lost to follow-up, leaving the remaining 77 patients for this study. All patients underwent macroscopic curative resection for liver, lung and lymph node metastases. Generally, the extent of hepatic resection was determined based on the retention rate of indocyanine green at 15 min (ICGR15) before surgery and hepatic reserve, as described by Miyagawa et al. (19). The type of resection was classified into two groups: anatomical resection (extended lobectomy, lobectomy, segmentectomy, or subsegmentectomy) and non-anatomical limited partial resection.
Patients' characteristics.
The chemistry profile was routinely measured for each patient preoperatively. Serum biochemistry profile data included serum albumin, CRP, and carcinoembryonic antigen (CEA). Use of blood products and dose were determined by the preference of attending surgeons based on guidelines for administration of blood products by the Japanese Ministry of Health and Welfare established in 1999 (20), as well as intraoperative blood loss, postoperative data for hemoglobin, platelets, serum albumin, and prothrombin time.
For the assessment of systemic inflammatory response using the GPS, the GPS was estimated as described previously (15-18): patients with normal albumin (≥35 g/l) and normal CRP level (≤10 mg/l) as GPS 0; those with low albumin (<35 g/l) or elevated CRP level (>10 mg/l) as GPS 1; and those with both low albumin (<35 g/l) and elevated CRP level (>10 mg/l) as GPS 2.
Firstly, we investigated the relation between clinical variables and disease-free and overall survival after hepatic resection by univariate and multivariate analyses. The factors consisted of the following 16 variables: age; gender; number of regional lymph node metastases from primary colorectal cancer; status of preoperative chemotherapy; synchronous/metachronous CRLM; number of tumors; tumor distribution; preoperative serum CEA level; type of resection; presence/absence of combined resection of primary tumor and CRLM; intraoperative transfusion of red blood cell concentrate (RCC); fresh-frozen plasma (FFP); platelet concentrate (PC); or albumin product; GPS (0 or 1/2); and SSI. Clinical continuous variables were classified into two groups for the log-rank test and the Cox proportional hazard regression model as follows: age <60 or ≥60 years, number of lymph node metastases <4 or ≥4, serum CEA <20 or ≥20 ng/ml.
Univariate analysis of disease-free and overall survival after hepatic resection.
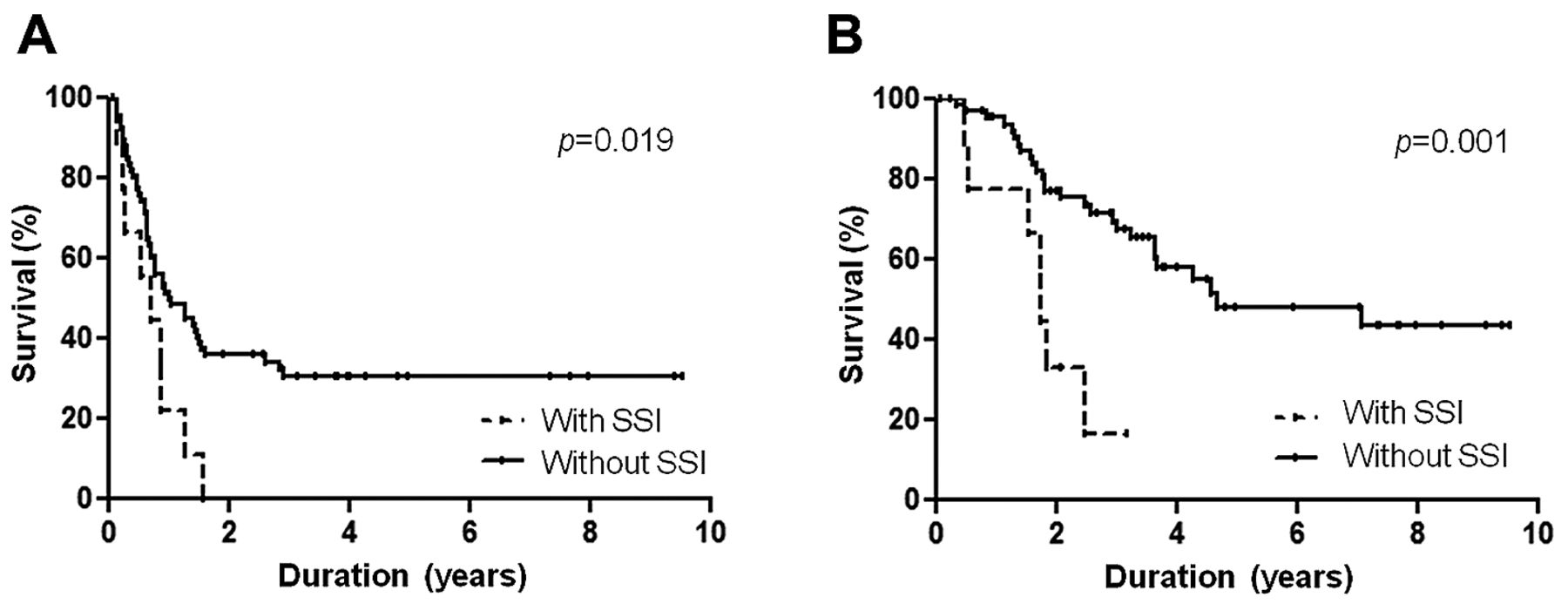
Kaplan-Meier curves for disease-free (A) and overall (B) survival in patients with and without SSI. Patients with SSI had significantly worse disease-free (p=0.019) and overall survival (p=0.001).
