


Abstract
Background: Little is known about the prognostic value and clinical significance of monitoring tumour status using tumour markers in patients with recurrent gastric cancer. Patients and Methods: Between 2002 and 2009, 91 consecutive patients exhibited recurrence after curative gastrectomy for gastric cancer. They were followed intensively using tumour markers such as CA19-9 and CEA and their records were retrospectively analyzed. Results: At the time of recurrence, patients were divided into three groups. Each tumour marker was re-elevated in 45 patients (51%) (re-elevation group: REG), was continuously-elevated since initial surgery in 23 patients (25%) (continuous elevation group: CEG) and was not elevated in 22 patients (24%) (non-elevation group: NEG). Survival after recurrence in REG was significantly better than in the other groups. In particular, those in REG had significantly better outcomes than those in NEG, in both survival after recurrence (p=0.0109) and total postoperative survival (p=0.0197), although there were no significant differences in recurrence-free survival between the two groups (p=0.8818). REG patients were able to receive more chemotherapy regimens than NEG patients (p=0.0730, REG vs. NEG, first-line 43% vs. 68%, second-line 33% vs. 32%, third-line or more 24% vs. 0%). Multivariate analysis revealed that re-elevations in tumour markers were found to be an independent prognostic factor for survival after recurrence [p=0.0014, hazard ratio=2.55 (95% CI: 1.45-4.65)]. Particularly for peritoneal recurrence, those in REG had significantly better outcomes than those in NEG (p<0.0005). Conclusion: Monitoring tumour dynamics using tumour markers may facilitate clinical decision-making, according to changes in tumour markers and contribute to survival prolongation in patients with recurrent gastric cancer.
Gastric cancer is one of the most common causes of death from cancer worldwide (1). Recent advances in diagnostic methods, less invasive treatment techniques and perioperative management have increased the early detection of gastric cancer and reduced mortality and morbidity rates (2-4). However, even if curative gastrectomy is performed, all patients have the potential risk of disease recurrence. Indeed, 40-60% of patients with locally-advanced cancer experience recurrence after surgery (5, 6). Therefore, to improve survival rates for patients with gastric cancer, recurrent disease must be diagnosed when it is still minimal or clinically-occult and an appropriate treatment strategy should be performed with consideration for its efficacy.
We hypothesized that monitoring tumour dynamics with tumour markers could contribute to survival prolongation whether early-detection was made or not because such monitoring may be helpful in the decision-making for selecting better timing of detailed examinations and in changing chemotherapy accordingly while the patient's performance status allows for additional treatments.
In this study, we investigated whether the tumour marker CEA and CA19-9 was useful for monitoring tumour status after recurrence and contributed to better outcomes. Our results might show that monitoring tumour dynamics using sensitive tumour markers enable us to select better chemotherapeutic regimens earlier according to changes in tumour markers and contribute to survival prolongation of recurrent gastric cancer patients to a clinically-satisfactory degree.
Patients and Methods
Patients. Between 2002 and 2009, 91 consecutive patients, who exhibited recurrence following curative gastrectomy (R0) for gastric cancer and had been treated in the Department of Digestive Surgery, Kyoto Prefectural University of Medicine, were retrospectively analyzed from hospital records. Curative resection was performed as sub-total or total gastrectomy according to the location of tumour for a secure sufficient tumour-free resection margin and radical lymphadenectomy was performed according to the Japanese Gastric Cancer Treatment Guidelines (7). Resected specimens were examined by pathologists based on classifications of the 14th Japanese Classification of Gastric Carcinomas (JCGC) (8) and 7th Tumour-Node-Metastasis (TNM) (9). The clinicopathological findings of these patients were determined retrospectively on the basis of their hospital records. Histological types were classified as differentiated (papillary, moderately and well-differentiated adenocarcinoma) and undifferentiated (poorly, undifferentiated, signet-ring cell carcinoma, and mucinous adenocarcinoma) based on the 14th JCGC.