Next, to assess the risk factors for SSI, we investigated the relation between clinical variables and SSI after hepatic resection by univariate and multivariate analyses. The factors consisted of the following 17 variables: age; gender; body-mass index (BMI); presence/absence of diabetes mellitus; presence/absence of preoperative chemotherapy; synchronous/metachronous CRLM; number of tumors; tumor distribution; type of resection; presence/absence of combined resection of primary tumor and CRLM; duration of operation; intraoperative blood loss; intraoperative transfusion of RCC, FFP, PC, or albumin product; and GPS (0 or 1/2).
Recurrence of colorectal cancer was defined as newly-detected local, hepatic, lung or extrahepatic tumors by ultrasonogaphy, computed tomography, or magnetic resonance image with or without increase in serum CEA or carbohydrate antigen 19-9 (CA 19-9). For recurrent liver metastasis, repeated hepatic resection, local ablation therapy, or systemic chemotherapy were performed based mainly on the number, size and location of the recurrent liver tumors, as well as on hepatic functional reserve including ICGR15, and the remnant liver volume. For lung metastasis, limited partial lung resection or systemic chemotherapy was performed. For local recurrence, tumor resection, radiotherapy, or systemic chemotherapy was performed. 5-fluorouracil (5-FU)-based chemotherapy was chosen as adjuvant and/or neo-adjuvant chemotherapy prior to 2003. Since 2004, patients received infusional 5-FU/1-leucovorin with oxaliplatin (FOLFOX), and/or infusional 5-FU/1-leucovorin with irinotecan (FOLFIRI).
SSI was defined as surgical wound infection with purulent discharge and bacterial isolation, or intra-abdominal organ/space infection with pyrexia or purulent discharge.
This retrospective study was approved by the Ethics Committee of The Jikei University School of Medicine (#21-121).
Statistical analysis. Data are expressed as the mean±standard deviation (SD). Analysis of disease-free and overall survival was performed using the log-rank test. Univariate analysis was performed using the Mann-Whitney U-test and Chi-square test. Multivariate analysis was performed using the Cox proportional regression model and logistic regression analysis, incorporating all variables with p<0.05 on univariate analysis. All p-values were considered statistically significant when the associated probability was less than 0.05. These analyses were conducted using IBM® SPSS statistics version 20.0 (IBM Japan, Tokyo, Japan).
Results
Patients' characteristics. Patients' characteristics are listed in Table I. SSI developed in 10 out of 77 patients (13%). Out of these, four patients developed surgical wound infection and six patients developed intra-abdominal organ/space infection. Moreover, 65 patients were scored as GPS 0, nine patients as GPS 1, and three patients as GPS 2.
Univariate and multivariate analysis of disease-free and overall survival after hepatic resection according to clinical variables. Table II lists the relationship between the clinical variables and disease-free as well as overall survival after hepatic resection. In univariate analysis, disease-free survival was worse in patients with more than four lymph node metastases (p=0.008), bilobar distribution (p=0.002), combined resection of primary tumor and CRLM (p=0.041) and postoperative SSI (p=0.019, Figure 1A). Patients with preoperative chemotherapy (p=0.059) and multiple CRLM (p=0.065) tended to have worse disease-free survival, but not significantly. Overall survival was worse in patients with more than four lymph node metastases (p<0.001), multiple CRLM (p=0.004), bilobar distribution (p=0.018) and postoperative SSI (p=0.001, Figure 1B). Patients with preoperative chemotherapy tended to have worse disease-free survival, but not significantly (p=0.083).
In multivariate analysis, more than four lymph node metastases (p=0.015) was an independent and significant predictor of disease-free survival (Table III). For overall survival, more than four lymph node metastases (p=0.001) and postoperative SSI (p=0.008) were independent and significant predictors (Table IV).
Multivariate analysis of disease-free survival after hepatic resection.
Multivariate analysis of overall survival after hepatic resection.
Univariate and multivariate analysis of clinical variables and SSI after hepatic resection. Table V lists the relationship between clinical variables and SSI after hepatic resection of CRLM. In univariate analysis, BMI ≥25 (p=0.013), bilobar distribution (p=0.046), combined resection of primary tumor and CRLM (p=0.022) and GPS 1 or 2 (p=0.022) were significant risk factors for SSI. Intraoperative FFP transfusion showed a trend towards correlation with development of SSI (p=0.079). In multivariate analysis, bilobar distribution (p=0.026), intraoperative FFP transfusion (p=0.036) and GPS 1 or 2 (p=0.023) were found to be independent risk factors for the development of SSI (Table VI).