Postoperative adjuvant chemotherapy using oral fluoropyrimidine S-1-based regimens with no radiation therapy was performed for patients with tumours of more than pathological stage II (10, 11). The follow-up program scheduled for all patients comprised a regular physical examination and laboratory blood tests including tumour marker CEA and CA19-9, chest X-rays every three months in the first postoperative year, every six months in the second postoperative year, and annually thereafter for at least five years. Computed tomography (CT) was performed annually for patients with pathological stage I-II tumours and every six months for patients with tumours of more than pathological stage III for the first five years. Otherwise, CT was performed within one month when tumour marker elevation or symptoms were detected in follow-up laboratory blood tests and regular physical examinations. Endoscopy was performed for all patients annually to screen for cancer in the gastric remnant.
The patterns of recurrence were classified as peritoneal, haematogenous, lymphatic and locoregional, and multiple recurrences. Peritoneal recurrences included positive cytology in the ascitic fluid, carcinomatosis, or ovarian metastasis. Haematogenous recurrences were defined as organic metastases including the liver, lung, and bone. Lymphatic and locoregional recurrences were in the regional and/or distant lymph nodes and gastric bed, and remnant gastric cancer at the anastomotic site or gastric stump. Multiple recurrences were defined as having multiple patterns of recurrence. Recurrences were categorized by the site at initial presentation. First-line and second-line, third-line or more chemotherapies for recurrence were performed using oral fluoropyrimidine S-1, 5-FU, cisplatin, taxane, irinotecan, and their combinations.
In this study, patients were categorized into three groups according to the pattern of change of either or both tumour markers at the time of recurrence as follows: non-elevation group, re-elevation group, and continuous elevation group. The elevation of tumour markers was defined that data of each or both tumour markers was beyond the degree of normal limit in blood laboratory test. In the non-elevation group, tumour markers were not elevated after initial surgery and were also not elevated at the time of recurrence. In the re-elevation group, tumour markers were not elevated after initial surgery but became elevated at the time of recurrence. In the continuous elevation group, tumour markers were elevated before and after initial surgery and were also continuously elevated at the time of recurrence. During follow-up after initial surgery or chemotherapy for recurrence, if tumor marker elevation was detected, prompt detailed examinations using imaging modalities such as CT and PET were normally performed.
Statistical analysis. The chi-square test and Fisher's exact probability test were performed for categorical variables, while the Student's t-test and Mann-Whitney U-test for unpaired data of continuous variables were performed to compare clinicopathological characteristics between groups. Cause-specific death was recorded when the cause of death was specified as recurrent gastric cancer. Post-recurrence survival at the time from recurrence to death, and overall survival at the time from curative gastrectomy to death were estimated using the Kaplan-Meier method, and the log-rank test was used to assess differences between clinical factors. A p-value of less than 0.05 was considered significant.
Results
Comparison of survival curves according to changing patterns of tumour marker changes in patients with recurrent gastric cancer. Between 2002 and 2009, 91 consecutive patients exhibited tumour recurrence following gastrectomy for gastric cancer. Out of all 91 patients analyzed, 46 (51%), 23 (25%), and 22 (24%) were assigned to the re-elevation group, the continuous-elevation group, and the non-elevation group, respectively. The median survival time (MST) after recurrence for the re-elevation group was the longest among these groups; re-elevation vs. continuous elevation vs. non-elevation: 244 days vs. 128 days vs. 93 days) (Figure 1A). In further analyses, the continuous-elevation group was excluded because it could not be fully determined whether residual tumour or recurrence was associated with the continuous elevation of tumour markers.
The re-elevation group had significantly better outcomes than the non-elevation group in both survival after recurrence (p=0.0109) (Figure 1B) and total postoperative survival (p=0.0197) (Figure 1D), although there were no significant differences in recurrence-free survival between the groups (p=0.8818) (Figure 1C). There are also no significant differences in clinicopathological factors between both groups (Table I). There may be a prognostic benefit of measuring these tumour markers in patients in the re-elevation group for survival after recurrence for gastric cancer.
Comparison of the time-course of chemotherapy and MST after recurrence between non-elevation and re-elevation groups. To investigate reasons for the prognostic difference between the re-elevation group and non-elevation group, we compared the time-course of chemotherapy in 68 consecutive patients in these groups. As a result, the frequency of patients treated with second-line chemotherapy or more, after recurrence tended to be higher in the re-elevation group than that in the non-elevation group (p=0.0730) (Figure 2). Namely, in the re-elevation group, 20 patients were treated with adjuvant chemotherapy-only or first-line chemotherapy (43%; MST after recurrence=240 days), 15 patients were treated with second-line chemotherapy (33%; MST after recurrence=186 days) and 11 patients were treated with third-line chemotherapy (24%; MST after recurrence=335 days). However, in the non-elevation group, 15 patients were treated with adjuvant chemotherapy or first-line chemotherapy (68%; MST after recurrence=93 days), 7 patients were treated with second-line chemotherapy (32%; MST after recurrence=79 days) and no patient were treated with third-line chemotherapy (0%) (Figure 2).

The median survival time after recurrence of gastric cancer in the re-elevation group was the longest among all groups; re-elevation vs. continuous elevation vs. non-elevation: 244 days vs. 128 days vs. 93 days) (A). The re-elevation group had significantly better outcomes than the non-elevation group in both survival after recurrence (p=0.0109) (B) and total postoperative survival (p=0.0197) (D), although there were no significant differences in recurrence-free survival between the groups (p=0.8818) (C).
Univariate and multivariate analyses of survival after recurrence using Cox's proportional hazard model. In order to determine prognostic independence of re-elevation of tumour markers, we performed univariate and multivariate analyses of survival after recurrence using the Cox's proportional hazard model. Consequently, univariate analysis showed that greater age and the re-elevation of tumour markers were significant prognostic factors for reduced cause-specific survival after recurrence. Multivariate analysis demonstrated that along with T-stage and tumour size, re-elevation of tumour markers was an independent prognostic factor (Table II).
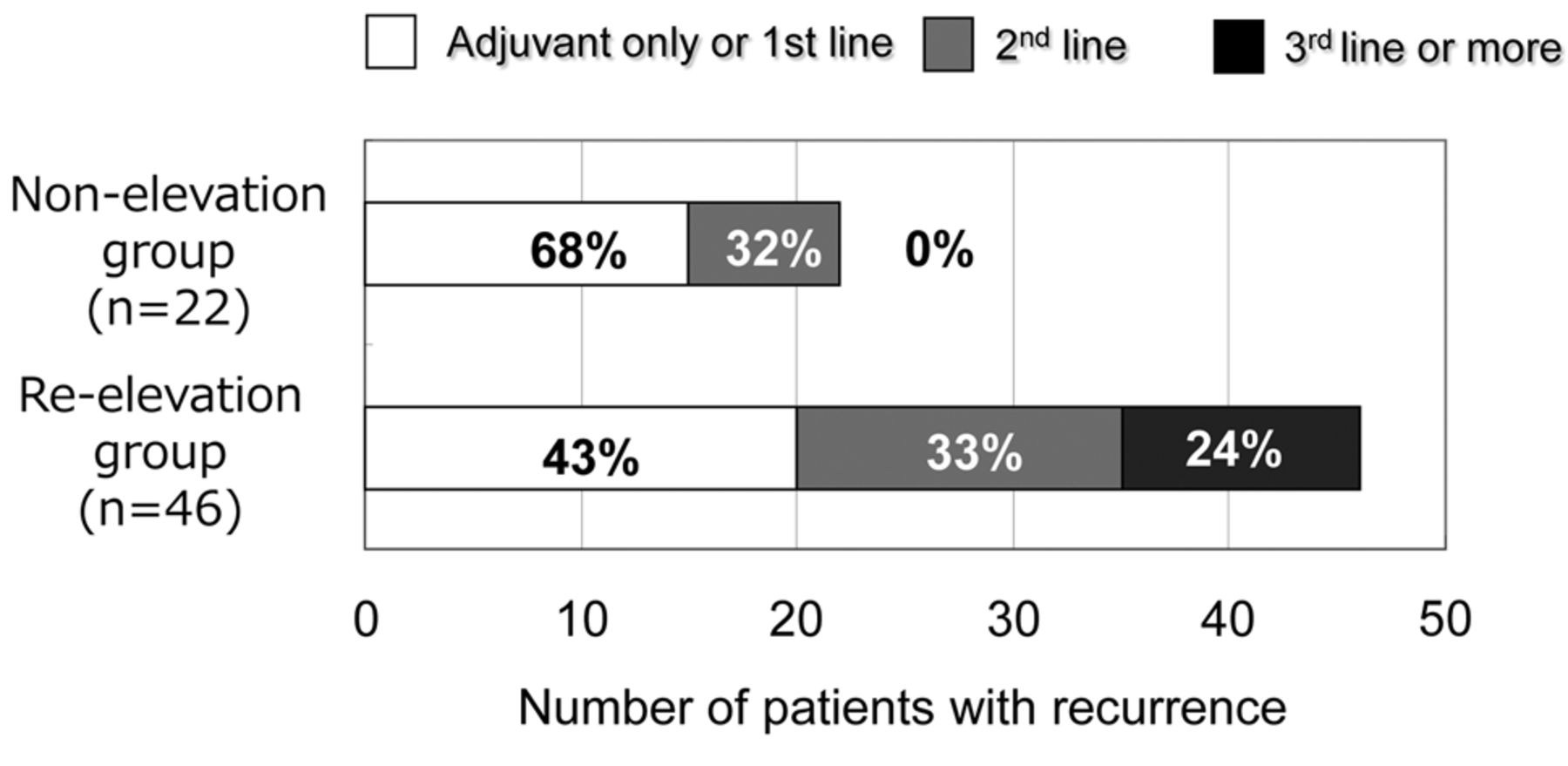
The frequency of patients treated with second-line chemotherapy or more after recurrence tended to be higher in the re-elevation group than that in the non-elevation group (p=0.0730).