Discussion
SSI is the most common postoperative complication in surgical patients, which increases both hospital stay and treatment costs (7). In addition, several investigators reported that postoperative infectious complications, including surgical wound infection, abdominal abscess, lower-respiratory tract infection and generalized sepsis, influenced long-term outcomes in patients with CRLM (14, 15). Major surgery elicits a degree of systemic inflammation and immunosuppression in patients (21). Several studies confirmed that infection is associated with excessive and sustained levels of pro-inflammatory cytokine release including those of interleukin (IL)-1 IL-6, IL-8 and tumor necrosis factor-alpha (22, 23). High levels of IL-6 reduce the number, development and regulatory function of cytotoxic T-lymphocytes, natural killer cells and dendritic antigen-presenting cells, and this combination has been reported to be associated with poor prognosis in cancer patients (24, 25). Infectious complication leads to an extended period of inflammation and immunosuppression (26), which may contribute to metastatic proliferation (27). In addition to immunosuppression, tumor-cell stimulatory effects may be considered. Wound infection and inflammation activates granulocytes, which contribute to continuous angiogenic stimulation such as the one of releasing endothelial growth factor (28). This condition may accelerate the growth of residual cancer cells or micrometastases (29). In the present study, overall survival of patients with SSI after elective hepatic resection for CRLM was significantly worse, and disease-free survival of such patients tended to be worse, as shown by statistical analyses, which was in accordance with the previous studies (14, 15). These findings suggest that growth of a recurrent tumor is more rapid in patients with SSI than in those without SSI, because of the immunosuppressive state caused by SSI. Moreover, intra-operative blood transfusion has been reported to prolong hospital stay and increase complications by immunosuppressive effect (14, 26, 30). In the present study, intraoperative FFP transfusion and bilobar distribution also increased the risk of developing SSI, which was in accordance with a previous study (14).
The GPS was first reported as a predictor of prognosis in inoperable non-small cell lung cancer in 2003 (31). GPS was shown to predict for prognosis in patients with not only inoperable cancer (32-34) but also operable cancer, such as colorectal, gastroesophageal and pancreatic cancer (35-37). However, for specific conditions of metastatic tumors, there have been few studies on the GPS in relation to postoperative therapeutic outcomes in patients with CRLM. Ishizuka et al. reported that the GPS was not able to predict the prognosis of patients with CRLM after hepatic resection (38). The discrepancy between CRLM and other tumors was explained by the fact that CRLM appears at an advanced stage of colorectal cancer, at which the mortality rate will be high irrespective of the GPS. In the present study, there was no significant association between the GPS and prognosis, but higher GPS score was one of the independent risk factors for SSI.
The reasons for the relation between the GPS, pre-treatment elevated CRP or low albumin concentrations, and postoperative complications in patients with malignancies remain unclear (18, 39). The systemic inflammatory response and hypoalbuminemia reflect the loss of lean tissue and protein, which suppresses immune function (40, 41). Preoperative elevation of CRP has been reported to be associated with reduced lymphocyte numbers (42) and an impaired T-lymphocyte response (43). In relation to myeloid cells, the ability of a cell to synthesize pro-inflammatory and anti-inflammatory mediators is affected by its previous state (44). Chronically activated phagocytes may demonstrate an inadequate response to infectious stressors in the postoperative period, resulting in an increased risk of perioperative infectious events.
Univariate analysis of clinical variables and surgical site infection after hepatic resection.
Risk stratification of postoperative infectious complications, and prevention of systemic inflammatory response may improve perioperative outcomes and long-term survival after resection of malignant tumors. Several therapeutic agents targeting the inflammatory response are undergoing clinical trials (45). Further investigation to clarify the relationship between immunosuppressive mechanisms caused by systemic inflammation and tumor progression is important to improve the therapeutic outcome.
Conclusion
Development of SSI after elective hepatic resection is associated with worse long-term outcomes in patients with CRLM. Risk stratification for SSI and careful management in the perioperative period for reduction of the incidence of SSI may be important to improve the long-term therapeutic outcome. GPS may be useful for preoperative risk stratification for SSI.
Multivariate analysis of clinical variables and surgical site infection after hepatic resection.
Footnotes
-
Conflicts of interest
The Authors declare that they have no conflicts of interest.
- Received January 28, 2013.
- Revision received March 5, 2013.
- Accepted March 5, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
Jump to section
Related Articles
Cited By...
- Risk Factors and Overcoming Strategies of Surgical Site Infection After Hepatectomy for Colorectal Liver Metastases
- Impact of surgical site infection (SSI) following gynaecological cancer surgery in the UK: a trainee-led multicentre audit and service evaluation
- Negative Impact of Fresh-frozen Plasma Transfusion on Prognosis of Pancreatic Ductal Adenocarcinoma After Pancreatic Resection
- Negative Impact of Fresh-frozen Plasma Transfusion on Prognosis after Hepatic Resection for Liver Metastases from Colorectal Cancer