Comparison of survival curves after recurrences according to the type of recurrence. Furthermore, we investigated which type of recurrence was more associated with favourable outcomes in patients with the re-elevation of tumour markers (Figure 3). As a result, particularly for peritoneal recurrence, the re-elevation group had significantly better outcomes than the non-elevation group (p=0.0020). In contrast, other types of recurrence were not prognostically different between the re-elevation group and non-elevation group (p=0.4317) (Figure 3). In addition, especially for patients with peritoneal recurrence, the number of patients treated with second-line or more chemotherapy after recurrence was higher in the re-elevation group than that in the non-elevation group. Namely, in the re-elevation group, 7 patients were treated with adjuvant chemotherapy or first-line chemotherapy (41%; MST after recurrence=220 days), 8 patients were treated with second-line chemotherapy (47%; MST after recurrence=329 days) and 2 patients were treated with third-line chemotherapy (12%; MST after recurrence=399 days). However, in the non-elevation group, 7 patients were treated with first-line chemotherapy (70%; MST after recurrence=132 days), 3 patients were treated with second-line chemotherapy (30%; MST after recurrence=79 days) and no patients were treated with third-line chemotherapy (0%) (Figure not shown).
Association between clinicopathological characteristics and tumour marker elevations.
Discussion
Monitoring tumour dynamics after recurrence with tumour markers may prompt detailed examinations according to the changes in tumour markers and allow for switching of chemotherapy from an ineffective regimen to other more promising regimens. In this study, we demonstrated that monitoring tumour dynamics using CEA and CA19-9 may facilitate clinical decision-making and contribute to survival prolongation in patients with recurrent gastric cancer.
To our knowledge, however, no report has yet provided evidence that monitoring tumour dynamics with such markers contributes to survival prolongation in gastric cancer. One possible reason may be that there had not been any effective or high-quality regimens of chemotherapy for recurrent gastric cancer achieving survival prolongation, only curative resection of recurrent tumours. However, several recent prospective randomized control trials such as JCOG9912 (Randomized phase-III study of 5-fluorouracil-alone versus combination of irinotecan and cisplatin versus S-1 alone in advanced gastric cancer. Japan Clinical Oncology Group 9912), SPIRITS (S-1 Plus cisplatin versus S-1 in RCT in the treatment for Stomach cancer), ToGA (Trastuzumab for Gastric Cancer), and START (S-1 and Taxotere for Advanced Gastric Cancer. Randomized Phase - III Trial) studies using newer agents showed survival benefits for advanced and recurrent gastric cancer in overall or sub-group analyses (12-15). Therefore, the significance of monitoring tumour dynamics using tumour markers in relation to treatment efficacy should be emphasized.
In this study, in order to elucidate prognostic effects using tumour marker dynamics, we analyzed data for 91 recent consecutive patients who underwent curative gastrectomy, and postoperative adjuvant chemotherapy such as 5-FU or oral fluoropyrimidine S-1-based regimens, if they were diagnosed with tumour of pathological stage II or higher. Moreover, we assigned all 91 patients into three groups based on tumour marker changes; obviously re-elevation of tumour markers at recurrence indicates the need to monitor subsequent treatment efficacy. Consequently, we showed that patients with tumour marker re-elevation at recurrence presented significantly better outcomes in both survival after recurrence and postoperative cause-specific survival than those of patients without elevation of tumour markers (Figure 1B and 1D). We also demonstrated that a re-elevation of tumour markers was an independent prognostic factor for better cause-specific survival after recurrence (Table II) and postoperative cause-specific survival (data not shown) by multivariate analysis.

Patients in the re-elevation group had significantly better outcomes than those in the non-elevation group with peritoneal recurrence (p=0.0020). In contrast, there were no significant differences in outcomes between the re-elevation group and non-elevation group for other types of recurrence (p=0.4317).
Univariate and multivariate analyses of survival after recurrence using the Cox's proportional hazard model.
Next, we examined the reasons for favourable prognostic effects in the re-elevation group. We investigated the background factors most associated reasons with survival, surveillance with tumour markers, and appropriate use and type of effective chemotherapy regimens with tumour markers after recurrence. As a result, there were no significant differences in background clinicopathological factors (Table I) and recurrence-free survival between the re-elevation and non-elevation groups (p=0.8818) (Figure 1B). These results could exclude the possibility of lead-time bias and the favourable outcome in the re-elevation group might not be associated with standard surveillance after initial surgery similarly to previous reports (16-20), but with the way of treatments using tumour makers after recurrence. Indeed, the frequency of patients treated with second-line chemotherapy or more after recurrence was tended to be higher in the re-elevation group than the non-elevation group (p=0.0730) (Figure 2). This suggests that monitoring tumour dynamics after recurrence using tumour markers contributes to the decision-making for selecting better chemotherapy regimens with better timing while the patient's performance status allows for switching to more effective treatments (17, 21).
We also found that patients with peritoneal recurrence in the re-elevation group had significantly better outcomes than those in the non-elevation group (p=0.0020). However, other types of recurrence had no significant effect on outcomes in these groups (p=0.4317) (Figure 3). These findings are in agreement with recent prospective randomized control trials such as ACTS-GC (Adjuvant Chemotherapy Trial of TS-1 for Gastric Cancer), SPIRITS and START studies using S-1-based regimens that found treatment sensitivity and survival benefits, particularly in non-measurable tumour recurrences such as peritoneal recurrence (11, 13, 15). In this study, patients were treated mainly with S-1-based regimens, similarly to the clinical trials described above. Therefore, our results strongly suggest that the survival effect of monitoring tumour dynamics with tumour makers might be enhanced by S-1-based chemotherapy, particular in peritoneal recurrence. Indeed, evaluation of treatment efficacy on peritoneal recurrence is difficult even if imaging tests such as CT and PET were performed. These findings might contribute to clinical decision-making in clinical practice.
We present here a framework of the significance of monitoring the tumour status of recurrence with tumour biomarkers. As far as we are aware, this study is the first report to provide evidence that monitoring biomarkers, even if they are only conventional tumour markers, may lead to favourable outcomes in recurrent gastric cancer. However, many issues should be addressed before these findings can be translated into a clinically useful strategy for advanced gastric cancer treatments, because there are still no similar reports and few tumour-specific biomarkers for use in clinical settings. Conventional serum tumour markers such as CEA and CA19-9 are useful to monitor tumour status following chemotherapy but lack a sufficient sensitivity and specificity to facilitate early detection and monitoring of cancer (22-24). Therefore, detecting novel biomarkers such as molecular biomarkers using a less invasive blood-based diagnostic assay is required, as shown in recent reports (25-28). If more patients with recurrence could be followed by a sensitive ‘tailor-made biomarker’ for each individual, these biomarkers may also contribute to improving survival rates for more patients with gastric cancer. At our Institute, these issues are currently under evaluation to detect novel biomarkers, including circulating cancer-associated nucleic acids such as cell-free DNA and microRNAs in plasma and serum (29-34). In conclusion, our results provide evidence that monitoring tumour dynamics using tumour markers may facilitate an early clinical decision-making and contribute to survival prolongation in patients with recurrent gastric cancer.
- Received February 3, 2013.
- Revision received March 15, 2013.
- Accepted March 15, 2013.
- Copyright© 2013 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.